Introduction
The response rates to neoadjuvant chemotherapy (NAC)
in patients with locally advanced breast cancer (LABC) are 40–60%.
The drawbacks of this treatment method are that certain patients
may experience adverse effects and that it may cause unnecessary
delay to surgical treatment, particularly in the cases with
progressive disease. Therefore, biomarkers that predict response to
NAC may prove useful. The most important qualities for a biomarker
are that it may be assessed easily and at low cost, even in
hospitals that lack expensive laboratory equipment and advanced
molecular techniques. Previous studies demonstrated that gene
microarray technologies are able to predict response to NAC
(1,2). However, this advanced technique has
not been routinely applied in the clinical setting due to its high
cost, particularly in developing countries and low-income
areas.
An increasing number of studies investigate factors
[including survivin, Ki-67, estrogen-receptor (ER) tumor status and
tumor grade] that may predict response to either first- or
second-line chemotherapy. However, available data on the prediction
of the efficacy of third-line chemotherapeutic agents (i.e., those
including anthracyclines and either docetaxel or dose-dense weekly
paclitaxel) are limited. The aim of this study was to investigate
whether survivin, Ki-67, ER tumor status and tumor grade are useful
predictive biomarkers for the response of the primary tumor to NAC
with a docetaxel-based regimen.
We considered a regimen of 75 mg/m2
docetaxel, 60 mg/m2 pirarubicin and 500 mg/m2
cyclophosphamide (TAC) once every 3 weeks to be an effective option
for NAC in LABC, in order that more patients benefit from
undergoing breast conserving-surgery following treatment. Survivin
expression and high tumor grade were shown to be independent
predictors of response.
Materials and methods
Patients
Between January, 2009 and December, 2012, 71
patients with locally advanced (stage IIb and IIIb) breast cancer
were enrolled at Lianyungang First People's Hospital (Jiangu,
China). Eligible patients had core needle biopsy-confirmed breast
cancer, were previously untreated and had locally advanced tumors
that were potentially operable, without evidence of distant
metastasis (Table I). Three
patients did not complete the chemotherapy scheme due to the
development of leukopenia and asthenia.
 | Table IUnivariate analysis of the association
of baseline characteristics with ORR and pCR. |
Table I
Univariate analysis of the association
of baseline characteristics with ORR and pCR.
| Characteristics | No. | ORR | P-value | pCR | P-value |
|---|
| No. of patients | 68 | | | | |
| Median age, years
(range) | 45 (35–60) | | | | |
| Tumor diameter, mm
(range) | 45 (25–80) | | | | |
| Menopausal
status |
| Premenopausal | 32 | 81% (26/32) | 0.587a | 19% (6/32) | 0.724a |
| Postmenopausal | 36 | 86% (31/36) | | 22% (8/36) | |
| ECOG performance |
| 0 | 44 | 86% (38/44) | 0.670b | 23% (10/44) | 0.782b |
| 1 | 24 | 79% (19/24) | | 17% (4/24) | |
| Clinical nodal
status |
| Negative | 18 | 78% (14/18) | 0.661b | 17% (3/18) | 0.889b |
| Positive | 50 | 86% (43/50) | | 22% (11/50) | |
| Stage |
| II (T≥5 cm) | 30 | 80% (24/30) | 0.668b | 20% (6/30) | 0.915a |
| III | 38 | 87% (33/38) | | 21% (8/38) | |
| Survivin |
| Negative | 18 | 61% (11/18) | 0.0072c | 0% (0/18) | 0.0292a |
| Positive | 50 | 92% (46/50) | | 28 (14/50) | |
| Ki-67 |
| Negative | 16 | 63% (10/16) | 0.0242c | 0% (0/16) | 0.0482a |
| Positive | 52 | 90% (47/52) | | 27% (14/52) | |
|
Estrogen-receptor |
| Negative | 31 | 87% (27/31) | 0.502a | 29% (8/31) | 0.330a |
| Positive | 37 | 81% (30/37) | | 16% (6/37) | |
| No. of cycles |
| 4 | 39 | 85% (33/39) | 1.0b | 21% (8/39) | 0.986a |
| 5–6 | 29 | 83% (24/29) | | 21% (6/29) | |
| Tumor type |
| Invasive
ductal | 60 | 87% (52/60) | 0.218b | 25% (13/60) | 0.891b |
| Invasive
lobular | 8 | 63% (5/8) | | 13% (1/8) | |
| Tumor grade |
| I/II | 28 | 71% (20/28) | 0.0472c | 11% (3/28) | 0.092a |
| III | 40 | 93% (37/40) | | 28% (11/40) | |
| PgR |
| Negative | 37 | 28% (11/40) | 0.189a | 22% (8/37) | 0.818a |
| Positive | 31 | 77% (24/31) | | 19% (6/31) | |
| HER2 status |
| 0 to 1+ | 50 | 88% (44/50) | 0.236b | 24% (12/50) | 0.412b |
| 2+ to 3+ | 18 | 72% (13/18) | | 17% (2/18) | |
This study was conducted in accordance with the
ethics principles of the Declaration of Helsinki. The study methods
were approved by the Institutional Review Board of Lianyungang
First People's Hospital and patients provided written informed
consent prior to enrollment.
Treatment
Prior to treatment initiation, tumors were measured
by magnetic resonance imaging (MRI). Patients received the TAC
regime, administered every 3 weeks for 4–6 cycles. Patients were
administered dexamethasone premedication (8 mg orally every 12 h, 6
times, starting the day prior to treatment initiation) to prevent
docetaxel-related hypersensitivity and fluid retention. Primary
prophylaxis with granulocyte colony-stimulating factor (G-CSF) was
not permitted. However, in patients who developed episodes of
febrile neutropenia or infection, administration of G-CSF was
mandatory in the subsequent cycles. Approximately 2 weeks after
NAC, the patients underwent either breast-conserving surgery or
modified radical mastectomy. Following surgery, the patients
received chemotherapy, radiotherapy, endocrine therapy or a
combination of these treatments.
Treatment response
The clinical treatment response was assessed using
the Response Evaluation Criteria in Solid Tumors (RECIST) (3). The overall clinical response rate
(ORR) was defined as the complete and partial responses combined.
The pathological complete response (pCR) was assessed after
surgical resection of the remaining tumor and nodes and was defined
as the absence of tumor cells, absence of persistent in situ
disease and negative axillary lymph nodes. All samples were
assessed by two pathologists at Lianyungang First People's
Hospital.
Evaluation of survivin, Ki-67 and ER
tumor status
Core biopsy specimens were fixed in 10%
neutral-buffered formalin for 24 h prior to processing and embedded
in paraffin wax blocks at the pathology laboratory in our hospital.
Sections (3 mm) were cut from each block, mounted on
positively-charged slides and stained with hematoxylin and
eosin.
Prior to immunohistochemical analysis, the tissue
sections were deparaffinized and rehydrated in graded alcohols. The
slides were subjected to heat-induced epitope retrieval by
immersion in 0.01 M boiling citrate buffer (pH 6) in a pressure
cooker for 3 min, followed by a 20-min cooling period and overnight
incubation with monoclonal antibody [rabbit monoclonal
anti-survivin (1:100, cat no: Z2159; Reta Corporation, Deerfield
Beach, FL, USA), rabbit monoclonal anti-Ki-67 (1:100, cat no:
Z2031; Reta Corporation) and rabbit monoclonal anti-ER (1:200, cat
no: Z2021RS; Reta Corporation)]. Negative and positive control
slides were also prepared. Histological classification was
performed according to the WHO criteria and tumor grading was
performed according to the Elston and Ellis criteria (4).
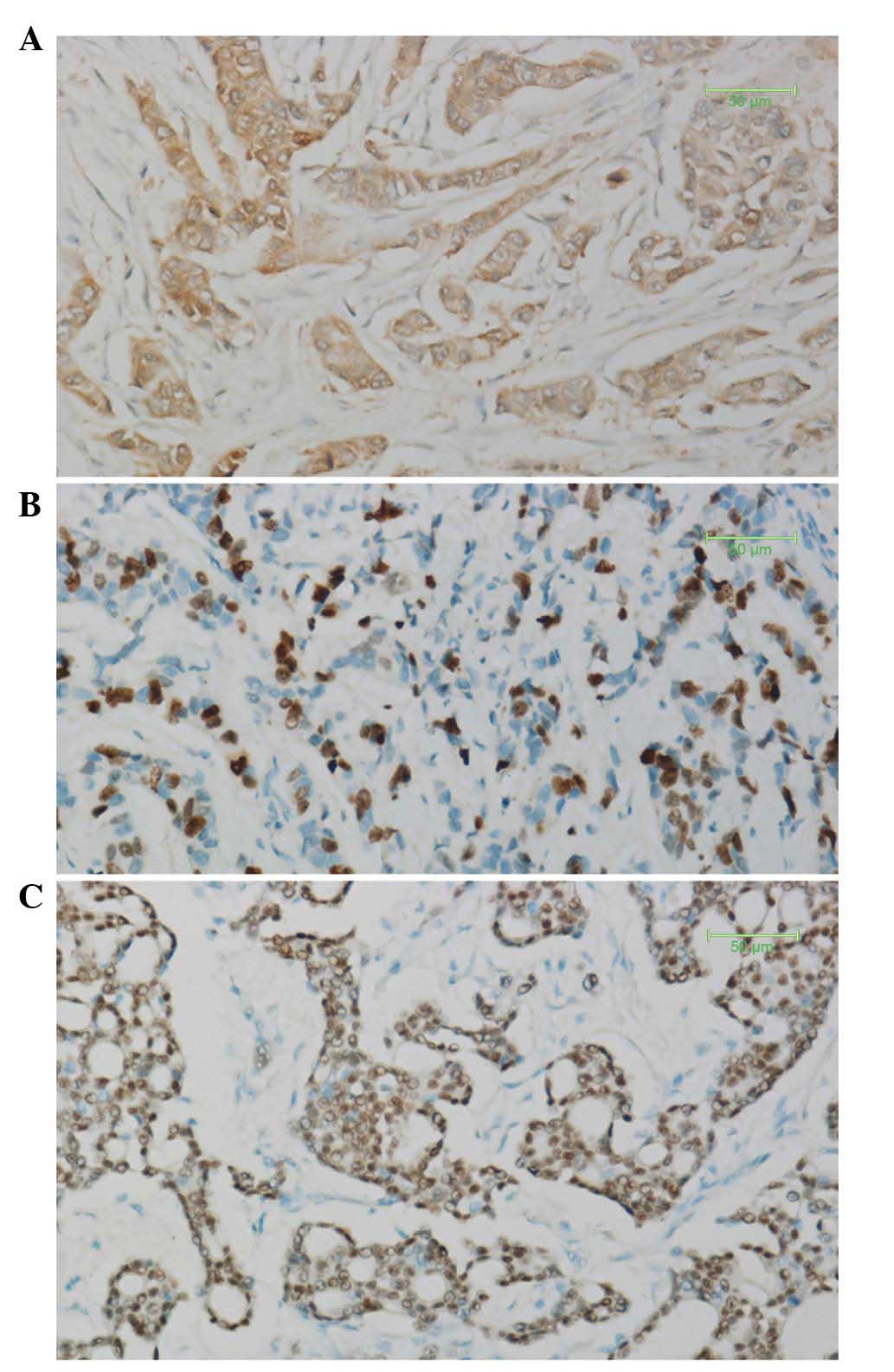
Survivin expression was semi-quantitatively
evaluated according to the percentage of cells with nuclear and/or
cytoplasmic reactions. Immunoreactivity was assessed in at least
five high-power fields at a magnification of ×200 and scores were
classified as follows: 0, <5% of tumor cells stained; 1, 5–20%
of tumor cells stained; and 2, >20% of tumor cells stained. A
score of 2 was considered as positive and scores of 0 or 1 were
considered negative (Fig. 1A)
(5). For Ki-67, nuclear staining
in >20% of the tumor cells was considered to indicate high-level
expression (Fig. 1B). Tumors were
classified as ER-positive when nuclear staining was visible in ≥10%
of the tumor cells (Fig. 1C)
(6).
Statistical analysis
The primary endpoint was to assess the predictive
value of survivin, Ki-67, ER-negative tumor status and tumor grade
for the ORR to docetaxel-based NAC in patients with LABC, to
enhance the breast-conserving surgery rate with docetaxel-based
NAC. The effects of survivin, Ki-67, ER tumor status and tumor
grade on the response to NAC and the correlations between survivin,
Ki-67 and ER tumor status were assessed with the Pearson's
Chi-square test (with a correction for continuity in comparisons
with small numbers). Possible predictive factors associated with
response probability at a significance level of ≤0.20 were
considered in a multivariable logistic regression analysis
(6). P<0.05 was determined as
the threshold for statistical significance and all P-values were
two-tailed. Data were analyzed with SPSS software for Windows
version 16.0 (SPSS Inc., Chicago, IL, USA).
Results
Tumor response
MRI revealed that 21 (31%) of the 68 patients
exhibited a clinical complete response and 37 (54%) exhibited a
partial response. Therefore, the ORR was 85%. The disease was
classified as stable in 11 (16.2%) of the 68 patients and no
patient had progressive disease. pCR was confirmed in 14 (20%) of
the 68 patients and 37 patients (54%) underwent breast-conserving
surgery.
Predictive value of survivin, Ki-67, ER
status and tumor grade
Of the 68 breast carcinomas, survivin expression was
detected in 50 (74%), with no expression observed in the adjacent
normal tissue. High-level expression of Ki-67 was detected in 52
(77%) tumors and a ER-negative status was detected in 31 (46%)
tumors. A total of 40 tumors (59%) were high-grade (grade III) and
the remaining 28 (41%) were grade I/II.
In the univariate analysis, survivin expression,
high-level Ki-67 expression and high tumor grade (grade III) were
significantly associated with ORR (P=0.007, 0.024 and 0.047,
respectively). Survivin expression and high-level Ki-67 expression
were significantly associated with pCR (P=0.029 and 0.048,
respectively) (Table I). In the
multivariate analysis, survivin expression and high tumor grade,
but not high-level Ki-67 expression, were significantly associated
with ORR (P=0.030 and 0.036, respectively) and none of the factors
was significantly associated with pCR (Table II).
| Table IIMultivariate analysis of the
association of protein expressions with ORR and pCR. |
Table II
Multivariate analysis of the
association of protein expressions with ORR and pCR.
| Predictive
markers | Odds ratio | 95% CI | P-value |
|---|
| Survivin |
| ORR | 5.879 | 1.185–29.178 | 0.030a |
| pCR | 3.652 | 0-0 | 0.998 |
| Ki-67 |
| ORR | 3.012 | 0.647–14.022 | 0.160 |
| pCR | 2.359 | 0-0 | 0.998 |
| Tumor grade |
| ORR | 5.993 | 1.124–31.967 | 0.036a |
| pCR | 0.254 | 0.537–10.474 | 0.254 |
| PgR | 0.460 | 0.091–2.328 | 0.348 |
Correlation between biomarkers
A strong correlation was observed between the
expression of survivin and the high-level expression of Ki-67
(P=0.034). It was not possible to clearly determine a correlation
between survivin expression and ER-positive tumor status (P=0.223)
or an inverse correlation between high-level Ki-67 expression and
ER-positive tumor status (P=0.059).
Discussion
Breast cancer is the most common cancer among women.
NAC may lead to tumor downstaging and increase the likelihood of
patients undergoing successful breast-conserving surgery. However,
the benefits depend on the selection of the most effective
chemotherapy regimens. Doctors commonly select regimens on the
basis of clinical and histological characteristics and treatment is
generally not individualized. Therefore, numerous patients may
receive unnecessary or ineffective NAC, which may lead to toxic
effects, increased cost, delay to curative treatment and tumor
cross-resistance (7). Thus,
methods to facilitate the selection of the most effective regimens
are urgently needed.
Anthracycline-based regimens for breast cancer
achieve high response rates. A widely used regimen for breast
cancer NAC is combined cyclophosphamide, doxorubicin and
fluorouracil; however, resistance to this regimen has emerged.
Previous trials reported good response rates with taxane-containing
regimens (8,9). Docetaxel has exhibited high activity
in combination with doxorubicin, including in patients with
anthracycline-resistant disease. Nabholtz et al(10) reported that patients with
metastatic breast cancer treated with combined docetaxel and
doxorubicin exhibited significantly improved ORRs compared to those
of patients treated with doxorubicin and cyclophosphamide. Mackey
et al(11) provided
evidence in their 10-year analysis of the randomised BCIRG 001
trial that TAC for the treatment of patients with node-positive,
early breast cancer provides long-term disease-free survival and
overall survival benefits compared to fluorouracil (5-FU),
doxorubicin and cyclophosphamide (FAC), irrespective of nodal,
hormone receptor and human epidermal growth factor receptor-2
(HER2) status.
Despite the improvements in ORR and the assessment
of several chemotherapeutic regimens, the pCR rate following NAC
for breast cancer remains low (12). Survival is significantly prolonged
in patients who achieve pCR after NAC compared to those who do not
(13,14). This finding may, therefore, be used
as a suitable surrogate endpoint for response in studies on NAC. In
our study, after 4–6 cycles of the TAC regimen, the clinical CR
rate was 31% and the pCR rate was 20%. Moreover, our primary
endpoint was breast-conserving surgery. This suggests that the TAC
regimen may be effective as NAC for patients with LABC.
The survivin gene (BIRC5) is a member of the
inhibitor of apoptosis protein family and has various functions:
regulation of cell proliferation and division, inhibition of cell
apoptosis and promotion of angiogenesis (15). Survivin expression was detected by
immunohistochemistry in 60–70% of primary breast tumors, with
little or no expression in control tissue samples. High expression
of survivin has been correlated with poor clinical outcomes in
breast, lung, prostate, pancreatic and colorectal cancers (16). Survivin may, therefore, be a
potential prognostic factor, a predictive factor for response to
treatment and a therapeutic target in breast cancer patients. In
the univariate analysis, we observed a significant correlation of
survivin expression with ORR and pCR to NAC. However, in the
multivariate analysis, a significant correlation was observed only
with ORR. Several studies reported that patients with a pCR
following NAC exhibited higher survival rates compared to those
without pCR (13,14) and a high expression of survivin has
been correlated with poor clinical outcomes (15,16).
Therefore, the results of a previous study by Petrarca et
al(18), indicating that
survivin may be a predictive biomarker of pCR to NAC in patients
with stage II and III breast cancer, were not in accordance with
our results and require further investigation. Another study
reported that failure of the downregulation of survivin following
neoadjuvant radiochemotherapy in rectal cancer was associated with
distant metastases and shortened survival (17), although there was no report of the
association with breast cancer.
Gerdes et al(19) previously used a mouse monoclonal
antibody against a nuclear antigen from a Hodgkin's lymphoma cell
line and identified Ki-67 as a marker of cell proliferation. Ki-67
was universally expressed among proliferating cells and absent in
quiescent cells. Several studies have since investigated the
possible prognostic role for Ki-67 in breast cancer, with varying
results. Urruticoechea et al(20) conducted a review of 40 studies
involving >11,000 patients and reported that Ki-67 expression
alone is able to predict positive or negative outcomes in patients
with node-negative breast cancer, although the predictive value was
not maintained in multivariate analyses. de Azambuja et
al(21) demonstrated that
Ki-67 expression in node-negative and node-positive breast cancer
was associated with poor overall and disease-free survival. The
findings of Stuart-Harris et al(22) did not support Ki-67 as a prognostic
marker for use in routine practice. Sánchez-Muñoz et
al(13) identified the Ki-67
index as an independent prognostic factor for disease-free and
overall survival in breast cancer patients treated with NAC. A high
Ki-67 expression and hormone receptor-negative status were shown to
be predictors of pCR. In the univariate, but not the multivariate,
analysis we observed that a high-level expression of Ki-67 was
significantly associated with good ORR and pCR to NAC, which may be
attributed to our small study sample. Although it is disputable
whether Ki-67 is an independent predictor or prognostic marker, a
high expression of Ki-67 indicating good response to
docetaxel-based NAC suggests that breast-conserving surgery may be
performed in the high-expression patients.
ER and progesterone receptor (PgR) status provides
the index for sensitivity to endocrine treatment; therefore, it is
the most important biomarker in breast cancer. Numerous studies
identified ER and PgR as independent variables, significantly
associated with the likelihood of achieving pCR (23,24).
However, the findings of our study, taken together with those of
Wang et al(25), do not
support this result. This discordance may be explained by the
heterogeneity of the investigation methods, particularly the
cut-offs used by various studies. In our study, the sample size was
small and the detection of PgR expression was performed after the
NAC, which may change the status and affect the result. We observed
that high histological grade was a significant independent
predictor of pCR in multivariate models with low-grade tumors,
which is consistent with the findings of previous studies in
multivariate models (6).
A good correlation was observed between survivin
expression and high-level Ki-67 expression, similar to the findings
of Xu et al(26). A
previous study by Lee et al(27) reported an inverse correlation
between high-level Ki-67 expression and ER-positive tumor status.
However, our study did not support that result and whether survivin
expression correlates with ER-positive tumor status could not be
determined. This was not in accordance with the findings of Ryan
et al(28), possibly due to
their detection methods for protein quantification being more
accurate.
In conclusion, a regimen of 75 mg/m2
docetaxel, 60 mg/m2 pirarubicin and 500 mg/m2
cyclophosphamide once every 3 weeks may be effective as NAC in LABC
and more patients may benefit from undergoing breast
conserving-surgery after the treatment. Survivin expression and
high tumor grade were identified as independent predictors of
response.
Acknowledgements
This study was supported by a grant from the
Lianyungang Municipal Health Bureau (no. 09009). The authors would
like to thank all the patients and their family members for their
consent and cooperation, without them this study would not have
been possible.
References
|
1
|
Ayers M, Symmans WF, Stec J, Damokosh AI,
Clark E, Hess K, Lecocke M, Metivier J, Booser D, Ibrahim N, Valero
V, Royce M, Arun B, Whitman G, Ross J, Sneige N, Hortobagyi GN and
Pusztai L: Gene expression profiles predict complete pathologic
response to neoadjuvant paclitaxel and fluorouracil, doxorubicin,
and cyclophosphamide chemotherapy in breast cancer. J Clin Oncol.
22:2284–2293. 2004. View Article : Google Scholar
|
|
2
|
van't Veer LJ, Dai H, van de Vijver MJ, He
YD, Hart AA, Mao M, Peterse HL, van der Kooy K, Marton MJ,
Witteveen AT, Schreiber GJ, Kerkhoven RM, Roberts C, Linsley PS,
Bernards R and Friend SH: Gene expression profiling predicts
clinical outcome of breast cancer. Nature. 415:530–536.
2002.PubMed/NCBI
|
|
3
|
Therasse P, Arbuck SG, Eisenhauer EA,
Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van
Oosterom AT, Christian MC and Gwyther SG: New guidelines to
evaluate the response to treatment in solid tumors. European
Organization for Research and Treatment of Cancer, National Cancer
Institute of the United States, National Cancer Institute of
Canada. J Natl Cancer Inst. 92:205–216. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Elston CW and Ellis IO: Pathological
prognostic factors in breast cancer. I. The value of histological
grade in breast cancer: experience from a large study with
long-term follow-up. Histopathology. 19:403–410. 1991. View Article : Google Scholar
|
|
5
|
Asanuma H, Torigoe T, Kamiguchi K,
Hirohashi Y, Ohmura T, Hirata K, Sato M and Sato N: Survivin
expression is regulated by coexpression of human epidermal growth
factor receptor 2 and epidermal growth factor receptor via
phosphatidylinositol 3-kinase/AKT signaling pathway in breast
cancer cells. Cancer Res. 65:11018–11025. 2005. View Article : Google Scholar
|
|
6
|
Petit T, Wilt M, Velten M, Millon R,
Rodier JF, Borel C, Mors R, Haegelé P, Eber M and Ghnassia JP:
Comparative value of tumor grade, hormonal receptors, Ki-67, HER-2
and topoisomerase II alpha status as predictive markers in breast
cancer patients treated with neoadjuvant anthracycline-based
chemotherapy. Eur J Cancer. 40:205–211. 2004. View Article : Google Scholar
|
|
7
|
Fuksa L, Micuda S, Grim J, Ryska A and
Hornychova H: Predictive biomarkers in breast cancer: their value
in neoadjuvant chemotherapy. Cancer Invest. 30:663–678. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cortes J and Roché H: Docetaxel combined
with targeted therapies in metastatic breast cancer. Cancer Treat
Rev. 38:387–396. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Belfiglio M, Fanizza C, Tinari N,
Ficorella C, Iacobelli S and Natoli C: Meta-analysis of phase III
trials of docetaxel alone or in combination with chemotherapy in
metastatic breast cancer. J Cancer Res Clin Oncol. 138:221–229.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nabholtz JM, Falkson C, Campos D, Szanto
J, Martin M, Chan S, Pienkowski T, Zaluski J, Pinter T, Krzakowski
M, Vorobiof D, Leonard R, Kennedy I, Azli N, Murawsky M, Riva A and
Pouillart P: Docetaxel and doxorubicin compared with doxorubicin
and cyclophosphamide as first-line chemotherapy for metastatic
breast cancer: results of a randomized, multicenter, phase III
trial. J Clin Oncol. 21:968–975. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mackey JR, Martin M, Pienkowski T, Rolski
J, Guastalla JP, Sami A, Glaspy J, Juhos E, Wardley A, Fornander T,
Hainsworth J, Coleman R, Modiano MR, Vinholes J, Pinter T,
Rodríguez-Lescure A, Colwell B, Whitlock P, Provencher L, Laing K,
Walde D, Price C, Hugh JC, Childs BH, Bassi K, Lindsay MA, Wilson
V, Rupin M, Houé V and Vogel C: Adjuvant docetaxel, doxorubicin,
and cyclophosphamide in node-positive breast cancer: 10-year
follow-up of the phase 3 randomised BCIRG 001 trial. Lancet Oncol.
14:72–80. 2013.PubMed/NCBI
|
|
12
|
Sachelarie I, Grossbard ML, Chadha M,
Feldman S, Ghesani M and Blum RH: Primary systemic therapy of
breast cancer. Oncologist. 11:574–589. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sánchez-Muñoz A, Plata-Fernández YM,
Fernández M, Jaén-Morago A, Fernández-Navarro M, de la
Torre-Cabrera C, Ramirez-Tortosa C, Lomas-Garrido M, Llácer C,
Navarro-Perez V, Alba-Conejo E and Sánchez-Rovira P: The role of
immunohistochemistry in breast cancer patients treated with
neoadjuvant chemotherapy: an old tool with an enduring prognostic
value. Clin Breast Cancer. 13:146–152. 2013.PubMed/NCBI
|
|
14
|
Untch M, Fasching PA, Konecny GE,
Hasmüller S, Lebeau A, Kreienberg R, Camara O, Müller V, du Bois A,
Kühn T, Stickeler E, Harbeck N, Höss C, Kahlert S, Beck T, Fett W,
Mehta KM, von Minckwitz G and Loibl S: Pathologic complete response
after neoadjuvant chemotherapy plus trastuzumab predicts favorable
survival in human epidermal growth factor receptor 2-overexpressing
breast cancer: results from the TECHNO trial of the AGO and GBG
study groups. J Clin Oncol. 29:3351–3357. 2011. View Article : Google Scholar
|
|
15
|
Church DN and Talbot DC: Survivin in solid
tumors: rationale for development of inhibitors. Curr Oncol Rep.
14:120–128. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Altieri DC: Survivin, cancer networks and
pathway-directed drug discovery. Nat Rev Cancer. 8:61–70. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sprenger T, Rodel F, Beissbarth T, Conradi
LC, Rothe H, Homayounfar K, Wolff HA, Ghadimi BM, Yildirim M,
Becker H, Rödel C and Liersch T: Failure of downregulation of
survivin following neoadjuvant radiochemotherapy in rectal cancer
is associated with distant metastases and shortened survival. Clin
Cancer Res. 17:1623–1631. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Petrarca CR, Brunetto AT, Duval V,
Brondani A, Carvalho GP and Garicochea B: Survivin as a predictive
biomarker of complete pathologic response to neoadjuvant
chemotherapy in patients with stage II and stage III breast cancer.
Clin Breast Cancer. 11:129–134. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gerdes J, Schwab U, Lemke H and Stein H:
Production of a mouse monoclonal antibody reactive with a human
nuclear antigen associated with cell proliferation. Int J Cancer.
3:13–20. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Urruticoechea A, Smith IE and Dowsett M:
Proliferation marker Ki-67 in early breast cancer. J Clin Oncol.
23:7212–7220. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
de Azambuja E, Cardoso F, de Castro G Jr,
Colozza M, Mano MS, Durbecq V, Sotiriou C, Larsimont D,
Piccart-Gebhart MJ and Paesmans M: Ki-67 as prognostic marker in
early breast cancer: a meta-analysis of published studies involving
12,155 patients. Br J Cancer. 96:1504–1513. 2007.PubMed/NCBI
|
|
22
|
Stuart-Harris R, Caldas C, Pinder SE and
Pharaoh P: Proliferation markers and survival in early breast
cancer: a systematic review and meta-analysis of 85 studies in
32,825 patients. Breast. 17:323–334. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Colleoni M, Viale G, Zahrieh D,
Bottiglieri L, Gelber RD, Veronesi P, Balduzzi A, Torrisi R, Luini
A, Intra M, Dellapasqua S, Cardillo A, Ghisini R, Peruzzotti G and
Goldhirsch A: Expression of ER, PgR, HER1, HER2, and response: a
study of preoperative chemotherapy. Ann Oncol. 19:465–472. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Colleoni M, Viale G, Zahrieh D, Pruneri G,
Gentilini O, Veronesi P, Gelber RD, Curigliano G, Torrisi R, Luini
A, Intra M, Galimberti V, Renne G, Nolè F, Peruzzotti G and
Goldhirsch A: Chemotherapy is more effective in patients with
breast cancer not expressing steroid hormone receptors: a study of
preoperative treatment. Clin Cancer Res. 10:6622–6628. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wang L, Jiang Z, Sui M, Shen J, Xu C and
Fan W: The potential biomarkers in predicting pathologic response
of breast cancer to three different chemotherapy regimens: a case
control study. BMC Cancer. 9:2262009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Xu C, Yamamoto-Ibusuki M, Yamamoto Y,
Yamamoto S, Fujiwara S, Murakami K, Okumura Y, Yamaguchi L, Fujiki
Y and Iwase H: High survivin mRNA expression is a predictor of poor
prognosis in breast cancer: a comparative study at the mRNA and
protein level. Breast Cancer. Sep 12–2012.(Epub ahead of
print).
|
|
27
|
Lee J, Im YH, Lee SH, Cho EY, Choi YL, Ko
YH, Kim JH, Nam SJ, Kim HJ, Ahn JS, Park YS, Lim HY, Han BK and
Yang JH: Evaluation of ER and Ki-67 proliferation index as
prognostic factors for survival following neoadjuvant chemotherapy
with doxorubicin/docetaxel for locally advanced breast cancer.
Cancer Chemother Pharmacol. 61:569–577. 2008. View Article : Google Scholar
|
|
28
|
Ryan BM, Konecny GE, Kahlert S, Wang HJ,
Untch M, Meng G, Pegram MD, Podratz KC, Crown J, Slamon DJ and
Duffy MJ: Survivin expression in breast cancer predicts clinical
outcome and is associated with HER2, VEGF, urokinase plasminogen
activator and PAI-1. Ann Oncol. 17:597–604. 2006. View Article : Google Scholar : PubMed/NCBI
|