Introduction
Chemotherapy-induced alopecia (CIA) is one of the
most traumatic side effects of chemotherapy for women with ovarian
cancer (1). This trauma is
accentuated by cancer recurrence (2,3). A
literature review of the effects of CIA on the quality of life
confirms that alopecia is a growing concern among women undergoing
chemotherapy (4), possibly due to
the increased preoccupation with appearance in modern society.
Hair is closely linked to a person’s identity. Women
have described baldness as a sign of weakness, which may lead to
depression and low self-esteem. Alopecia is a constant reminder of
the cancer diagnosis for the afflicted individual and a
stigmatizing sign of cancer that is difficult to disguise (5), occasionally leading to social
withdrawnness (6). Baldness may
also be associated with loss of attractiveness, which in turn may
affect sexual relations (2). Women
have expressed fears of being rejected by their partners due to
alopecia (7).
CIA is caused by the effects of the chemotherapeutic
drug on the hair follicles that continuously receive blood supply
from the superficial scalp arteries. Currently, the main approach
to minimizing CIA is scalp cooling (8). The rationale of scalp cooling is to
achieve a vasoconstriction of the peripheral blood vessels, which
leads to a reduction of the drug supply to the hair follicles
(9) and decreased intracellular
metabolism (10). Earlier findings
suggested that, at a depth of 1–2 mm in the scalp, the temperature
should be reduced to at least 22°C to obtain a hair-preserving
effect (11). Cooke et al
(12) reported that the average
scalp temperature in patients with severe alopecia was 25.6°C.
Bulow et al (10) cooled
the scalp of 10 healthy volunteers and measured the blood flow to
the frontal region by injecting 133Xe. The authors of
that study observed that a subcutaneous temperature of 22°C
corresponded to a surface temperature of 19°C. However, since then,
investigations on the optimal degree of hypothermia of the scalp
surface in order to achieve a sufficient vasoconstriction for hair
preservation have been limited (13).
Over the last decades, different cooling techniques
of the scalp to decrease CIA have been used in the clinical
setting. The previously used cooling methods (crushed ice, frozen
cryogel caps and cold-air cooling) were temperature-unstable,
uncomfortable for the patient and time-consuming for staff.
Furthermore, these older techniques demonstrated no conclusive
evidence with regard to the reduction of alopecia (9). More recently, a computerized
technique with a cooling unit similar to a refrigerator has been
used to regulate the pre-set temperature. This technique has also
been used in our department for research purposes and in the
clinical setting since 2003. Over 300 patients have been treated
with these cooling machines and our clinical experience is that
this technique significantly reduces hair loss. Therefore, it
appeared worthwhile to further refine this technique, increase our
knowledge regarding the optimal temperature and treatment time
required and make scalp cooling an efficient method for reducing
hair loss and preserving the self-image of the patient.
The study was divided into two parts: the first part
(pre-study) aimed to assess which pre-set temperature (3 or 8°C)
was the most effective in achieving a subcutaneous temperature of
<22°C in healthy volunteers. The temperature variations within
and among the participants at the baseline and during the cooling
procedure and the temperature variations associated with different
regions of the scalp were also investigated.
The aim of the second part of the study (main study)
was to compare the extent of CIA in patients undergoing scalp
cooling after 4 cycles of paclitaxel in combination with
carboplatin. The collective aim of the study was to determine which
temperature (3 or 8°C) was the most effective in preventing hair
loss and the most tolerable to the patients.
Materials and methods
Pre-study
This study was conducted at the Department of
Gynecological Oncology, Örebro University Hospital, Sweden. Data
collection was initiated in 2005 and continued until 2007. A group
of 5 healthy female volunteers underwent scalp cooling and
participated in three sessions of scalp temperature measurements
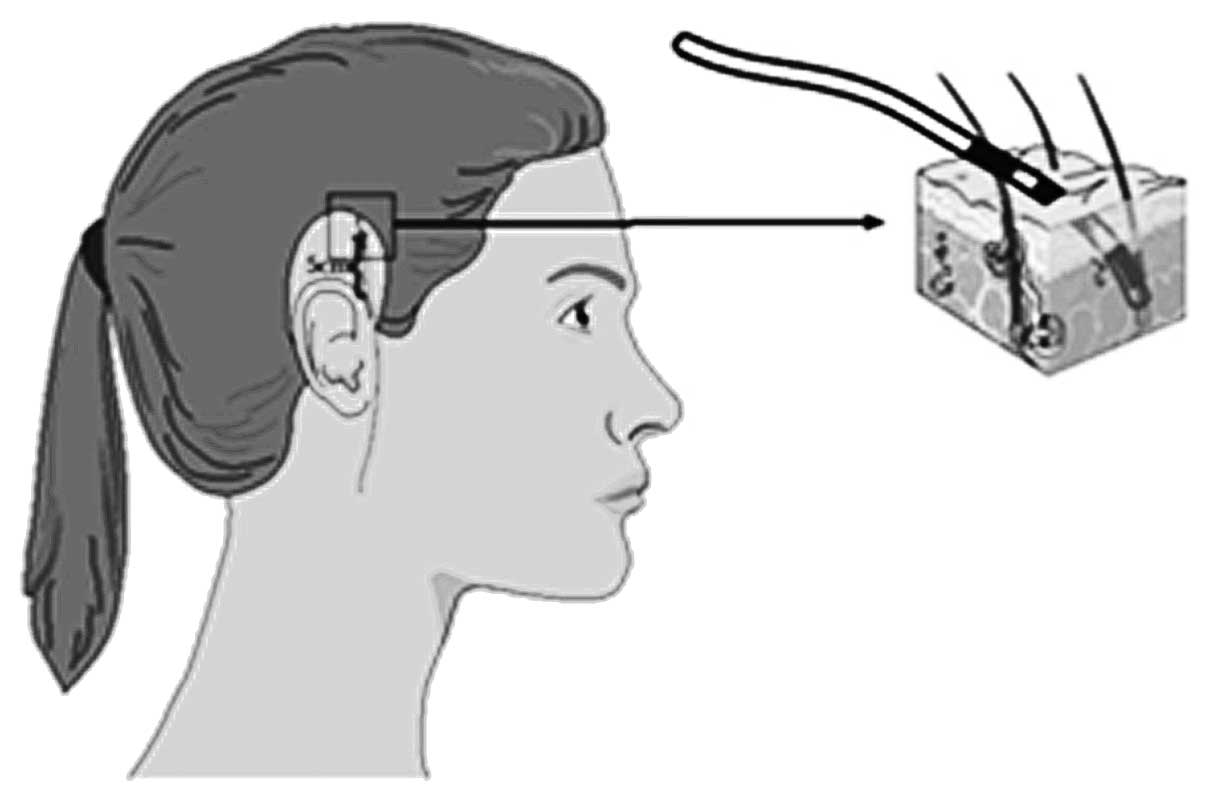
(Table I). Following wetting of
the hair, a peripheral venous catheter, 1.3 mm in diameter, was
inserted into the scalp in parallel with the skin surface. The
steel needle was removed and the grip of the plastic catheter was
cut off, leaving 2.5 cm of the plastic catheter visible, with 0.7
cm remaining inside the scalp.
 | Table I.Five healthy females underwent scalp
cooling and participated in three sessions of scalp temperature
measurements. |
Table I.
Five healthy females underwent scalp
cooling and participated in three sessions of scalp temperature
measurements.
| Variables | Measurement I | Measurement II | Measurement III |
|---|
| Time for data
collection | May–June, 2006 | September, 2006 | March, 2007 |
| Machine
Dignicap™ | Manufactured in
2002 | Manufactured in
2006 | Manufactured in
2006 |
| Sample | 5 participants | 5 participants | 5 participants |
| Age (years) | 47–63 | 47–63 | 47–63 |
| Pre-set temperature
(°C) | 8 | 3 | 8 |
| Site of probe on the
head | Top, right side,
back | Right side | Right side |
| Registration
interval | Every other sec
during 1 h | Every other sec
during 1 h | Every other sec
during 1 h |
Probes for scalp temperature measurement were placed
into the catheter and affixed with transparent surgical tape. The
tip of each probe was estimated to be at a depth of 1–2 mm, which
coincides with the location of the hair follicles. During
measurements II and III, the probes were placed on the right side
of the head, which was found to be a temperature-stable region.
Instruments
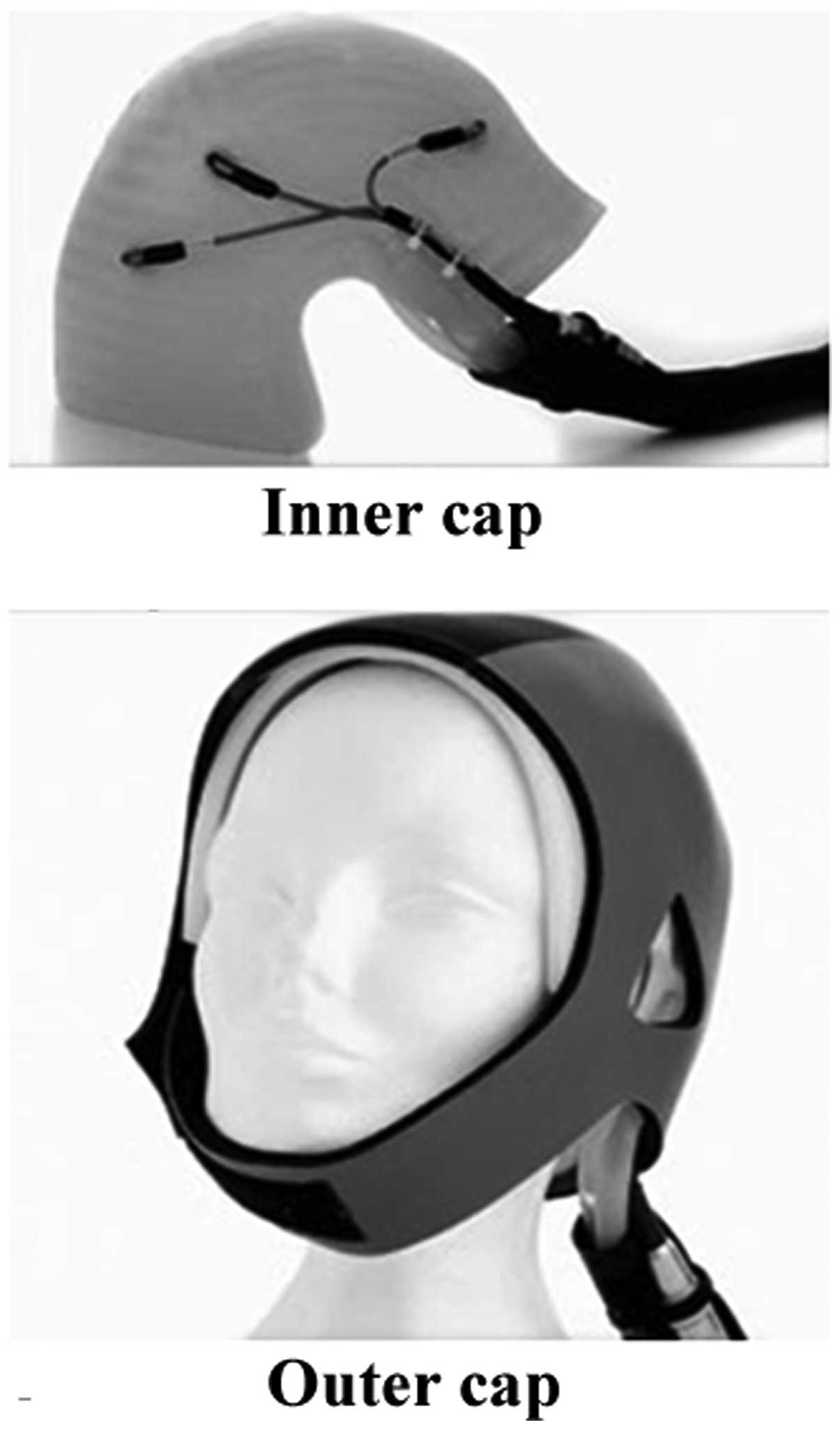
Dignitana™ equipment was used. The pre-set
temperature was recorded by 3 sensors inside the silicone cap
(Fig. 1) and was visible on the
monitoring screen of the machine. During the cooling procedure, a
coolant medium consisting of circulating water and glycol
circulated in the labyrinthine channels (interspaced at 7 mm) of an
inner cap of silicone in a sealed system. A tight-fitting outer cap
made of elastic neoprene was placed on the head of the volunteers
and the patients. The Venflon™ Pro catheters, the HT 41019 probes
with 3 sensors and an ATS-101 thermometry system used to record the
temperatures, were purchased from Lund Science AB (Lund,
Sweden).
The probes on the right side of the head were placed
5 cm above the crease of the earlobe. The other probes (top and
back of the head) were placed in vertical and horizontal positions,
aligned with the probes on the right side. The locations of the
probes are shown in Fig. 2.
The overall cooling procedure was adjusted to the
clinic’s routines and was conducted in a well-ventilated
two-patient wardroom. The best-fitted cooling cap was placed on the
moistened hair of each volunteer. The scalp of the volunteer was
cooled and the procedure lasted for 1 h. The temperatures selected
for the test were 3 and 8°C, which were on both sides of the
clinically used temperature of 5°C, and were allowed a fluctuation
of ±1.5°C (which was the level of exactness provided by the
manufacturer), without trespassing each other. Plus 3°C was the
lowest stable temperature possible to pre-set on the machine
according to our prior pre-tests. Multiple pre-measurements were
performed to test different sites of the head and assess the
response of the scalp temperature when selecting different pre-set
temperatures between 3 and 11°C.
Main study
Patients who preferred scalp cooling and who met the
inclusion criteria were consecutively invited to participate in the
study. The chemotherapy regimen used in this study was a
combination of paclitaxel and carboplatin. Paclitaxel is a highly
potent drug that causes severe alopecia, whereas carboplatin is
associated with a low risk of alopecia (14). The majority of the patients had a
confirmed diagnosis of ovarian carcinoma and the remaining patients
had endometrial carcinoma. The characteristics of the 43 evaluable
patients are presented in Table
II. This part of the study was conducted between November, 2007
and May, 2011.
| Table II.Patient characteristics of the main
study. |
Table II.
Patient characteristics of the main
study.
| Variables | No. | Mean (range) |
|---|
| Age (years) | | |
| All patients | 43 | 64.3 (38–84) |
| 3°C | 20 | 65.6 (38–84) |
| 8°C | 23 | 63.1 (46–82) |
| Diagnosis | | |
| Ovarian cancer | 22 | - |
| Endometrial
cancer | 17 | - |
| Cervical
cancer | 2 | - |
| Tubal cancer | 1 | - |
| Peritoneal
cancer | 1 | - |
Inclusion criteria
The inclusion criteria of the present study were as
follows: i) patients with gynecological cancer initiated on a
chemotherapy session of paclitaxel (175 mg/m2) in
combination with carboplatin (AUC 5–6); ii) patients who understood
Swedish; and iii) patients who signed an informed consent.
Exclusion criteria
The exclusion criteria of the present study were as
follows: i) patients with previous alopecia; ii) patients who had
received chemotherapy in the previous 12 months; and iii) patients
who were considered ineligible for scalp cooling by the
physician.
Randomization
After signing an informed consent, the patients were
randomized to either the 3 or the 8°C group via numbered, sealed
envelopes. The member of the staff responsible for applying the
cooling cap contacted the person responsible for the storage of the
envelopes prior to each course of treatment. The same temperature
was used for each consecutive session.
Blinding
The member of the staff who applied the cap and
managed the cooling procedure was made aware of the pre-set
temperature. The patient, the nurse who administered the
chemotherapy and the persons who evaluated the photos were blinded
to the pre-set temperature.
Ethical consideration
All procedures were conducted in accordance with the
Helsinki Agreement (World Medical Association Declaration of
Helsinki, 2002). The project was conducted in accordance with the
Consolidated Guidelines on Good Clinical Practice (International
Conference on Harmonization of Technical Requirements for
Registration of Pharmaceuticals for Human Use, 1997). The study was
approved by the Regional Ethics Committee in Uppsala-Örebro (Dnr
2005:082).
Procedure
The entire procedure was conducted by skilled and
experienced staff. Images (digital and paper) of the crown of the
head were captured prior to each cycle and labeled with code
numbers and dates. The hair was moistened and the randomized
temperature was registered on the screen of the machine. The scheme
for this course was in alignment with the clinical practice. The
scalp was cooled with the Dignitana technique, as described above.
The pump-driven paclitaxel infusion was initiated 30 min after the
scalp cooling and lasted for 3 h. Directly after the paclitaxel
infusion was stopped, the carboplatin infusion was administered
over 30–60 min. The cooling cap was retained for 1.5 h after the
paclitaxel infusion had stopped. The procedure lasted for ∼5 h and
the patients were connected to the machine during the whole
time.
Data recording
The estimated hair loss of the patients and their
experience of the cooling procedure was recorded. The captured
images were stored in a memory card and transformed to Microsoft
Picture Manager. The temperature registration by the sensors in the
cold cap was stored in a personal coded disk. The content of the
disks was transferred to a CD, in which all the patient temperature
curves were stored. The patients were asked to complete a
questionnaire regarding headache and coldness following each
treatment session.
Evaluation of temperature graphs
The two investigators assessed the graphs from each
cycle of all the patients to determine whether the temperature
variation exceeded ±1.5°C. The recorded temperatures varied within
a margin of ±1.5°C in 64 of the 108 measurements (59%), whereas 44
measurements deviated from the margin of ±1.5°C. In 15
measurements, the recorded temperature was occasionally >1.5°C
of the pre-set temperature and in 26 measurements the corresponding
temperature was recorded to be <1.5°C. Three measurements
exhibited variations >1.5°C on both sides. These patients were
all included in the analysis, since the variations were only one or
more rapid peaks. After 30 min of cooling, a steady-state was
achieved.
Patients’ subjective evaluation
The patients estimated their own hair loss in a
questionnaire prior to the second and the following treatments.
Following the removal of the cooling cap, the patient rated the
experience of headache and/or coldness during the cooling
procedure. The patients assessed their hair loss and discomfort on
a visual analogue scale (VAS). The VAS was graded 0–10, with 0
indicating no hair loss or no discomfort and 10 as total hair loss
or the most severe discomfort.
Evaluation of images
The images were separately evaluated by two
investigators, E.E. and L.N., using the VAS with 0–10 grading. All
the images were compared for each patient in line, with 0
corresponding to no hair loss and 10 to total hair loss. There was
a significant coherence in the evaluations; whenever there was a
difference of opinions, a consensus was reached.
Hypothesis
We hypothesized that 65% of patients would retain
80% of their hair at a pre-set temperature of 3°C and 35% would
retain 80% of their hair at a pre-set temperature of 8°C.
Statistical analysis
The mean values and standard deviations (SDs) were
calculated for the VAS scores. The differences were assessed by the
Student’s t-test and repeated analysis of variance (ANOVA) measures
(intergroup differences and time dependence). The differences
regarding hair loss of >50% or the use of a wig were assessed by
the Pearson’s Chi-square test. The Wilcoxon matched-pairs test was
used to compare the VAS scores of the patients and the
investigators. Kappa test statistics was used to compare the
inter-rater agreement reliability. The statistical analyses were
performed with STATISTICA software, version 11, 2012 (StatSoft,
Inc., Tulsa, OK, USA).
Results
Pre-study
The main finding of the pre-study was that a
temperature of 3°C of the coolant tended to be most effective in
achieving a subcutaneous temperature of <22°C. With this pre-set
temperature, 4 of the 5 volunteers reached a subcutaneous
temperature of <22°C following 30 min of cooling, whereas with a
pre-set temperature of 8°C, only 2 volunteers reached a
subcutaneous temperature of <22°C. The results were identical
after 60 min of cooling (Table
III).
| Table III.Measurements II and III. |
Table III.
Measurements II and III.
| A, Measurement II,
subcutaneous temperature (°C), right side of the scalp, 3°C
group |
|
| Subject | Baseline | 30 min | 60 min |
|
| A | 34.03 | 19.14 | 17.38 |
| B | 33.60 | 24.12 | 23.56 |
| C | 32.27 | 16.86 | 14.68 |
| D | 32.93 | 16.29 | 15.36 |
| E | 29.95 | 10.24 | 10.53 |
|
| B, Measurement III,
subcutaneous temperature (°C), right side of the scalp, 8°C
group |
|
| Subject | Baseline | 30 min | 60 min |
|
| A | 33.96 | 24.76 | 22.37 |
| B | 33.64 | 27.63 | 25.00 |
| C | 32.88 | 18.96 | 18.41 |
| D | 34.76 | 19.68 | 18.18 |
| E | 33.88 | 23.15 | 22.30 |
In measurement I, the response to cooling in various
regions of the scalp was investigated. The results demonstrated
that the top of the head (vertex) was less responsive. The baseline
subcutaneous temperature in this area was higher in 3 of the 5
volunteers and this difference was observed after 30 and 60 min of
cooling in 4 of the 5 volunteers (Table IV).
| Table IV.Measurement I, subcutaneous
temperatures (°C) at various regions of the scalp, pre-set
temperature 8°C. |
Table IV.
Measurement I, subcutaneous
temperatures (°C) at various regions of the scalp, pre-set
temperature 8°C.
| Subject | Scalp region | Baseline | 30 min | 60 min |
|---|
| A | Back | 34.54 | 24.98 | 22.37 |
| Top | 36.09 | 32.89 | 31.98 |
| Right side | 34.28 | 23.89 | 22.79 |
| B | Back | 25.29 | Lost | Sensor |
| Top | 33.40 | 20.55 | 20.66 |
| Right side | 34.97 | 22.58 | 20.98 |
| C | Back | 33.24 | 16.47 | 16.07 |
| Top | 36.22 | 30.97 | 30.15 |
| Right side | 35.97 | 22.40 | 22.07 |
| D | Back | 34.58 | 24.61 | 23.77 |
| Top | 35.10 | 30.78 | 30.24 |
| Right side | 35.55 | 23.40 | 21.35 |
| E | Back | 34.61 | 25.77 | 24.28 |
| Top | 35.95 | 30.06 | 29.92 |
| Right side | 34.55 | 20.44 | 20.18 |
The difference in scalp temperature at the baseline
prior to cooling varied within individuals and among individuals
during each measurement session. The baseline temperature exhibited
a maximum variation of 3.7°C among the 5 volunteers (Table V).
| Table V.Subcutaneous baseline temperatures
(°C), right side. |
Table V.
Subcutaneous baseline temperatures
(°C), right side.
| Subject | Measurements
|
|---|
| I | II | III |
|---|
| A | 34.28 | 34.03 | 33.96 |
| B | 34.97 | 33.60 | 33.64 |
| C | 35.97 | 32.27 | 32.88 |
| D | 35.55 | 32.93 | 34.76 |
| E | 34.55 | 29.95a | 33.88 |
The results of our pre-tests demonstrated that the
change in the pre-set temperature was not linearly associated with
the subcutaneous temperature.
Main study
A total of 47 patients were included in the study
and 43 patients were evaluable after 1 cycle of chemotherapy. Of
the 4 patients who completed cycle 1, 3 patients developed
anaphylactic reactions to chemotherapy and 1 patient underwent a
change in the regimen. The reasons for discontinuation during the
following cycles were anaphylactic reactions, peripheral neuropathy
and regimen modification.
The results from the patients’ evaluation of their
own hair loss yielded a numerically lower VAS score for the 3°C
compared to that for the 8°C temperature. This tendency was most
pronounced in cycle 4 compared to the first 3 cycles. However, the
differences were not statistically significant (Student’s t-test;
ANOVA repeated measures). The evaluation of the images by the
investigators to grade hair loss demonstrated the same numerical
differences in cycles 1–2, although without statistical
significance between the two pre-set temperatures of the coolant
medium. A significant time effect (ANOVA; P=0.035) was observed
from cycle 1 to 4 with decreasing hair loss from cycle 2 (Table VI). The most pronounced hair loss
was recorded after cycle 2, by the patients as well as the
investigators. The inter-rater agreement between the patients’
evaluation of their own hair loss and the investigators’ evaluation
of the images was low (κ-value=0.16, 95% CI: 0.04–0.28). The
patients scored their hair loss significantly higher on the VAS
compared to the investigators (Wilcoxon matched-pairs test;
P=0.033).
| Table VI.Evaluation of hair loss by the visual
analog scale. |
Table VI.
Evaluation of hair loss by the visual
analog scale.
| A, Patients’
evaluationa |
|
| Temperature | Cycle 1 | Cycle 2 | Cycle 3 | Cycle 4 |
|
| 3°C | 3.0 (1.5) | 2.9 (2.1) | 1.8 (1.8) | 2.8 (2.7) |
| 8°C | 3.3 (2.2) | 3.7 (2.9) | 2.4 (2.4) | 1.7 (1.7) |
| P-valueb | 0.678 | 0.389 | 0.457 | 0.615 |
|
| B, Study nurses’
evaluation (photos)a |
|
| Temperature | Cycle 1 | Cycle 2 | Cycle 3 | Cycle 4 |
|
| 3°C | 1.9 (1.2) | 2.1 (1.2) | 1.3 (0.7) | 0.9 (0.7) |
| 8°C | 2.6 (2.1) | 3.1 (1.8) | 1.3 (0.9) | 1.0 (1.4) |
| P-valueb | 0.291 | 0.087 | 0.829 | 0.837 |
In the complete series, 49% of patients subjectively
experienced >50% hair loss and 38% reported the need for a wig.
No significant differences were recorded between patients treated
with 3°C and those treated with 8°C regarding these end-points.
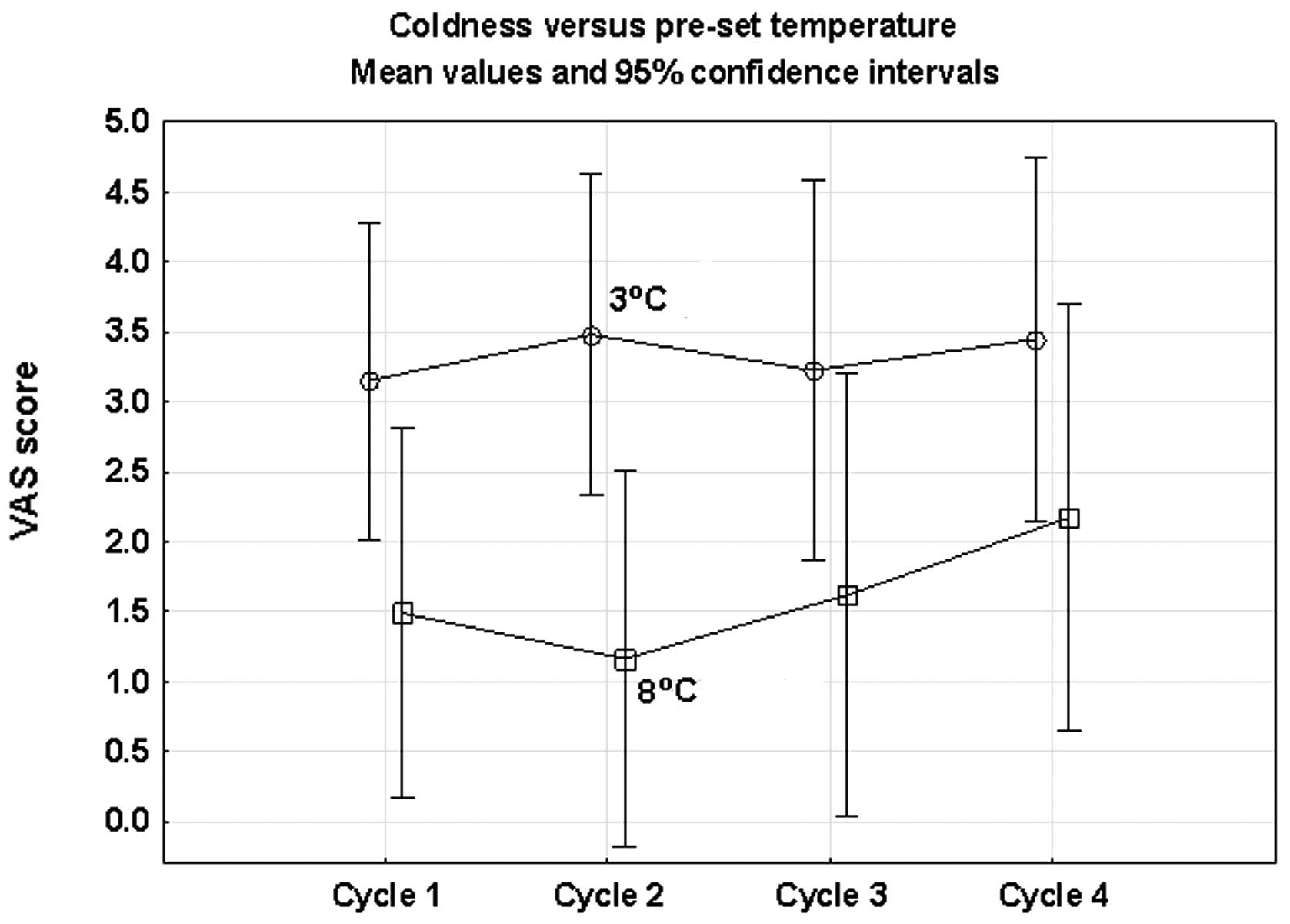
The results indicated an association between the
pre-set temperature and the patients’ experience of headache and
coldness. There was a marginally higher mean score for headache in
the 3°C compared with the 8°C group. Repeated ANOVA measures
revealed a borderline significance (P=0.085). The feeling of
coldness was more common in the 3°C group and this difference was
statistically significant (ANOVA; P= 0.037) (Fig. 3). No significant time effects were
observed in the registered side effects (Table VII).
| Table VII.Evaluation of side effects by the
visual analog scale. |
Table VII.
Evaluation of side effects by the
visual analog scale.
| A,
Headachea,b |
|
| Temperature | Cycle 1 | Cycle 2 | Cycle 3 | Cycle 4 |
|
| 3°C | 0.8 (1.0) | 0.9 (1.4) | 1.0 (2.3) | 0.3 (0.3) |
| 8°C | 0.5 (0.6) | 0.3 (0.3) | 0.4 (0.2) | 0.3 (0.2) |
| P-valued | 0.193 | 0.124 | 0.298 | 0.662 |
|
| B,
Coldnessa,c |
|
| Temperature | Cycle 1 | Cycle 2 | Cycle 3 | Cycle 4 |
|
| 3°C | 2.7 (2.3) | 3.0 (2.5) | 3.0 (2.8) | 3.4 (2.4) |
| 8°C | 1.8 (1.8) | 1.6 (1.5) | 1.9 (1.8) | 2.5 (2.6) |
| P-valued | 0.175 | 0.061 | 0.207 | 0.320 |
Discussion
The findings of the pre-study indicated that a
pre-set temperature of 3°C of the coolant medium was more effective
in achieving a subcutaneous temperature level of <22°C and,
possibly, in preventing alopecia more efficiently. However, the
randomized main study could not verify a significant difference in
the prevention of alopecia between the 3°C and the 8°C groups. The
findings also revealed a difficulty in determining a specific
pre-set temperature suitable for all individuals, which was in
agreement with the findings of other studies (6,11,15).
Furthermore, scalp cooling may not be suitable for all patients
(16) and the incidence of side
effects, such as headache and coldness, may increase with lower
pre-set temperatures.
Although the number of volunteers was limited, the
findings of the pre-study provided useful information regarding the
range of variations in scalp temperature within and among
individuals, at baseline and during the cooling procedure. To the
best of our knowledge, these variations had not been priorly
documented to this extent. The variations may explain why patients
respond with such divergence to scalp cooling in the clinical
setting, despite identical pre-set temperatures. Gregory et
al (11) measured the scalp
temperature in 24 patients using a hypodermic needle and reported
variations in the subcutaneous temperature from 18.5–28.5°C during
cooling; however, since needle placement was not reported in that
study, a comparison with our findings is difficult.
Investigators have previously attempted to elucidate
the reason for the variations in scalp temperature among
individuals. Breed (17) reported
that biochemical and biophysical processes affected the association
between skin temperature and hair loss. Bulow et al
(10) investigated whether the
enhanced heat dissipation originates from structures lying below
the subcutaneous tissue or from thermal reflex differences when it
comes to skin perfusion. Janssen et al (18) underlined the importance of
individual anatomical differences, such as the shape of the head
and the thickness of the insulating fat layer. Those findings
contradicted those previously reported by Gregory et al
(11); those authors suggested
that the variation in scalp temperature among patients may not be
attributed to the density of the scalp tissue or hair thickness.
There is currently no satisfactory explanation for the wide scalp
temperature variation in the same individual at various time
points.
Our clinical experience is that the most extensive
hair loss during chemotherapy with scalp cooling is observed in the
top of the head, which was confirmed by the findings from our
pre-study. The subcutaneous baseline temperature in that region was
∼30°C and appeared to be more unresponsive to scalp cooling. Trueb
(14) also reported that the top
of the head is the most common region where hair loss is observed.
Massey (19) observed that the
temperature in the top of the head at room temperature tended to be
by 1°C higher compared to that in other regions of the scalp. In
the present study, the evaluation of the images captured from the
top of head indicated that this is the region most extensively
affected by alopecia.
To the best of our knowledge, this study was the
first randomized, blinded study on scalp cooling and the comparison
of two pre-set temperatures to determine the most effective
temperature level for the prevention of hair loss. The study group
exclusively included patients receiving the same highly potential
chemotherapeutic agent (paclitaxel) to ensure homogeneity. Our
findings are consistent with those reported by Ridderheim et
al (20), who used the same
technique and observed that hair loss in 30 patients who received
paclitaxel and carboplatin ranged from 0–6.5 (mean 2.5) on the VAS
with a pre-set temperature of 5°C. When summarizing all the cycles
of the present study, we estimated a mean value of 2.4 (range,
0.2–7.8) on the VAS with a pre-set temperature of 3°C and a mean of
3.2 (range, 0.3–9.0) with a pre-set temperature of 8°C, indicating
a temperature dependence of hair loss.
In addition, the main study provided data on the
side effects associated with scalp cooling, such as headache and
coldness, enabling a better understanding of this subject.
Side effects, such as headache and coldness, are
commonly reported in conjunction with scalp cooling (20,21).
The discomfort of scalp cooling was increased when the pre-set
temperature was lowered from 8 to 3°C. Katsimbri et al
(22) reported that headache
appeared to worsen with extended regimens. The patients in our
study had the cold cap on for 5 h, which must be considered as the
maximum tolerated time for patients undergoing chemotherapy. We
also observed a higher incidence of headache and feeling of
coldness compared to previous findings with a pre-set temperature
of 5°C (20).
In previous studies, the outcome of scalp cooling
was measured on a 4-point Dean’s scale (23), or according to the World Health
Organization’s 5 criteria of hair loss (19,24).
Both scales range from no hair loss to 75% or total hair loss. For
the evaluation of the main study, the VAS was selected with 10
score steps, which is the same method as that used by Ridderheim
et al (20). That study
used the same method of scalp cooling and some of the patients
included received the same type of chemotherapy as our patients,
which makes the two studies comparable. There are more flexible
choices in the evaluation of hair loss and side effects when using
the VAS, which was convenient and considered as an advantage.
There are a number of considerations when evaluating
the results of the present and other studies. In the pre-study, we
were unable to confirm with precision that the tip of the probe was
placed at the depth of the hair follicles. Probe displacement may
explain some of the deviations. However, the results are largely in
agreement with the findings of Bulow et al (10), who stated that the temperature
reduction from the subcutaneous to the epicutaneous tissue in the
frontal region of the head is ∼3°C. The association between
subcutaneous and epicutaneous temperatures was not linear
throughout the cooling procedure, with the difference being more
noticeable after 30 min.
In the main study, there were a number of patients
who were unable to complete the 4 cycles, due to circumstances
beyond our control. Moreover, the time of patient inclusion was
more prolonged than anticipated.
The fit of the cooling cap may also affect the study
results. Further studies are required on the design of the cooling
cap and the contact between the cooling channels of the inner cap
and the surface of the scalp, particularly in the region of the
vertex (top of the head).
In conclusion, the results demonstrated that a
pre-set temperature of 3°C of the coolant tended to be more
effective in achieving a subcutaneous temperature of <22°C.
However, there was no statistically significant difference between
the two investigated temperatures regarding the prevention of CIA
in patients receiving paclitaxel and carboplatin. Numerically, the
VAS scores were in favor of the 3°C temperature; however, the
differences between the two groups were not statistically
significant. In addition, the difference between the two levels of
temperature may be due to the rather limited number of patients
included in this study.
Our findings revealed a difficulty in determining an
optimal pre-set temperature for all the individuals. Ideally, a
non-invasive method should measure the temperature of the surface
of the scalp during the cooling session and adapt the pre-set
temperature of the coolant in response to this measurement. In
order to measure scalp temperature there is a need for an
appropriate validated instrument, as previously stated by Hesketh
et al (25). Until a more
reliable method to investigate the advantages and disadvantages of
scalp cooling is designed, we must conclude that a temperature of
3°C may be more effective in preventing alopecia during
paclitaxel/carboplatin treatment, at the cost of a higher incidence
of side effects.
Our findings indicated that further investigations
are required to evaluate and improve the existing scalp cooling
techniques during chemotherapy treatment of cancer patients.
References
|
1.
|
Fitch MI: Psychosocial management of
patients with recurrent ovarian cancer: treating the whole patient
to improve quality of life. Semin Oncol Nurs. 19:40–53. 2003.
View Article : Google Scholar
|
|
2.
|
Rosman S: Cancer and stigma: experience of
patients with chemotherapy-induced alopecia. Patient Educ Couns.
52:333–339. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Sun CC, Bodurka DC, Weaver CB, Rasu R,
Wolf JK, Bevers MW, et al: Rankings and symptom assessments of side
effects from chemotherapy: insights from experienced patients with
ovarian cancer. Support Care Cancer. 13:219–227. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Lemieux J, Maunsell E and Provencher L:
Chemotherapy-induced alopecia and effects on quality of life among
women with breast cancer: a literature review. Psychooncology.
17:317–328. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Girman CJ, Hartmaier S, Roberts J,
Bergfeld W and Waldstreicher J: Patient-perceived importance of
negative effects of androgenetic alopecia in women. J Womens Health
Gend Based Med. 8:1091–1095. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Cook NF: Self-concept and cancer:
understanding the nursing role. Br J Nurs. 8:318–324. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Ekwall E, Ternestedt BM and Sorbe B:
Recurrence of ovarian cancer-living in limbo. Cancer Nurs.
30:270–277. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Trueb RM: Chemotherapy-induced alopecia.
Curr Opin Support Palliat Care. 4:281–284. 2010. View Article : Google Scholar
|
|
9.
|
Tollenaar RA, Liefers GJ, Repelaer van
Driel OJ and van de Velde CJ: Scalp cooling has no place in the
prevention of alopecia in adjuvant chemotherapy for breast cancer.
Eur J Cancer. 30A:1448–1453. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Bulow J, Friberg L, Gaardsting O and
Hansen M: Frontal subcutaneous blood flow, and epi- and
subcutaneous temperatures during scalp cooling in normal man. Scand
J Clin Lab Invest. 45:505–508. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Gregory RP, Cooke T, Middleton J, Buchanan
RB and Williams CJ: Prevention of doxorubicin-induced alopecia by
scalp hypothermia: relation to degree of cooling. Br Med J (Clin
Res Ed). 284:1674:1982
|
|
12.
|
Cooke T, Gregory RP, Middleton J and
Williams C: Prevention of doxorubicin-induced alopecia. Br Med J
(Clin Res Ed). 282:734–735. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Grevelman EG and Breed WP: Prevention of
chemo-therapy-induced hair loss by scalp cooling. Ann Oncol.
16:352–358. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Trueb RM: Chemotherapy-induced alopecia.
Semin Cutan Med Surg. 28:11–14. 2009. View Article : Google Scholar
|
|
15.
|
Janssen FP, Rajan V, Steenbergen W, van
Leeuwen GM and van Steenhoven AA: The relationship between local
scalp skin temperature and cutaneous perfusion during scalp
cooling. Physiol Meas. 28:829–839. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Dougherty L: Comparing methods to prevent
chemotherapy-induced alopecia. Cancer Nurs Pract. 5:25–31. 2006.
View Article : Google Scholar
|
|
17.
|
Breed WP: What is wrong with the
30-year-old practice of scalp cooling for the prevention of
chemotherapy-induced hair loss? Support Care Cancer. 12:3–5.
2004.PubMed/NCBI
|
|
18.
|
Janssen FE, Van Leeuwen GM and Van
Steenhoven AA: Modelling of temperature and perfusion during scalp
cooling. Phys Med Biol. 50:4065–4073. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Massey CS: A multicentre study to
determine the efficacy and patient acceptability of the Paxman
Scalp Cooler to prevent hair loss in patients receiving
chemotherapy. Eur J Oncol Nurs. 8:121–130. 2004. View Article : Google Scholar
|
|
20.
|
Ridderheim M, Bjurberg M and Gustavsson A:
Scalp hypothermia to prevent chemotherapy-induced alopecia is
effective and safe: a pilot study of a new digitized scalp-cooling
system used in 74 patients. Support Care Cancer. 11:371–377.
2003.
|
|
21.
|
Protiere C, Evans K, Camerlo J, d’Ingrado
MP, Macquart-Moulin G, Viens P, et al: Efficacy and tolerance of a
scalp-cooling system for prevention of hair loss and the experience
of breast cancer patients treated by adjuvant chemotherapy. Support
Care Cancer. 10:529–537. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Katsimbri P, Bamias A and Pavlidis N:
Prevention of chemotherapy-induced alopecia using an effective
scalp cooling system. Eur J Cancer. 36:766–771. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Christodoulou C, Klouvas G, Efstathiou E,
Zervakis D, Papazachariou E, Plyta M and Skarlos DV: Effectiveness
of the MSC cold cap system in the prevention of
chemotherapy-induced alopecia. Oncology. 62:97–102. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
van den Hurk CJ, Peerbooms M, van de
Poll-Franse LV, Nortier JW, Coebergh JW and Breed WP: Scalp cooling
for hair preservation and associated characteristics in 1411
chemotherapy patients - results of the Dutch Scalp Cooling
Registry. Acta Oncol. 51:497–504. 2012.PubMed/NCBI
|
|
25.
|
Hesketh PJ, Batchelor D, Golant M, Lyman
GH, Rhodes N and Yardley D: Chemotherapy-induced alopecia:
psychosocial impact and therapeutic approaches. Support Care
Cancer. 12:543–549. 2004.PubMed/NCBI
|