Introduction
Subepithelial tumors (SETs) of the gastrointestinal
tract, which may be an occasional finding on routine upper
gastrointestinal (GI) endoscopy, represent a diagnostic and
therapeutic challenge. SETs include malignant tumors, such as GI
stromal tumors, malignant lymphomas, carcinoid tumors and gastric
cancers resembling SETs, as well as benign tumors, such as
leiomyomas, aberrant pancreas and lipomas. The most common type of
tumor is gastrointestinal stromal tumor (GIST), first described by
Mazur and Clark (1). GISTs
originate from the submucosa (SM) and muscularis propria (MP) of
the GI tract. En-bloc resection is widely performed for the
treatment of definite GISTs. Currently, minimally invasive local
resection techniques, such as hybrid natural orifice transluminal
endoscopic surgery (NOTES), which consists of endoscopic
full-thickness resection (EFTR), have been developed for the
treatment of endoluminal GISTs (2,3).
Furthermore, endoscopic diagnostic methods for SETs have been
proposed (4,5), including our safe and reliable method
of bloc biopsy performed under a direct endoscopic view by using
submucosal endoscopy with a mucosal flap method (SEMF) (4). Although considered by some as a novel
optimal endoscopic mini-invasive technique for the management of
SETs, there are currently no established guidelines for endoscopic
submucosal dissection (ESD). ESD possesses several advantages over
conventional endoscopic mucosal resection, including a higher
en-bloc resection rate and more accurate pathological estimation.
It is currently gaining broad acceptance for the treatment of early
neoplastic lesions and was also proposed for the treatment of SETs
(6–9). Recently, studies on ESD for SETs
originating in the MP layer of the GI wall reported some
limitations with respect to complete resection and safety, which
may be attributed to difficulties with the endoscopic platform and
a high perforation rate (8,10,11).
Thus, the indications and utility of ESD for SETs originating
within the SM remain undetermined. There have been a number of
studies on the successful treatment of symptomatic SETs originating
in the SM and carcinoid tumors (12–15).
Endoscopic ultrasonography (EUS) is considered to be the most
accurate method for determining the size, layer of origin, margins
and echogenicity of SETs. As it is technically possible to perform
ESD for the en-bloc resection of SETs revealed by EUS as a remnant
in the SM layer, we recommend ESD as a suitable treatment for
symptomatic benign GI SETs and small carcinoid tumors originating
in the SM. In this study, we aimed to present the efficacy and
safety of ESD treatment in 12 patients with SETs originating in the
SM layer and discuss the predictors of treatment success.
Patients and methods
Selection criteria
This retrospective non-comparative study of a case
series reviewed the cases of 12 consecutive patients who underwent
ESD for SETs at Kagawa University Hospital (Kagawa, Japan) between
March, 2009 and April, 2013 and met the following selection
criteria: lesion contained within the SM layer; symptomatic SET
strongly suspected to be a benign tumor on conventional endoscopic
imaging, EUS and computed tomography (CT); confirmed histological
diagnosis of carcinoid tumor; carcinoid tumor ≤10 mm; no lymph node
or distant metastasis found prior to ESD. Ethical approval was
granted from the Ethics Committee of Kagawa University (Kagawa,
Japan). Prior written patient informed consent was obtained.
Patients
The patients (6 males and 6 females) had a mean age
of 60.4 years (range, 41–78 years) and had symptomatic benign SETs
(n=3; 1 had an esophageal hemangioma and 2 had gastric lipomas) or
small carcinoid tumors (n=9) (Table
I). In the 3 symptomatic SET cases, tissue sampling was not
performed prior to ESD. All the regions were evaluated by routine
EUS (high-frequency miniprobe, 20 MHz, UM-3R; Olympus Medical
Systems, Tokyo, Japan) and CT. In all the cases, the EUS revealed a
mass localized in the SM, which was confirmed on CT not to invade
the surrounding organs.
 | Table I.Clinicopathological data of patients
with subepithelial tumors (n=12). |
Table I.
Clinicopathological data of patients
with subepithelial tumors (n=12).
| Case | Age
(years)/gender | Location | Symptoms | Tumor size (mm) | Layer | Echoic | Pathology |
|---|
| 1 | 41/F |
Esophagus/cervical | Yes | 25 | SM | Hypo | Hemangioma |
| 2 | 76/F | Stomach/antrum | Yes | 30 | SM | Hyper | Lipoma |
| 3 | 41/F | Stomach/antrum | Yes | 20 | SM | Hyper | Lipoma |
| 4 | 64/M | Stomach/body | No | 9 | SM | Hypo | WDNET |
| 5 | 78/F | Duodenum/bulb | No | 8 | SM | Hypo | WDNET |
| 6 | 51/M | Rectum/Rb | No | 9 | SM | Hypo | WDNET |
| 7 | 63/M | Rectum/Rb | No | 7 | SM | Hypo | WDNET |
| 8 | 69/M | Rectum/Ra | No | 8 | SM | Hypo | WDNET |
| 9 | 60/F | Rectum/Rb | No | 10 | SM | Hypo | WDNET |
| 10 | 54/F | Rectum/Rb | No | 4 | SM | Hypo | WDNET |
| 11 | 64/M | Rectum/Rb | No | 2 | SM | Hypo | WDNET |
| 12 | 64/M | Rectum/Ra | No | 5 | SM | Hypo | WDNET |
ESD
ESD was performed with the use of a single-channel
scope (GIF-H260Z; Olympus Medical Systems) and an electrosurgical
unit (VIO300D; ERBE Elektromedizin GmbH, Tübingen, Germany). A
short transparent cap was attached to the tip of endoscope to
provide a constant endoscopic view and to apply tension to the
connective tissue for submucosal dissection. ESD was mainly
performed as follows: First, marker dots were placed ∼5 mm from the
lesion and, using a 23-gauge disposable needle, a submucosal
injection of several milliliters of 0.4% hyaluronate sodium
solution (MucoUp; Johnson & Johnson K.K., Tokyo, Japan) was
performed around the lesion to lift it off the MP layer. The mucosa
was then incised outside the marker dots, using a needle knife
(KD-650L or 650U; Olympus Medical Systems). The submucosal
connective tissue beneath the lesion was gradually dissected in the
SM layer directly above the muscular coat with the needle knife or
an improved insulated-tip (IT-2) knife (KD-611L; Olympus Medical
Systems). The solution was injected repeatedly during the
dissection if required. Finally, the lesion was completely resected
from the MP layer with the needle or the IT-2 knife. Hemostasis of
the large blood vessels running through the layers prior to
dissection prevented intraoperative bleeding. All patients were
administered intravenous midazolam (0.05 mg/kg) and pethidine (50
mg) prior to the procedure. All the procedures were performed by an
experienced endoscopist (H.K.: >200 successfully performed ESD
procedures). During the entire procedure bleeding was controlled
using hemostatic forceps (FD-410LR; Olympus Medical Systems). The
patients were allowed to intake a small amount of water immediately
after the treatment. If there were no complications, the patients
were permitted to intake soft food on the following day and were
discharged within 1 week.
The en-bloc resection rate, procedure time,
complications and residual local recurrence of the resected lesion
were evaluated. In addition, for the 9 small carcinoid tumors,
complete resection was histologically evaluated. An en-bloc
resection was defined as an one-piece resection including tumor
enucleation. The procedure time was measured from the time of
marker dot placement to the resection of the lesion. The
complications included the incidence of bleeding requiring blood
transfusion, perforation and intraluminal stenosis requiring
additional surgery. For the 9 small carcinoid tumors, incomplete
resection was defined as the extension of the tumor into the
lateral or vertical resection margin.
Follow-up
All patients were scheduled for follow-up by
standard endoscopy and EUS every 3 months within the first year
following treatment to confirm the healing of the artificial ulcer
and assess any residual tumor. Thereafter, follow-up continued on
an annual basis to monitor for local recurrence and other lesions.
Biopsy specimens were collected from any ulcerative lesion
identified during follow-up to histologically confirm the presence
of residual tumor and local recurrence. Abdominal and pelvic CT was
performed to assess the pararectal lymph nodes and identify distant
metastasis as deemed necessary. Three cases (1, 2 and 6) are
presented subsequently, cases 1 and 2 are rare, and therefore of
interest and case 6 is typical of cartinoid cases.
Case 1
A 41-year-old female presented with dysphagia. GI
endoscopy revealed a bluish submucosal mass (diameter, 25 mm) in
the upper esophagus. The EUS revealed a hypoechoic mass localized
in the SM layer. The mass was diagnosed as a submucosal hemangioma
of the esophagus. ESD was performed under general anesthesia after
obtaining the patient’s informed consent. Although a submucosal
vascular plexus was identified, loose connective tissue was present
in the SM directly above the muscular coat, enabling the dissection
of the target layer. There were several large blood vessels running
through the muscular coat; however, secure hemostasis with a
coagulation forceps blocked the flow in these vessels. The clear
operative field for ESD permitted the careful dissection required
to avoid rupturing the hemangioma. The resected en-bloc specimen
included a dark purple mass. The histopathological results revealed
the outgrowth of dilated blood vessels surrounded by flat
endothelial cells in the SM, leading to the diagnosis of cavernous
hemangioma. The patient has been recurrence-free for 6 months
(17).
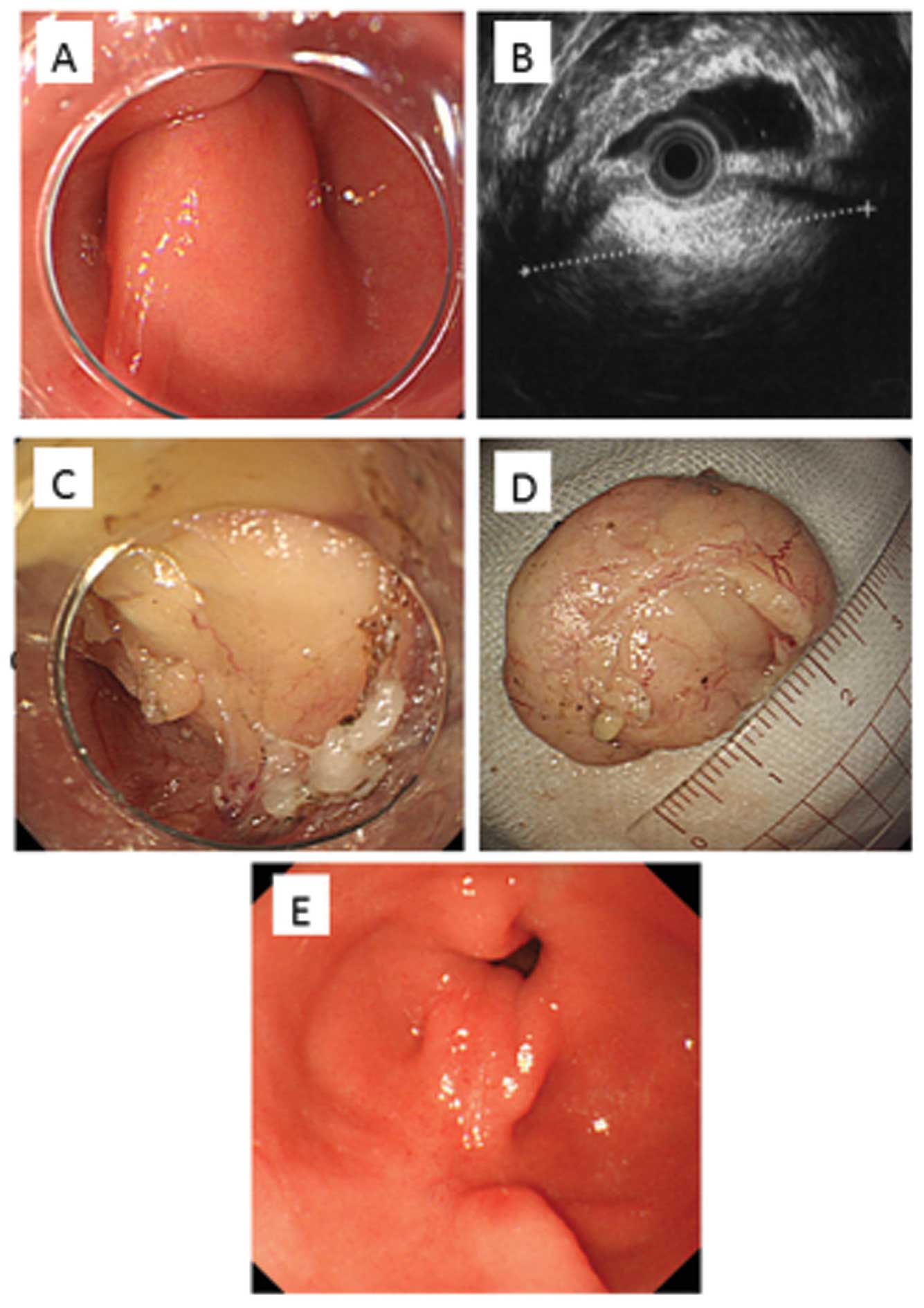
Case 2
In this case, ESD was selected as diagnostic
treatment for a symptomatic gastric SET originating in the
submucosal layer, which was ultimately proven to be a lipoma. A
75-year-old female presented with a sensation of abdominal fullness
brought on by a GI obstruction by a SET (diameter, 30 mm) in the
prepyloric area (Fig. 1A), causing
ball-valve syndrome. The EUS revealed a hyper-echoic mass localized
in the SM (Fig. 1B), although it
could not be accurately diagnosed with EUS-fine needle aspiration
(FNA). Although we recommended obtaining a tissue sample using our
method of bloc biopsy with SEMF (4), the patient opted for endoscopic
resection of the SET to relieve the abdominal fullness. After
obtaining informed consent, we selected tumor enucleation as the
minimum resection, using ESD to prevent postoperative prepyloric
stenosis. The yellowish tumor identified under a direct endoscopic
view during ESD was suggestive of a lipoma. The submucosa was
easily dissected without the need for any specific technique
(Fig. 1C) and en-bloc resection
was achieved in 41 min. The size of the tumor was 30 × 20 mm
(Fig. 1D). There were no
complications and the sensation of abdominal fullness disappeared
immediately after ESD. The follow-up endoscopy 2 months following
ESD revealed no residual tumor or gastrointestinal obstruction
(Fig. 1E). The histopathological
examination confirmed the diagnosis of a lipoma.
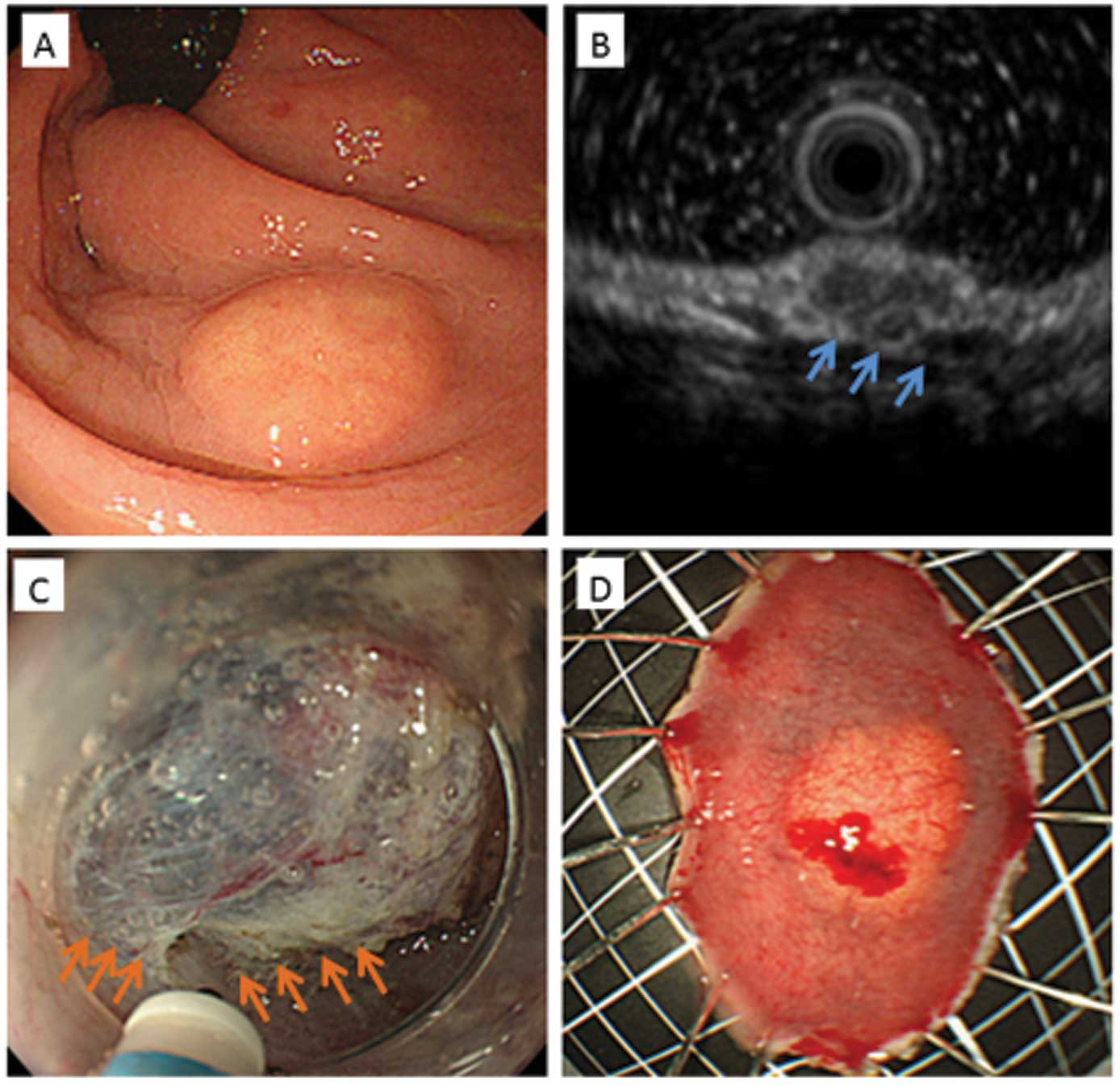
Case 6
A 51-year-old man was diagnosed with a rectal
carcinoid tumor (diameter, 9 mm) located below the rectal area
(Fig. 2A). The EUS revealed a
hypoechoic mass originating in the SM layer, with no invasion of
the MP layer (Fig. 2B). ESD was
performed using a needle knife (KD-650U; Olympus Medical Systems)
after obtaining the patient’s informed consent. The SM was
dissected immediately above the MP layer to avoid a positive
vertical resection margin (Fig.
2C). En-bloc resection was successfully completed in 52 min,
without any complications (Fig.
2D). The histological examination confirmed the diagnosis of a
rectal carcinoid tumor, classified as a well-differentiated
neuroendocrine tumor, and a negative resection margin. The patient
has been recurrence-free for 6 months.
Results
Clinical outcome and complications
The clinical outcomes according to the endoscopic
treatment modality are summarized in Table II. The entire procedure was
successfully completed in all the patients. En-bloc resection was
performed in all 12 cases and the mean procedure time was 45 min
(range, 20–120 min). There were no reported complications during or
after the procedure and there were no cases of intraluminal
stenosis requiring additional surgery.
| Table II.Clinical outcomes according to the
endoscopic treatment modality (n=12). |
Table II.
Clinical outcomes according to the
endoscopic treatment modality (n=12).
| Case | Pathology | Procedure time
(min) | Complete
resection | Complications | Follow-up period
(months) | Recurrence | Additional
surgery |
|---|
| 1 | Hemangioma | 120 | Yes | No | 6 | No | No |
| 2 | Lipoma | 41 | Yes | No | 4 | No | No |
| 3 | Lipoma | 32 | Yes | No | 18 | No | No |
| 4 | WDNET | 37 | Yes | No | 36 | No | No |
| 5 | WDNET | 63 | Yes | No | 2 | No | No |
| 6 | WDNET | 52 | Yes | No | 4 | No | No |
| 7 | WDNET | 30 | Yes | No | 13 | No | No |
| 8 | WDNET | 49 | Yes | No | 35 | No | No |
| 9 | WDNET | 37 | Yes | No | 39 | No | No |
| 10 | WDNET | 28 | Yes | No | 2 | No | No |
| 11 | WDNET | 31 | Yes | No | 1 | No | No |
| 12 | WDNET | 20 | Yes | No | 1 | No | No |
Follow-up and histopathology
The median follow-up was 13.4 months (range, 1–39
months) and there was no reported recurrence or disease-related
mortality during the follow-up period. Histopathologically,
curative resection was achieved in all 9 carcinoid tumor cases,
which were all classified as well-differentiated neuroendocrine
tumors (proliferation index <2%).
Discussion
There is currently no consensus on the optimal
strategy for the endoscopic treatment of SETs. Endoscopic
submucosal resection (ESMR) has been reported to be effective for
the treatment of SETs (12–15)
and it is usually reserved for lesions that are confined to the
submucosal or mucosal layers, due to the increased risk of
perforation associated with ESMR of lesions originating in the MP
layer. However, ESMR occasionally requires a large en-bloc
resection and secure hemostasis may prove challenging. Recently,
ESD, which was developed from the endoscopic mucosal resection
method, was introduced as a novel method of endoscopic treatment
that allows for such resection and hemostatic management, as well
as precise histological staging. ESD may also be more effective in
preventing disease recurrence compared to the conventional ESMR.
Indeed, there are already available studies on the successful
application of the ESD procedure for the diagnostic treatment of
several types of GI SETs, such as lipomas and carcinoids (16–19).
We recommend ESD as a suitable treatment for
symptomatic SET with gastrointestinal obstruction. In the present
study, the treatment of symptomatic benign SETs (1 esophageal
hemangioma and 2 gastric lipomas) was successful and the symptoms
were eliminated. Moreover, we previously reported the first case of
a submucosal esophageal hemangioma successfully removed en-bloc by
ESD (17). Since conventional
endoscopic therapy, such as ESMR, has been associated with the risk
of bleeding and recurrence of hemangiomas (20), en-bloc removal by ESD may prove to
be a viable treatment option in these cases. Furthermore, ESD
treatment may be indicated if EUS and CT reveal that the tumors are
confined to the SM layer, without large inflow vessels. In
addition, radical ESD treatment was possible in 2 cases of
symptomatic gastric lipomas in the present study. In case 2,
considering the issue of postoperative pyloric stenosis, we
performed tumor enucleation with minimum resection using ESD.
Endoscopic observation at 3 months postoperatively revealed healing
of the surgical site with scar formation, but without deformation
or stenosis. This suggests that, if preoperative diagnostic imaging
reveals a typical lipoma, tumor enucleation that takes into account
postoperative stenosis may be an effective treatment option.
ESD may be the optimal treatment method for
symptomatic SETs originating in the SM layer, since it allows for
secure hemostasis and en-bloc resection under direct vision.
Indeed, the efficacy of endoscopic treatment using ESD for SETs,
mainly GISTs, originating in the MP layer of the GI tract was
previously reported (8,10,11).
However, since GI full-thickness layers must be resected to treat
SETs in the MP layer, the site must be securely closed and the
vasculature in all the layers must be carefully managed. There is
also a limit to the en-bloc resection that may be performed without
damaging the tumor in a narrow operative field accessible through a
small opening. Three case series with similar inclusion criteria
and methods reported comparable rates of successful en-bloc
resection for SETs originating in the MP layer (61–68%) and severe
complications due to perforation (5.4, 0 and 12%, respectively)
(8,21,22).
Therefore, minimally invasive local resection techniques, such as
NOTES, appear to be suitable for the treatment of SETs originating
from the MP layer (2,3).
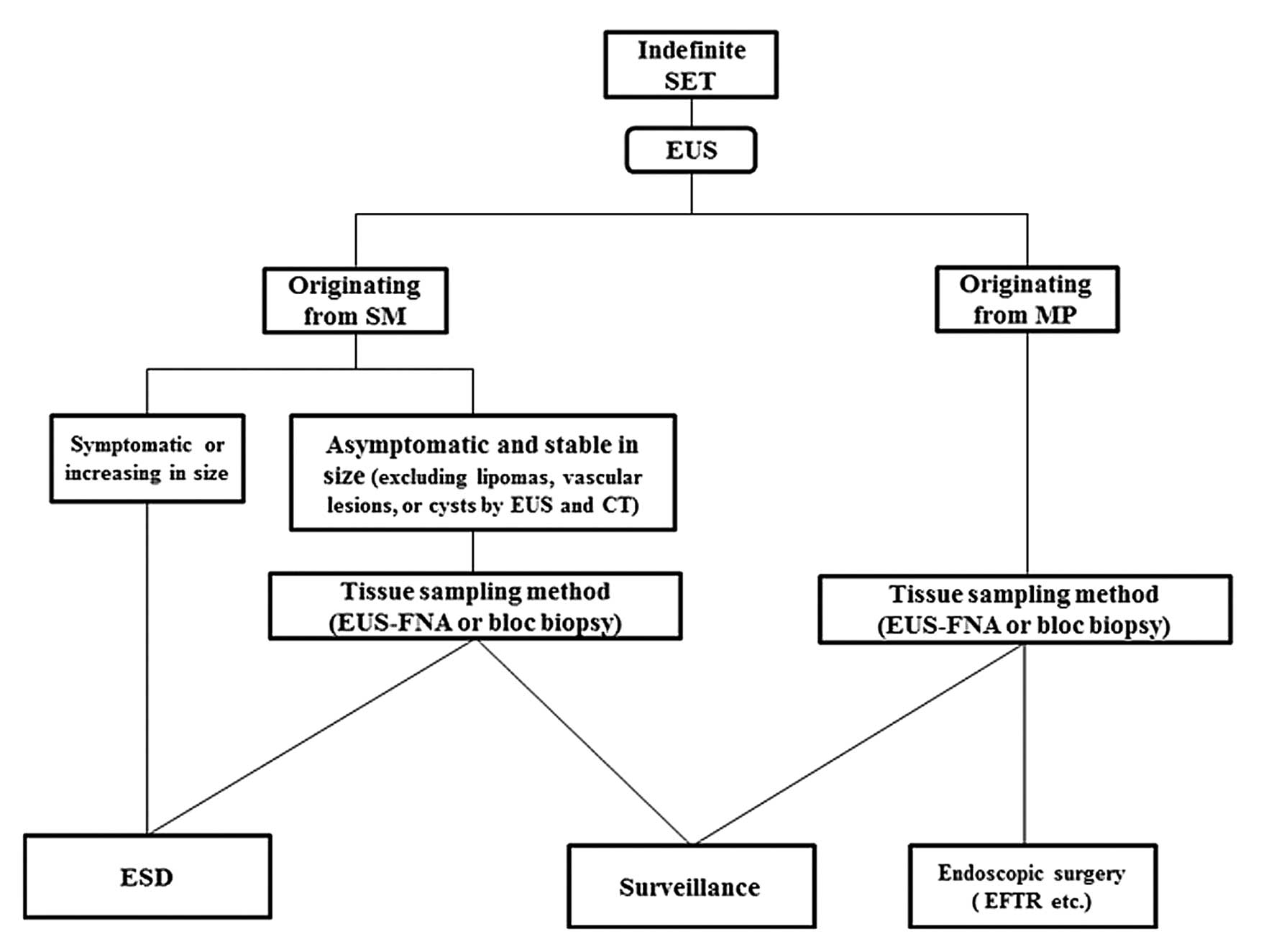
We recommend the algorithm presented in Fig. 3 for the management of indefinite
SETs, except carcinoid tumors. As was demonstrated by the present
study, ESD may be the treatment of choice for symptomatic SETs or
SETs increasing in size, when found to be originating in the SM
layer on EUS. For asymptomatic SETs and SETs stable in size
originating in the SM layer (excluding lipomas, vascular lesions or
cysts identified on EUS and CT), tissue sampling methods, such as
EUS-FNA or bloc biopsy with SEMF, are recommended. According to the
histological findings, surveillance or ESD treatment may be
selected. If a SET originating in the MP layer is identified on
EUS, tissue sampling is recommended to distinguish GISTs from other
benign tumors (e.g., leiomyoma and schwannoma). Minimally invasive
local resection, such as EFTR, is recommended if the lesion is
confirmed to be a GIST. If tissue sampling methods reveal a benign
SET, surveillance over the short term is not required.
As regards the possibility of ESD treatment for
carcinoid tumors, tumor size is considered to be the most important
factor associated with the metastasis of rectal carcinoid tumors
(23,24). Endoscopic treatment is considered
to be curative for small carcinoid tumors (<10 mm) with an
extremely low risk of metastasis (23,24).
However, there is still some controversy over the optimal
endoscopic method for the resection of rectal carcinoid tumors.
Endoscopic treatment for carcinoid tumors requires special
techniques for deeper resection to achieve clear margins, since
∼75% of the tumors extend into the SM layer (25). Conventional ESMR was found to allow
for a lower rate of en-bloc resection, particularly with respect to
the vertical margin (26);
therefore, to improve resectability, an ESMR technique utilizing a
ligation device was designed and found to achieve a significantly
deeper vertical resection margin and a higher curative resection
rate (15). More recently, ESD was
reported to be an effective method for the treatment of rectal
carcinoid tumors (18,19).
The advantages of ESD over previously used treatment
methods for carcinoids are significant. Firstly, ESD achieves clear
vertical resection margins by dissecting the SM immediately above
the MP layer. Secondly, ESD enables precise histological assessment
of the resected specimen. For these reasons, we recommend ESD as
the most suitable method for the treatment of carcinoid tumors of
the SM. In our study, histopathological curative resection by ESD
was achieved without complications in all 9 cases of carcinoid
tumors, although the mean procedure time was longer (38.6 min)
compared to that reported by previous studies (18,19,26).
This may be attributed to the longer time required to achieve a
clear vertical margin while avoiding perforation; however, this
also resulted in the absence of any complications. However, ESD may
involve certain risks due to its technical difficulties; in
addition, it may be more time-consuming. Therefore, only
experienced endoscopists should perform ESD treatment for
carcinoids. In this study, none of the cases exhibited tumor
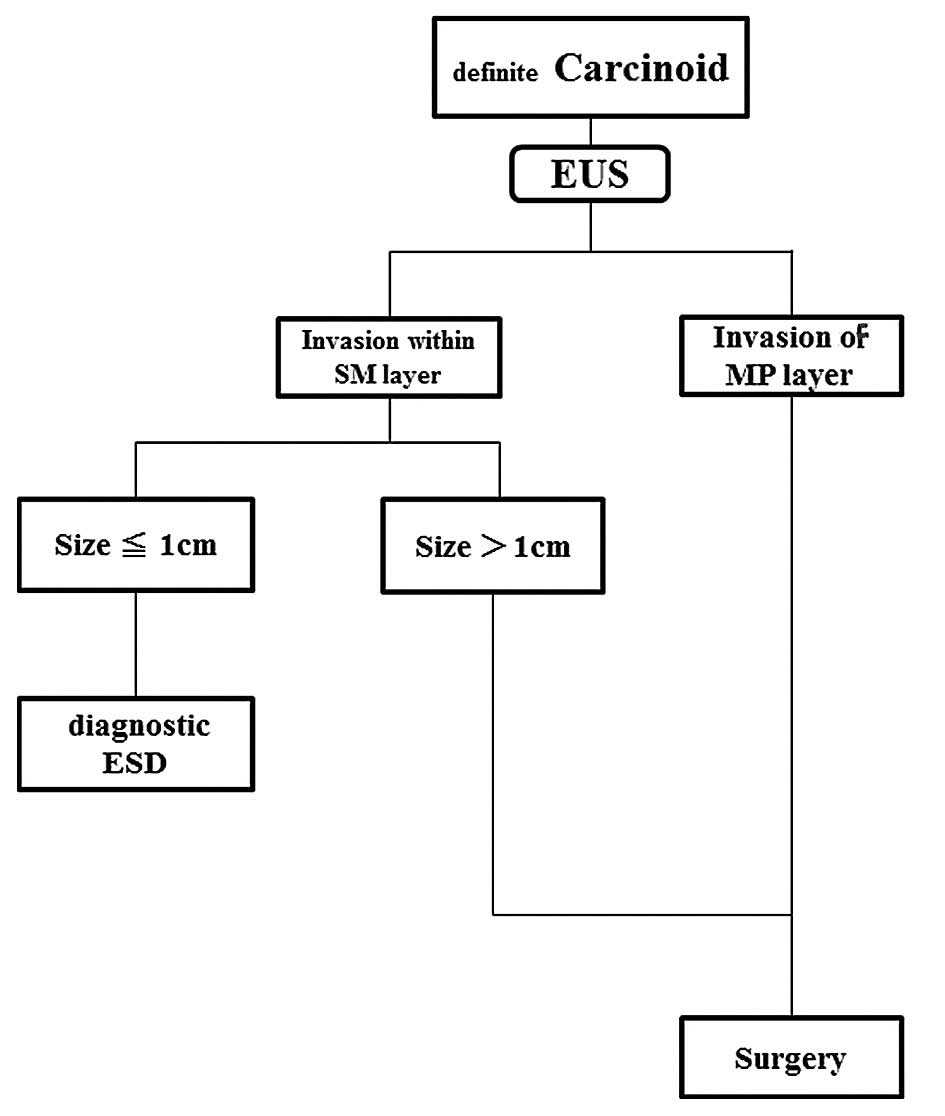
recurrence during follow-up. We suggest the algorithm presented in
Fig. 4 for the management of
definite carcinoids. Diagnostic ESD is recommended for small
carcinoid tumors (<10 mm) when EUS reveals tumor invasion within
the SM. If histology indicates that ESD was not curative,
additional surgery is required. Conventional surgery is recommended
for carcinoid tumors >10 mm in size or when EUS reveals tumor
invasion of the MP layer. In the case of rectal carcinoid tumors,
however, those sized <10 mm were reported to result in <2%
chance of metastasis (27).
Careful follow-up is required to detect any local recurrence, as
complete removal may be possible in repeat procedures. In carcinoid
tumors sized <10 mm, further prospective studies are required to
determine the feasibility of ESD, the long-term recurrence rates
and patient survival. The advantages of the present study are that
it suggests novel indications and the validity of ESD treatment for
symptomatic SETs and carcinoid tumors <10 mm in size that
originate in the SM, as well as the inclusion of a novel strategy
based on flowcharts for SETs and carcinoid tumors. However, the
limitation of the present study was that it was a single-center,
non-comparative study with a small sample size. Therefore, larger
scale prospective studies are required to verify our findings.
In conclusion, if EUS reveals a SET originating in
the SM layer, without infiltration of the MP layer, and resection
is required to alleviate abdominal symptoms, the minimally invasive
ESD procedure may be considered as a feasible diagnostic treatment
option.
References
|
1.
|
Mazur MT and Clark HB: Gastric stromal
tumors. Reappraisal of histogenesis. Am J Surg Pathol. 7:507–519.
1983. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Mori H, Kobara H, Kobayashi M, et al:
Establishment of pure NOTES procedure using a conventional flexible
endoscope: review of six cases of gastric gastrointestinal stromal
tumor. Endoscopy. 43:631–634. 2011. View Article : Google Scholar
|
|
3.
|
von Renteln D, Rosch T, Kratt T, et al:
Endoscopic full-thickness resection of submucosal gastric tumors.
Dig Dis Sci. 57:1298–1303. 2012.PubMed/NCBI
|
|
4.
|
Kobara H, Mori H, Fujihara S, et al: Bloc
biopsy by using submucosal endoscopy with a mucosal flap method for
gastric subepithelial tumor tissue sampling (with video).
Gastrointest Endosc. 77:141–145. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
de la Serna-Higuera C, Perez-Miranda M,
Diez-Redondo P, et al: EUS-guided single-incision needle-knife
biopsy: description and results of a new method for tissue sampling
of subepithelial GI tumors (with video). Gastrointest Endosc.
74:672–676. 2011.PubMed/NCBI
|
|
6.
|
Ono H, Kondo H, Gotoda T, et al:
Endoscopic mucosal resection for treatment of early gastric cancer.
Gut. 48:225–229. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Katoh T, Itoh Y, Mohri T, et al:
Endoscopic enucleation of gastrointestinal stromal tumors of the
stomach: report of five cases. World J Gastroenterol. 14:2609–2611.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Bialek A, Wiechowska-Kozlowska A,
Pertklewicz J, et al: Endoscopic submucosal dissection for
treatment of gastric subepithelial tumors (with video).
Gastrointest Endosc. 75:276–286. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Rosch T, Sarbia M, Schumacher B, et al:
Attempted endoscopic en bloc resection of mucosal and submucosal
tumors using insulated-tip knives: a pilot series. Endoscopy.
36:788–801. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Bialek A, Wiechowska-Kozlowska A and Huk
J: Endoscopic submucosal dissection of large gastric stromal tumor
arising from muscularis propria. Clin Gastroenterol Hepatol.
8:e119–e120. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Inoue H, Ikeda H, Hosoya T, et al:
Submucosal endoscopic tumor resection for subepithelial tumors in
the esophagus and cardia. Endoscopy. 44:225–230. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Hyun JH, Jeen YT, Chun HJ, et al:
Endoscopic resection of submucosal tumor of the esophagus: results
in 62 patients. Endoscopy. 29:165–170. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Kojima T, Takahashi H, Parra-Blanco A, et
al: Diagnosis of submucosal tumor of the upper GI tract by
endoscopic resection. Gastrointest Endosc. 50:516–522. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Waxman I, Saitoh Y, Raju GS, et al:
High-frequency probe EUS-assisted endoscopic mucosal resection: a
therapeutic strategy for submucosal tumors of the GI tract.
Gastrointest Endosc. 55:44–49. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Ono A, Fujii T, Saito Y, et al: Endoscopic
submucosal resection of rectal carcinoid tumors with a ligation
device. Gastrointest Endosc. 57:583–587. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Yoshida T, Fujisaki J, Suganuma T, et al:
Successful en bloc resection of a 5 cm symptomatic sessile gastric
lipoma by endoscopic submucosal dissection. Dig Endosc. 24:2822012.
View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Kobara H, Mori H and Masaki T: Successful
en bloc resection of an esophageal hemangioma by endoscopic
submucosal dissection. Endoscopy. 44(Suppl 2): E134–E135. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Lee DS, Jeon SW, Park SY, et al: The
feasibility of endoscopic submucosal dissection for rectal
carcinoid tumors: comparison with endoscopic mucosal resection.
Endoscopy. 42:647–651. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Park HW, Byeon JS, Park YS, et al:
Endoscopic submucosal dissection for treatment of rectal carcinoid
tumors. Gastrointest Endosc. 72:143–149. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Urakami T, Kondo K, Kasugai T, et al: A
case of recurrent esophageal cavernous hemangioma increasing
rapidly after surgery. Jpn J Thorac Cardiovasc Surg. 46:1206–1210.
1998.(In Japanese).
|
|
21.
|
Lee IL, Lin PY, Tung SY, et al: Endoscopic
submucosal dissection for the treatment of intraluminal gastric
subepithelial tumors originating from the muscularis propria layer.
Endoscopy. 38:1024–1028. 2006. View Article : Google Scholar
|
|
22.
|
Hwang JC, Kim JH, Kim JH, et al:
Endoscopic resection for the treatment of gastric subepithelial
tumors originated from the muscularis propria layer.
Hepatogastroenterology. 56:1281–1286. 2009.PubMed/NCBI
|
|
23.
|
Park CH, Cheon JH, Kim JO, et al: Criteria
for decision making after endoscopic resection of
well-differentiated rectal carcinoids with regard to potential
lymphatic spread. Endoscopy. 43:790–795. 2011. View Article : Google Scholar
|
|
24.
|
Soga J: Carcinoids of the rectum: an
evaluation of 1,271 reported cases. Surg Today. 27:112–119. 1997.
View Article : Google Scholar
|
|
25.
|
Matsumoto T, Iida M, Suekane H, et al:
Endoscopic ultrasonography in rectal carcinoid tumors: contribution
to selection of therapy. Gastrointest Endosc. 37:539–542. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Zhou PH, Yao LQ, Qin XY, et al: Advantages
of endoscopic submucosal dissection with needle-knife over
endoscopic mucosal resection for small rectal carcinoid tumors: a
retrospective study. Surg Endosc. 24:2607–2612. 2010. View Article : Google Scholar
|
|
27.
|
Modlin IM, Oberg K, Chung DC, et al:
Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol.
9:61–72. 2008. View Article : Google Scholar
|