Introduction
Colorectal cancer is a major cause of cancer-related
mortality worldwide, causing ∼500,000 deaths annually (1). Following curative resection, there is
a considerable risk of recurrence in patients with stage II and III
disease. Recurrence occurs in ∼20% of stage II patients and ∼50% of
the stage III patients may be cured with surgery alone (2–5).
Therefore, it is critical to identify patients with a high risk of
recurrence.
Aquaporins (AQPs) are a family of small membrane
transport proteins that assemble in cell membranes as tetramers and
primarily act as water-selective pores that facilitate the
osmotically-driven transport of water across plasma membranes
(6,7).
AQP1 is expressed in vascular endothelial cells
throughout the body is not expressed in the central nervous,
genital, lymphoid and gastrointestinal systems, including the
colonic mucosa (8,9). It was reported that several types of
cancer express AQP1 and it may be involved in carcinogenesis
(10,11). An in vitro study
demonstrated that AQP1-mediated plasma membrane water permeability
is crucial for colon cancer cell migration and may be associated
with tumor invasion and metastasis (12). However, available data on the
clinical significance of AQP1 in colon cancer are limited. In the
present study, the association of AQP1 expression in colon cancer
with clinicopathological findings was evaluated using tissue
micro-array (TMA) analysis and it was demonstrated that AQP1 is a
prognostic factor for advanced colon cancer.
Materials and methods
Patients
A total of 168 consecutive stage II and III colon
cancer patients who underwent curative resection between January,
1997 and August, 2008 were investigated. The final stage was
pathologically confirmed according to the International Union
Against Cancer (UICC) classification system, 7th edition. The
degree of lymphovascular and vascular invasion was classified as
negative, mild or severe by the pathologists of our hospital.
Patients with rectosigmoid cancer were included in this study.
Tissue microarrays were prepared from each tumor and a
representative area was carefully selected from a hematoxylin and
eosin (H&E)-stained section. A total of 120 patients (51 cases
with stage II and 69 cases with stage III disease) with no other
causes of death were subjected to statistical analysis.
Tissue microarray
A TMA is composed of small 1.0-mm cores of tissue
obtained from paraffin blocks. For tissue stamping, the tumor areas
were marked on H&E-stained sections and then marked directly on
the corresponding formalin-fixed, paraffin-embedded tissue blocks.
Paraffin-embedded tumor material was cut into 4-μm sections
and placed onto glass slides, followed by staining with H&E and
anti-AQP1 antibody (H-55; Santa Cruz Biotechnology, Inc., Santa
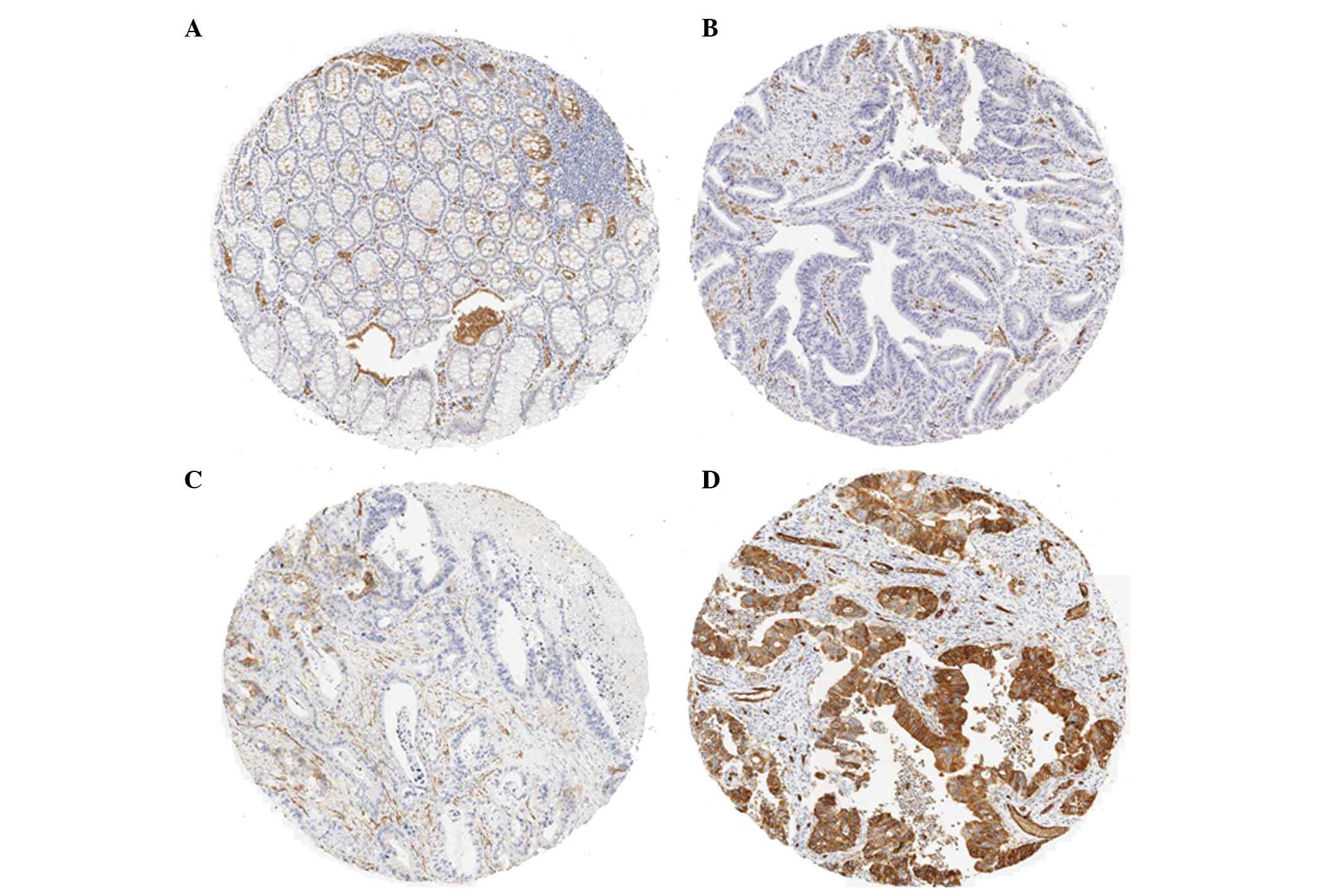
Cruz, CA, USA) at a 1:100 dilution. Immunostaining of the TMAs was
graded semi-quantitatively by considering the staining intensity
and the percentage of positive tumor cells by two pathologists who
were blinded to the clinicopathological variables. The staining
intensity was scored using three grades as follows: 0, no staining
of cancer cells; 1, weak staining; and 2, strong staining. The
percentage of stained tumor cells was classified on a scale of 3
grades: 0, no positive cells; 1, <50% positive cancer cells; and
2, >50% positive cancer cells (Fig.
1). The AQP1 expression by the tumor was defined as positive
when the sum of the intensity and the extent scores was ≥3 and as
negative when the score was <3.
Statistical analysis
The JMP-9 software package was used for statistical
analysis. AQP1 expression was analyzed as nominal data. The
association between AQP1 expression and clinicopathological
characteristics was analyzed using the χ2 test or the
two-sided Student’s t-test, as appropriate. Survival was assessed
by the Kaplan-Meier method and compared by the log-rank test. The
multivariate analysis was performed using Cox’s proportional
hazards model to evaluate risk factors for cancer-related
mortality. P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics
The clinical characteristics of the 120 colon cancer
patients are summarized in Table
I. Ninety-two percent of the patients had tumor invasion deeper
than pT3 and 8 cases had pT4b. Lymph node metastasis was identified
in 57.5% of the patients. Lymphovascular and vascular invasion were
positive in 68.4 and 60.0% of the patients, respectively.
Postoperative chemotherapy was administered to 57.5% of the
patients and the regimens were as follows: UFT in 43 patients,
LV/UFT in 9, CDDP/5FU in 3, FOLFOX in 3 and FOLFIRI in 9 patients.
The recurrence rate of this series was 25.8%.
 | Table I.Patient clinicopathological
characterisitics. |
Table I.
Patient clinicopathological
characterisitics.
| Characteristics | No. | % |
|---|
| Age (years) | | |
| <75 | 92 | 76.7 |
| ≥75 | 28 | 23.3 |
| Gender | | |
| Male | 65 | 54.2 |
| Female | 55 | 45.8 |
| Tumor location | | |
| Right | 57 | 47.5 |
| Left | 63 | 52.5 |
| Depth of
invasiona | | |
| pT1 | 1 | 0.8 |
| pT2 | 8 | 6.7 |
| pT3 | 81 | 67.5 |
| pT4a | 22 | 18.3 |
| pT4b | 8 | 6.7 |
| Bowel
obstruction | | |
| Yes | 14 | 11.7 |
| No | 106 | 88.3 |
| Lymph node
involvementa | | |
| pN0 | 51 | 42.5 |
| pN1 | 51 | 42.5 |
| pN2 | 18 | 15.0 |
| Differentiation | | |
| High | 58 | 48.3 |
| Moderate | 52 | 43.3 |
| Poor/Muc/Sig | 10 | 8.3 |
| Lymphovascular
invasion | | |
| Negative | 38 | 31.7 |
| Mild | 53 | 44.2 |
| Severe | 29 | 24.2 |
| Vascular
invasion | | |
| Negative | 48 | 40.0 |
| Mild | 35 | 29.2 |
| Severe | 37 | 30.8 |
| CEA | | |
| <3.5 | 69 | 57.5 |
| ≥3.5 | 46 | 38.3 |
| CA19-9 | | |
| <37 | 88 | 73.3 |
| ≥37 | 22 | 18.3 |
| Postoperative
chemotherapy | | |
| Yes | 69 | 57.5 |
| No | 51 | 42.5 |
| Recurrence | | |
| Yes | 31 | 25.8 |
| No | 89 | 74.2 |
| AQP1 scoreb | | |
| 0 | 64 | 53.3 |
| 2 | 13 | 10.8 |
| 3 | 17 | 14.2 |
| 4 | 26 | 21.7 |
Immunohistochemical staining for
AQP1
To evaluate the expression of AQP1 in colon cancer,
immunostaining of 120 paraffin-embedded primary colon cancer
specimens was performed. The normal epithelium exhibited no AQP1
staining (Fig. 1A). The AQP1 score
was 0 in 64 (53.3%), 2 in 13 (10.8%), 3 in 17 (14.2%) and 4 in 26
patients (21.7%). The incidence of AQP1-positive expression in
colon cancer (score ≥3) was 35.9% (43/120) (Table I).
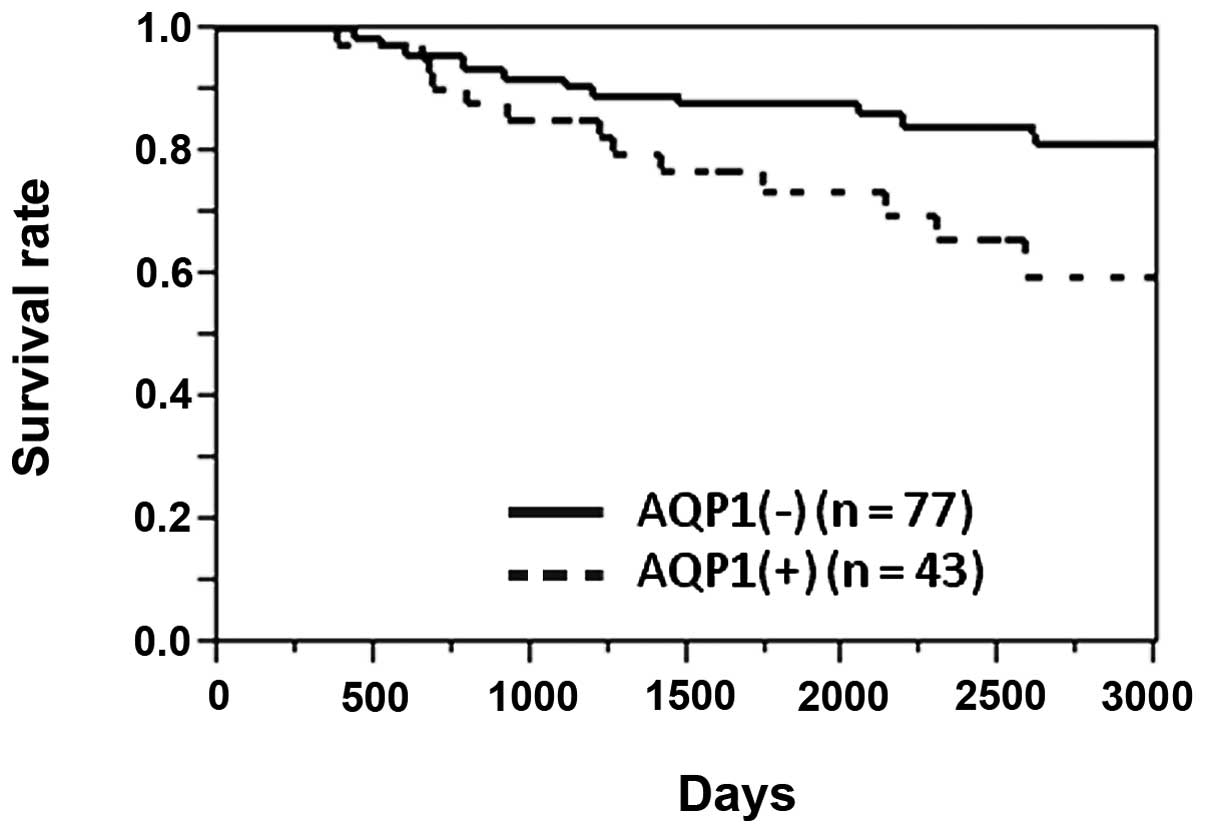
Survival
The 5-year survival rate of the 120 patients was
83.1%. The 5-year survival rates of AQP1-positive and -negative
patients were 73.5 and 87.9%, respectively. The survival rate of
AQP1-positive patients was significantly lower compared to that of
AQP1-negative patients (P=0.030, log-rank test) (Fig. 2).
Correlation of AQP1 expression with
clinicopathological factors
The association of AQP1 expression with
clinicopathological factors is shown in Table II. The AQP1 expression exhibited a
significant correlation with lymph node metastasis (P=0.042),
severe lymphovascular invasion (P=0.012) and vascular invasion
(P=0.017). AQP1 expression was also higher in left-sided compared
to that in right-sided colon cancer (P=0.038). Only one of the 10
poorly differentiated adenocarcinomas expressed AQP1, although the
difference was not statistically significant.
| Table II.Association between patient
characteristics and AQP1 expression in colon cancer. |
Table II.
Association between patient
characteristics and AQP1 expression in colon cancer.
| Characteristics | AQPa overexpression
| P-value |
|---|
| (−) | (+) |
|---|
| Age (years) | | | |
| <75 | 60 | 32 | 0.663 |
| ≥75 | 17 | 11 | |
| Gender | | | |
| Male | 40 | 25 | 0.513 |
| Female | 37 | 18 | |
| Tumor location | | | |
| Right | 42 | 15 | 0.038 |
| Left | 35 | 28 | |
| Depth of
invasion | | | |
| pT1 | 1 | 0 | 0.779 |
| pT2 | 5 | 3 | |
| pT3 | 54 | 27 | |
| pT4a | 11 | 11 | |
| pT4b | 6 | 2 | |
| Bowel
obstruction | | | |
| Yes | 8 | 6 | 0.774 |
| No | 69 | 37 | |
| Lymph node
involvement | | | |
| pN0 | 38 | 13 | 0.042 |
| pN1, N2 | 39 | 30 | |
|
Differentiation | | | |
| High,
moderate | 68 | 42 | 0.151 |
| Poor/Muc/Sig | 9 | 1 | |
| Lymphovascular
invasion | | | |
|
Negative-mild | 64 | 27 | 0.012 |
| Severe | 13 | 16 | |
| Vascular
invasion | | | |
|
Negative-mild | 59 | 24 | 0.017 |
| Severe | 18 | 19 | |
| CEA | | | |
| <3.5 | 42 | 27 | 0.476 |
| ≥3.5 | 31 | 15 | |
| CA19-9 | | | |
| <37 | 55 | 33 | 0.517 |
| ≥37 | 16 | 6 | |
| Postoperative
chemotherapy | | | |
| Yes | 39 | 30 | 0.057 |
| No | 38 | 13 | |
| Recurrence | | | |
| Yes | 16 | 15 | 0.090 |
| No | 61 | 28 | |
Prognostic impact of AQP1 expression
The association of various clinical factors to the
prognosis is shown in Table III.
The factors associated with poor prognosis were age ≥75 years
(P=0.0001), right colon cancer (P=0.019), pT4b (P=0.0004), lymph
node metastasis (P=0.049), bowel obstruction by the tumor
(P=0.029), CEA ≥3.5 (P=0.004) and AQP1 positivity (P=0.030).
Furthermore, the Cox’s proportional hazard analysis using these
factors revealed that age ≥75 years [risk ratio (RR)=3.209;
P=0.020], pT4b (RR=7.968; P=0.004), a high CEA level (RR=3.254;
P=0.021) and AQP1 positivity (RR=2.593; P=0.038) were independent
poor prognostic factors (Table
IV).
| Table III.Kaplan-Meier analysis of factors
related to overall survival. |
Table III.
Kaplan-Meier analysis of factors
related to overall survival.
| Factors | No. | 5y-OS | P-value |
|---|
| Age (years) | | | |
| <75 | 92 | 87.4 | 0.0001a |
| ≥75 | 28 | 69.7 | |
| Gender | | | |
| Male | 65 | 87.9 | 0.061 |
| Female | 55 | 77.5 | |
| Tumor location | | | |
| Right | 55 | 75.7 | 0.019a |
| Left | 63 | 89.8 | |
| Depth of
invasion | | | |
| pT1, 2, 3,
4a | 112 | 84.7 | 0.0004a |
| pT4b | 8 | 62.5 | |
| Bowel
obstruction | | | |
| Yes | 14 | 64.2 | 0.029a |
| No | 106 | 86.0 | |
|
Differentiation | | | |
| High | 58 | 78.8 | 0.167 |
| Other | 62 | 87.6 | |
| Lymphovascular
invasion | | | |
|
Negative-mild | 92 | 86.2 | 0.245 |
| Severe | 28 | 73.1 | |
| Vascular
invasion | | | |
|
Negative-mild | 79 | 82.9 | 0.626 |
| Severe | 41 | 83.4 | |
| Lymph node
involvement | | | |
| Negative | 51 | 92.0 | 0.049a |
| Positive | 69 | 76.1 | |
| CEA | | | |
| <3.5 | 69 | 93.8 | 0.004a |
| ≥3.5 | 46 | 72.3 | |
| CA19-9 | | | |
| <37 | 89 | 91.4 | 0.086 |
| ≥37 | 22 | 68.1 | |
| Postoperative
chemotherapy | | | |
| Yes | 69 | 85.9 | 0.085 |
| No | 51 | 79.4 | |
| AQP1 | | | |
| Negative | 77 | 87.9 | 0.030a |
| Positive | 43 | 73.7 | |
| Table IV.Multivariate analysis of factors
associated with overall survival. |
Table IV.
Multivariate analysis of factors
associated with overall survival.
| Factors | Risk ratio | 95% CI
| P-value |
|---|
| Lower | Upper |
|---|
| Age ≥75 years | 3.209 | 1.202 | 8.789 | 0.020a |
| Right colon
cancer | 1.642 | 0.606 | 4.821 | 0.334 |
| Bowel
obstruction | 1.130 | 0.328 | 3.361 | 0.829 |
| pT4b | 7.968 | 2.098 | 24.995 | 0.004a |
| Lymph node
involvement | 2.299 | 0.840 | 7.102 | 0.107 |
| CEA ≥3.5 | 3.254 | 1.193 | 9.754 | 0.021a |
| AQP1+ | 2.593 | 1.057 | 6.439 | 0.038a |
Discussion
The AQPs are a family of small (∼30-kDa monomers)
membrane transport proteins that assemble in cell membranes as
tetramers and primarily act as water-selective pores, facilitating
the osmotically-driven transport of water across plasma membranes
(6,7). Recently, various studies have focused
on the association of AQPs and cancer (10–17).
AQP1 is expressed in vascular endothelial cells
throughout the body, except in the normal central nervous, genital
and lymphoid systems. This molecule is also not expressed by normal
colonic epithelial glands (6–9). It
was reported that several types of cancer express AQP1 and it may
be involved in tumor invasion and metastasis. Hu et al
(13) demonstrated that AQP1
expression by tumor cells may increase local invasiveness and the
ability to metastasize by comparing B16F10 melanoma and 4T1 breast
tumor mouse cell lines with or without AQP1 expression. The results
of that study demonstrated that AQP1 expression increased the water
permeability of the plasma membrane and the migration of cancer
cells in vitro.
In addition, Moon et al (10) reported that AQP1 was associated
with colorectal carcinogenesis and Yiang (12) reported that the AQP1 activity in
plasma membranes affected HT20 colon cancer cell migration in
vitro. Those findings revealed that the expression of AQP1 is
associated with tumor progression in colon cancer. Our findings
also suggested that AQP1 is associated with cancer progression.
Furthermore, our study demonstrated that AQP1
expression is a predictor of advanced colon cancer. The
overexpression of AQP1 has already been demonstrated to be a
prognostic indicator in basal cell carcinoma of the breast
(14), clear cell renal cell
carcinoma (15) and lung carcinoma
(16). However, there have been no
previous studies on the association of AQP1 with the prognosis of
colon cancer. To the best of our knowledge, this was the first
study to demonstrate that AQP1 is a prognostic biomarker for colon
cancer.
Of note, although AQP1 overexpression is a poor
prognostic factor for breast, lung and colon cancer, it is a good
prognostic factor for renal carcinoma. The reason for this
difference has not been elucidated thus far. Furthermore, our
study, we observed that the AQP1 expression in poorly
differentiated adenocarcinoma was low, although low differentiation
is considered to be included among the poor prognostic factors and
AQP1 expression was predicted to be high in this histological type.
However, only two of the 10 cases of poorly differentiated
carcinoma exhibited recurrence in our series. More cases of poorly
differentiated adenocarcinoma should be investigated to elucidate
these inconsistencies.
Although postoperative chemotherapy was shown to
affect treatment outcomes, the effect was not statistically
significant, which may be attributed to the use of ineffective
regimens. The effects of postoperative chemotherapy were assessed
according to AQP1 expression and there was no observed difference
(data not shown). This result may not immediately prove the
validity of postoperative chemotherapy. Recently designed standard
regimens, such as FOLFOX, may improve the prognosis of high-risk
colon cancer patients.
The possibility of targeting AQP1 for the treatment
of colon cancer was recently suggested. Bin et al (17) reported that acetazolamide, a
carbonic anhydrase inhibitor (Diamox®) that is used to
treat glaucoma and epilepsy, inhibited AQP1 expression and colon
cancer xenograft tumor growth. Therefore, AQP1 may be a prognostic
factor as well as a treatment target in colon cancer.
In conclusion, the expression of AQP1 is associated
with characteristics of progression of colon cancer, such as lymph
node metastasis and lymphovascular invasion and is a poor
prognostic factor for advanced colon cancer. These clinical results
are consistent with previous experimental findings that support the
association of AQP1 with factors such as tumor growth, invasiveness
and metastasis. Therefore, AQP1 is a molecule that requires further
investigation regarding the prognostic evaluation and treatment of
colon cancer.
Acknowledgements
This study was supported by grants
from the Ministry of Education, Culture, Sports, Science and
Technology of Japan.
References
|
1.
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar
|
|
2.
|
Gill S, Loprinzi CL, Sargent DJ, Thomé SD,
Alberts SR, Haller DG, Benedetti J, Francini G, Shepherd LE,
Francois Seitz J, Labianca R, Chen W, Cha SS, Heldebrant MP and
Goldberg RM: Pooled analysis of fluorouracil-based adjuvant therapy
for stage II and III colon cancer: who benefits and by how much? J
Clin Oncol. 22:1797–1806. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
André T, Quinaux E, Louvet C, Colin P,
Gamelin E, Bouche O, Achille E, Piedbois P, Tubiana-Mathieu N,
Boutan-Laroze A, Flesch M, Lledo G, Raoul Y, Debrix I, Buyse M and
de Gramont A: Phase III study comparing a semimonthly with a
monthly regimen of fluorouracil and leucovorin as adjuvant
treatment for stage II and III colon cancer patients: final results
of GERCOR C96.1. J Clin Oncol. 25:3732–3738. 2007.PubMed/NCBI
|
|
4.
|
Mamounas E, Wieand S, Wolmark N, Wolmark
N, Bear HD, Atkins JN, Song K, Jones J and Rockette H: Comparative
efficacy of adjuvant chemotherapy in patients with Dukes’ B versus
Dukes’ C colon cancer: results from four National Surgical Adjuvant
Breast and Bowel Project adjuvant studies (C-01, C-02, C-03, and
C-04). J Clin Oncol. 17:1349–1355. 1999.
|
|
5.
|
Le Voyer TE, Sigurdson ER, Hanlon AL,
Hanlon AL, Mayer RJ, Macdonald JS, Catalano PJ and Haller DG: Colon
cancer survival is associated with increasing number of lymph nodes
analyzed: a secondary survey of intergroup trial INT-0089. J Clin
Oncol. 21:2912–2919. 2003.PubMed/NCBI
|
|
6.
|
Agre P, King LS, Yasui M, Guggino WB,
Ottersen OP, Fujiyoshi Y, Engel A and Nielsen S: Aquaporin water
channels - from atomic structure to clinical medicine. J Physiol.
542:3–16. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Verkman AS and Mitra AK: Structure and
function of aquaporin water channels. Am J Physiol Renal Physiol.
278:F13–F28. 2000.PubMed/NCBI
|
|
8.
|
Mobasheri A and Marples D: Expression of
the AQP-1 water channel in normal human tissues: a semiquantitative
study using tissue microarray technology. Am J Physiol Cell
Physiol. 286:C529–C537. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Bondy C, Chin E, Smith BL, Preston GM and
Agre P: Developmental gene expression and tissue distribution of
the CHIP28 water-channel protein. Proc Natl Acad Sci USA.
90:4500–4504. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Moon C, Soria JC, Jang SJ, Lee J, Obaidul
Hoque M, Sibony M, Trink B, Chang YS, Sidransky D and Mao L:
Involvement of aquaporins in colorectal carcinogenesis. Oncogene.
22:6699–6703. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Yang JH, Shi YF, Chen XD and Qi WJ: The
influence of aquaporin-1 and microvessel density on ovarian
carcinogenesis and ascites formation. Int J Gynecol Cancer.
16:400–405. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Yiang J: Aquaporin-1 activity of plasma
membrane affects HT20 colon cancer cell migration. IUBMB Life.
61:1001–1009. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Hu J and Verkman AS: Increased migration
and metastatic potential of tumor cells expressing aquaporin water
channels. FASEB J. 20:1892–1894. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Otterbach F, Callies R, Adamzik M, Kimmig
R, Siffert W, Schmid KW and Bankfalvi A: Aquaporin (AQP1)
expression is a novel characteristic feature of a particularly
aggresive subgroup of basal-like breast carcinomas. Breast Cancer
Res Treat. 120:67–76. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Huang Y, Murakami T, Sano F, Kondo K,
Nakaigawa N, Kishida T, Kubota Y, Nagashima Y and Yao M: Expression
of aquaporin 1 in primary renal tumors: a prognostic indicator for
clear-cell renal cell carcinoma. Eur Urol. 56:690–698. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Machida Y, Ueda Y, Shimasaki M, Sato K,
Sagawa M, Katsuda S and Sakuma T: Relationship of aquaporin 1, 3,
and 5 expression in lung cancer cells to cellular differentiation,
invasive growth, and metastasis potential. Hum Pathol. 42:669–678.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Bin K and Shi-Peng Z: Acetazolamide
inhibits aquaporin-1 expression and colon cancer xenograft tumor
growth. Hepatogastroenterology. 58:110–111. 2011.PubMed/NCBI
|