Introduction
Clinically, mediastinal masses are currently a
common occur-rence. The incidence of certain diseases, such as lung
cancer and sarcoidosis, is on the increase. Accurate and early
diagnosis of such diseases is crucial for the appropriate treatment
and prognosis (1,2). A major concern for clinicians
worldwide is the establishment of a diagnostic method that is fast,
accurate and minimally invasive.
Imaging is crucial in the diagnosis of mediastinal
masses. An imaging scan may provide critical information with
regard to the location, size and periphery of the lesions and it is
fast and non-invasive. Positron emission tomography-computed
tomography (PET-CT) may also indicate whether the mass is benign or
malignant. However, more precise information is required for
staging and typing.
Although mediastinoscopy or surgery is considered to
be the gold standard for diagnosis (3), some patients are unable to tolerate
the procedural injury and intravenous anesthesia. Therefore,
efforts are focused on establishing a method that is easy to use,
minimally invasive and efficient in providing the critical
information required.
Transbronchial biopsy is such a method, particularly
trans-bronchial needle aspiration (TBNA), which aspirates masses
and pathological lymph nodes through an air tube, with minimal
invasion (4). However,
conventional TBNA requires the assistance of X-ray, CT or PET-CT;
therefore, there remains the need for equipment that may guide
real-time sampling. The development of the ultrasound technique
enabled clinicians to perform esophageal endoscopic
ultrasound-guided fine-needle aspiration (EUS-FNA) in the 1980s.
Although this technique was efficient in real-time aspiration of
para-esophageal masses, its range was limited for mediastinal
masses (5) and the technique was
developed further over the subsequent decades. When endobronchial
ultrasound-guided (EBUS)-TBNA was introduced, it enabled sampling
within a broader range (6,7). Furthermore, there is continuous
improvement, such as ventilation (8) and linear probes (9), which rendered this procedure easier,
faster and more accurate. Therefore, EBUS-TBNA may be the optimal
method. However, the equipment is costly and may be unaffordable
for some hospitals. Furthermore, certain clinicians consider
conventional TBNA sufficient for diagnosis, provided it is
performed by a skilled expert. Over the last few years,
particularly from 2000 onwards, several studies have focused on
this issue. Certain studies indicated that EBUS-TBNA performs
better in terms of diagnostic sensitivity and specificity, as well
as safety (10,11). However, other studies suggested
that conventional TBNA was not inferior to EBUS-TBNA (12,13).
Although there have been several studies comparing these two
methods, they all presented with drawbacks, particularly their
small sample size. Therefore, we conducted this meta-analysis using
the existing resources to compare the diagnostic yield of the two
methods.
Materials and methods
Search strategy
A comprehensive literature search was conducted in
order to identify studies comparing the diagnostic performance of
EBUS-TBNA to that of TBNA in the detection of mediastinal masses.
The eligible studies were required to use histopathological and/or
cytological analysis, or close clinical follow-up for ≥6 months
after mediastinoscopy or surgery, as the reference standard.
Studies that investigated EBUS-TBNA or conventional TBNA alone,
studies that did not provide results on (or sufficient data to
calculate) diagnostic yield and studies that assessed diagnostic
yield only in metastatic mediastinal lymph nodes, were
excluded.
A search was conducted through the electronic
databases PubMed (from 1966 to April, 2011), Embase (from 1980 to
April, 2011) and the Cochrane Library. The search terms included
‘endobronchial ultrasound’, ‘endoscopic ultrasound’ or
‘endosonography’, ‘transbronchial ultrasound’ and ‘trans-bronchial
needle aspiration’. We also reviewed the reference lists of
original and review articles to identify relevant studies. There
were no restrictions regarding publication language.
Study selection and data collection
Two reviewers (Z.T.Y. and Z.X.J.) independently
assessed the eligibility of the identified studies and
discrepancies were resolved by consensus. Data was collected using
standardized data collection forms. The following information was
extracted from each eligible study: first author’s name, year of
publication, description of study population, study design
(prospective, retrospective or unknown), patient enrollment
(consecutive or not), interpretation of test results (blinded or
not), patient selection on the basis of CT- or PET-positive results
or not, reference standard and diagnostic yield results.
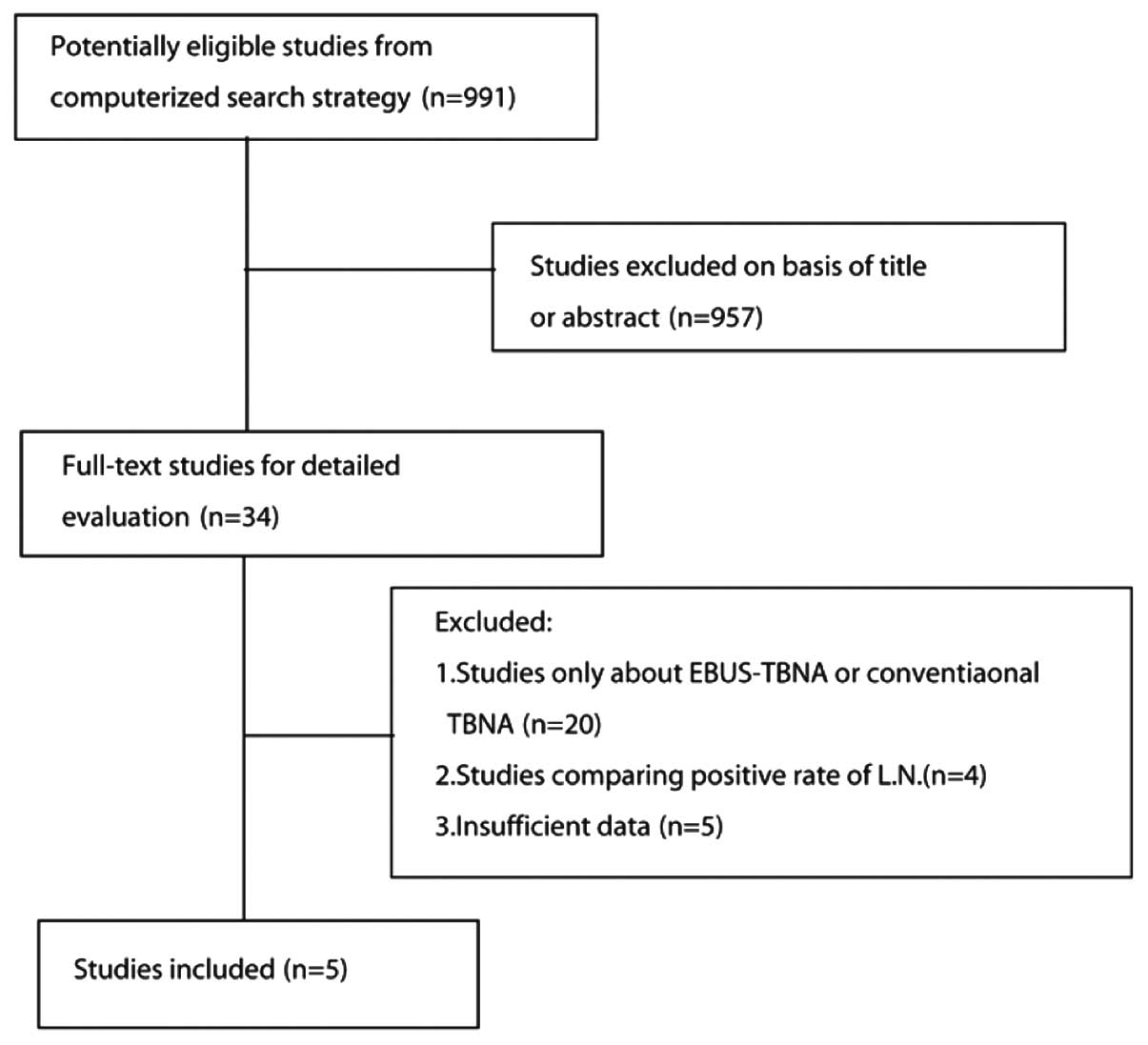
A total of 991 citations were initially identified.
After reviewing the titles and abstracts, 957 citations, such as
case reports, reviews, reader letters and studies not assessing
both methods, were excluded. After reading the full text, 5 studies
were selected for inclusion in the planned meta-analysis (Fig. 1 and Table I) (12–16).
 | Table I.Characteristics of the trials included
in the meta-analysis. |
Table I.
Characteristics of the trials included
in the meta-analysis.
| Authors (refs.) | Study time | Sample size | Mean age | Study design | ROSE | Conventional TBNA
(%) | EBUS-TBNA (%) |
|---|
| Arslan et al
(12) | 2006.7–2007.10 | 60 | 56.15 | Prospective,
randomized | No | 10/30 (33.3) | 20/30 (66.7) |
| Tremblay et al
(13) | 2006.9–2007.08 | 50 | 40.2 | Randomized,
blinded | No | 14/26 (53.8) | 20/24 (83.3) |
| Herth et al
(14) | 2001.6–2002.3 | 200 | 51.9 | Randomized | No | 66/100 (66) | 85/100 (85) |
| Oki et al
(15) | - | 15 | 55.2 | Prospective | No | 13/15 (93) | 13/15 (93) |
| Shannon et al
(16) | 1993.1–1994.11 | 82 | 60 | Prospective,
randomized | Yes | 32/42 (76.2) | 33/40 (82.5) |
Statistical analysis
To calculate the pooled odds ratio (OR), the number
of true positives in each arm was extracted from each study and
combined using the method described by Mantel and Haenszel
(17). A pooled OR>1 indicated
a diagnostic yield in the EBUS-TBNA arm. Heterogeneity between the
trials was evaluated by the χ2 test and I2
statistic (18). These indices
were used to assess the percentage of variability across studies
attributable to heterogeneity rather than chance. Statistical
heterogeneity was considered significant when P<0.10 for the
χ2 test or I2>50%. When there was no
statistically significant heterogeneity, a pooled effect was
calculated with a fixed-effects model; otherwise, a random-effects
model was employed. We also assessed the probability of publication
bias according to the Egger’s (19) and Begg-Mazumdar (20) tests. All reported P-values were
two-sided and P<0.05 was considered to indicate a statistically
significant difference. Statistical analyses were performed using
RevMan software, version 5.0 (The Cochrane Collaboration).
Results
Study selection
The literature search yielded 991 studies, of which
957 were excluded after reviewing the title and abstract. The
remaining 34 potentially eligible studies underwent a full-text
review. However, 20 studies only focused on EBUS-TBNA or
conventional TBNA, 4 studies compared the positive lymph node rates
and 5 studies did not provide sufficient data. Ultimately, 5
studies (12–16), including a total of 407 patients,
fulfilled all the inclusion criteria and were selected for the
meta-analysis.
Characteristics of individual
studies
Arslan et al (12) conducted a prospective study,
enrolling 60 patients who were blindly randomized. The overall
diagnostic yield was 66.7% (20/30) in the EBUS-TBNA and 33.33%
(10/30) in the conventional TBNA group. The difference between the
groups was statistically significant, particularly during the early
stages of the disease. In the study conducted by Tremblay et
al (13), EBUS-TBNA and TBNA
were compared in 50 patients, randomly and blindly. EBUS-TBNA
accurately diagnosed 20 (83.30%) of the 24 patients and
conventional TBNA diagnosed 14 (53.80%) of the 26 patients.
Furthermore, EBUS exhibited a higher aspiration efficiency (4–2.2
on average). Herth et al (14) conducted a large-scale study,
including 200 randomized patients. The diagnostic outcome was 85%
(EBUS-TBNA) vs. 66% (conventional TBNA). The patients in that study
were also stratified by the location of the lymph nodes and the
authors concluded that, when the lesion was in the subcarinal
region, there was no difference between EBUS-TBNA and conventional
TBNA; however, when the lesion was located elsewhere, the
difference was statistically significant. The 3 previously
mentioned studies consistently confirmed that the diagnostic yield
of EBUS-TBNA was higher compared with that of conventional TBNA;
however, certain researchers were not convinced. In a study
conducted by Oki et al (15), 15 patients were evaluated by
EBUS-TBNA and conventional TBNA and the diagnostic yield was
identical (93% in both methods). Furthermore, a study conducted by
Shannon et al (16)
enrolled 82 patients. Rapid on-site evaluation (ROSE) by
cytopathological examination was applied and the results suggested
that there was no significant difference, with or without the use
of ultrasound (Table I).
Patients, diagnostic methods and effect
on diagnostic yield
All studies used an ultrasound bronchoscope provided
by Olympus (Tokyo, Japan). The median number of participants was
77.5 (range, 15–200) and the median age was 53.5 years (range,
40–60 years). The diagnosis was based on histopathological and/or
cytological analysis in all 5 studies. When the final diagnosis was
not definitive, other diagnostic methods, such as clinical
follow-up for ≥6 months, mediastinoscopy or surgery were used.
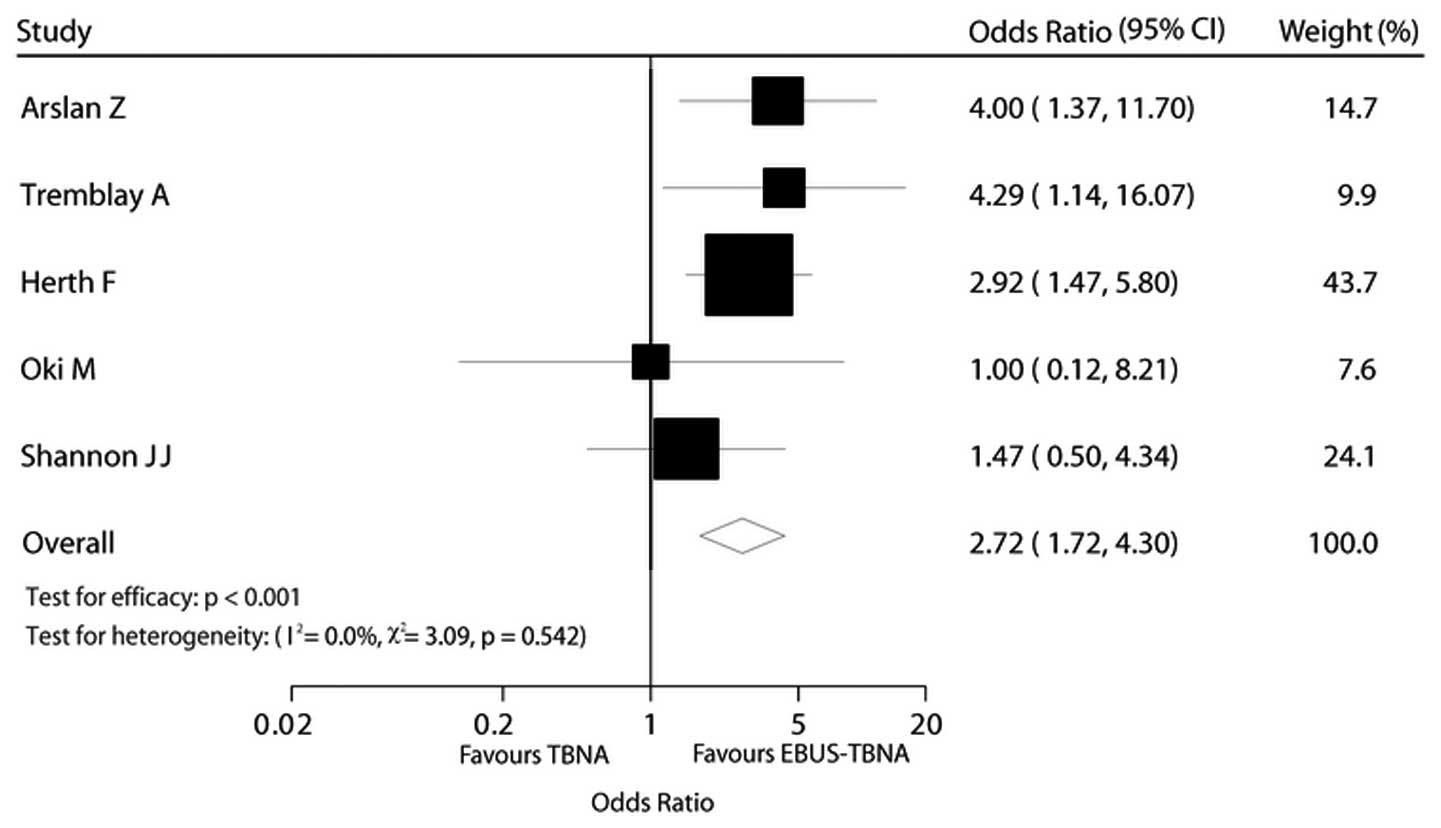
The effect of the diagnostic method on diagnostic
yield was estimated directly for all 5 trials. The EBUS-TBNA arm
was associated with a significantly higher OR compared to that of
the TBNA arm in terms of diagnostic yield [OR=2.72, 95% confidence
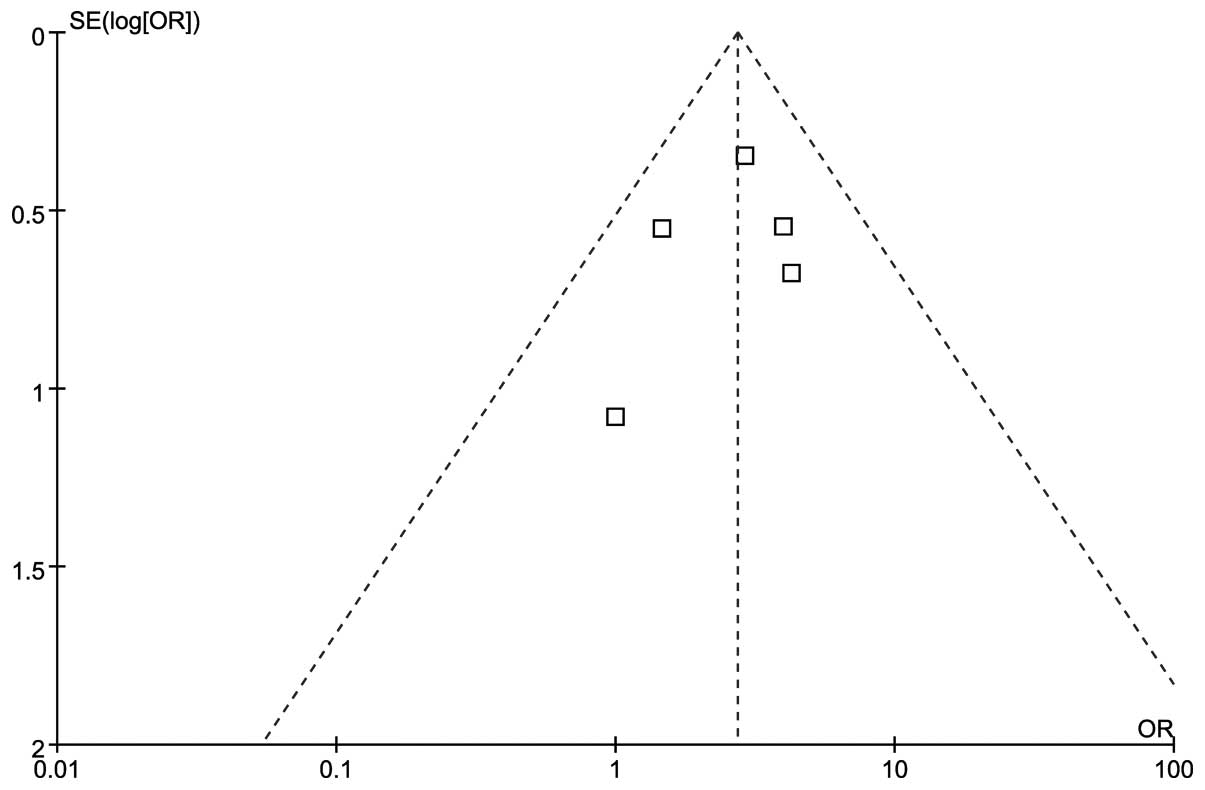
interval (CI): 1.72–4.30, P<0.001; Fig. 2]. There was no evidence of
heterogeneity among individual trials (I2=0%, P=0.540).
We detected no evidence of publication bias using the Egger’s
(P=0.568) and the Begg-Mazumdar (P=0.806) tests (Fig. 2).
Discussion
Accurate staging enables the selection of the
appropriate treatment, which may achieve higher survival rates and
improve the quality of life of the patients. In our clinical
practice, the diagnostic methods may be classified into invasive
and non-invasive. Although mediastinal lymph nodes and masses may
be apparent on CT or PET-CT, accurate diagnosis requires a tissue
biopsy. The treatment options depend largely on histology and
staging. Therefore, the invasive techniques are necessary. In order
to determine the pathological type, tissue may be obtained under
X-ray or CT guidance. Fiber-optic bronchoscopy or mediastinoscopy
may be used. If a diagnosis cannot be confirmed with these methods,
surgery may be the final option. Among these invasive methods, we
always to select the least invasive procedure with the highest
level of diagnostic sensitivity.
In a meta-analysis conducted by Holty et al
(21), TBNA exhibited a relatively
higher specificity (99%), although the sensitivity was low (39%),
with a pooled major complication rate of 0.3%. A meta-analysis by
Micames et al (22)
reported that EUS-FNA identified 83% of the patients (95% CI:
0.78–0.87) with positive and 97% of the patients (95% CI:
0.96–0.98) with negative mediastinal lymph nodes. In a
meta-analysis by Gu et al (1), the primary endpoint was the accuracy
of EBUS-TBNA in detecting lymph node metastases in lung cancer. The
results demonstrated that EBUS-TBNA exhibited the highest
sensitivity (93%, 95% CI: 0.91–0.94) and specificity (100%, 95% CI:
0.99–1.000) (Figs. 2 and 3).
To the best of our knowledge, this meta-analysis was
the first to compare the diagnostic yield between EBUS-TBNA and
conventional TBNA. Our results demonstrated that EBUS-TBNA
performed better compared with conventional TBNA and were
consistent with those of well-designed previous studies (13,15).
Shannon et al (16)
reported that the ROSE method they used improved the diagnostic
accuracy, which was consistent with the results of Chin et
al (23); however, it requires
costly and sophisticated equipment. In the studies of Herth et
al (14) and Arslan et
al (12), the patients were
stratified according to the anatomic location of the pathological
lymph nodes. The authors reported that EBUS-TBNA performed better
in sites other than the subcarinal space. When the lesion was
peripherally located, although EBUS-TBNA sampled more accurately
and easily, the diagnostic yield was low and was improved via
combination with other equipment (24,25).
Those findings suggest that when EBUS-TBNA is used for diagnostic
purposes, the site of the lesion should be carefully considered. In
our meta-analysis, no complication (such as, vessel injury) was
recorded among the 407 patients. Rong et al (26)mentioned in his study that there were
more complications in the conventional TBNA group, although the
difference between EBUS-TBNA and TBNA was not statistically
significant. According to our experience, if clinicians are
familiarized with the anatomy, have mastered the technique and
properly evaluate the patient’s condition prior to the procedure,
the majority of complications may be avoided.
There were certain limitations to our analysis,
although our findings demonstrated that EBUS-TBNA performed better
compared to conventional TBNA. The design and sample size of the
enrolled studies did not meet our expectations. Other factors, such
as the experience of the operators (27), the time of the aspiration and the
location, size and nature of the lesions, may affect the final
result. When these factors are well-controlled, the comparison may
be of greater value.
In conclusion, EBUS-TBNA and conventional TBNA are
safe and provide good diagnostic yield in the diagnosis of hilar
and mediastinal masses and lymphadenopathies. However, EBUS-TBNA
performs better compared with conventional TBNA, with shorter
aspiration time and higher sensitivity. The result may be further
improved via combination with ROSE. However, further randomized,
multicenter clinical trials including larger sample sizes are
required to further establish the advanatages of EBUS-TBNA over
conventional TBNA in the diagnosis of mediastinal masses.
Acknowledgements
This study was supported by grants
from the National Natural Science Foundation of China (nos.
30871133 and 81270073).
References
|
1.
|
Gu P, Zhao YZ, Jiang LY, Zhang W, Xin Y
and Han BH: Endobronchial ultrasound-guided transbronchial needle
aspiration for staging of lung cancer: a systematic review and
meta-analysis. Eur J Cancer. 45:1389–1396. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Varela-Lema L, Fernandez-Villar A and
Ruano-Ravina A: Effectiveness and safety of endobronchial
ultrasound-trans-bronchial needle aspiration: a systematic review.
Eur Respir J. 33:1156–1164. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Rusch VW: Mediastinoscopy: an endangered
species? J Clin Oncol. 23:8283–8285. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Arroliga AC and Matthay RA: The role of
bronchoscopy in lung cancer. Clin Chest Med. 14:87–98.
1993.PubMed/NCBI
|
|
5.
|
Annema JT, Versteegh MI, Veselic M, Voigt
P and Rabe KF: Endoscopic ultrasound-guided fine-needle aspiration
in the diagnosis and staging of lung cancer and its impact on
surgical staging. J Clin Oncol. 23:8357–8361. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Silvestri GA, Hoffman BJ, Bhutani MS, et
al: Endoscopic ultrasound with fine-needle aspiration in the
diagnosis and staging of lung cancer. Ann Thorac Surg.
61:1441–1446. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Hurter T and Hanrath P: Endobronchial
sonography: feasibility and preliminary results. Thorax.
47:565–567. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Becker HD: EBUS: a new dimension in
bronchoscopy. Of sounds and images - a paradigm of innovation.
Respiration. 73:583–586. 2006.PubMed/NCBI
|
|
9.
|
Herth FJ and Eberhardt R: Actual role of
endobronchial ultrasound (EBUS). Eur Radiol. 17:1806–1812. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Cetinkaya E, Gunluoglu G, Ozgul A, et al:
Value of real-time endobronchial ultrasound-guided transbronchial
needle aspiration. Ann Thorac Med. 6:77–81. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Ost DE, Ernst A, Lei X, et al: AQuIRE
Bronchoscopy Registry: Diagnostic yield of endobronchial
ultrasound-guided trans-bronchial needle aspiration: results of the
AQuIRE Bronchoscopy Registry. Chest. 140:1557–1566. 2011.
View Article : Google Scholar
|
|
12.
|
Arslan Z, Ilgazli A, Bakir M, Yildiz K and
Topçu S: Conventional vs. endobronchial ultrasound-guided
transbronchial needle aspiration in the diagnosis of mediastinal
lymphadenopathies. Tuberk Toraks. 59:153–157. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Tremblay A, Stather DR, Maceachern P,
Khalil M and Field SK: A randomized controlled trial of standard vs
endobronchial ultrasonography-guided transbronchial needle
aspiration in patients with suspected sarcoidosis. Chest.
136:340–346. 2009. View Article : Google Scholar
|
|
14.
|
Herth F, Becker HD and Ernst A:
Conventional vs. endobronchial ultrasound-guided transbronchial
needle aspiration: a randomized trial. Chest. 125:322–325. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Oki M, Saka H, Kitagawa C, Tanaka S,
Shimokata T, Kawata Y, Mori K, Kajikawa S, Ichihara S and Moritani
S: Real-time endobronchial ultrasound-guided transbronchial needle
aspiration is useful for diagnosing sarcoidosis. Respirology.
12:863–868. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Shannon JJ, Bude RO, Orens JB, et al:
Endobronchial ultrasound-guided needle aspiration of mediastinal
adenopathy. Am J Respir Crit Care Med. 153:1424–1430. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Deeks JJ, Higgins JPT and Altman DG:
Analysing data and undertaking meta-analyses. Cochrane Handbook for
Systematic Reviews of Interventions. Higgins JPT and Green S:
Version 5.0.0 (updated February 2008). Available from url:
http://www.mrc-bsu.cam.ac.uk/cochrane/handbook500/.
Accessed July 15, 2011.
|
|
18.
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Egger M, Davey Smith G, Schneider M and
Minder C: Bias in meta-analysis detected by a simple, graphical
test. BMJ. 315:629–634. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Begg CB and Mazumdar M: Operating
characteristics of a rank correlation test for publication bias.
Biometrics. 50:1088–1101. 1994. View
Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Holty JE, Kuschner WG and Gould MK:
Accuracy of trans-bronchial needle aspiration for mediastinal
staging of non-small cell lung cancer: a meta-analysis. Thorax.
60:949–955. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Micames CG, McCrory DC, Pavey DA, Jowell
PS and Gress FG: Endoscopic ultrasound-guided fine-needle
aspiration for non-small cell lung cancer staging: A systematic
review and metaanalysis. Chest. 131:539–548. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Chin R Jr, McCain TW, Lucia MA, et al:
Transbronchial needle aspiration in diagnosing and staging lung
cancer: how many aspirates are needed? Am J Respir Crit Care Med.
166:377–381. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Sheski FD and Mathur PN: Endobronchial
ultrasound. Chest. 133:264–270. 2008. View Article : Google Scholar
|
|
25.
|
Vilmann P and Puri R: The complete
‘medical’ mediastinoscopy (EUS-FNA + EBUS-TBNA). Minerva Med.
98:331–338. 2007.
|
|
26.
|
Rong F, Xiao SH, Liu J, Li YX, Mai HY and
Lu YS: A comparative research on the conventional transbronchial
needle aspiration and endobronchial ultrasound-guided
transbronchial needle aspiration for the diagnosis of mediastinum
lesions. Zhonghua Jie He He Hu Xi Za Zhi. 34:120–122. 2011.
|
|
27.
|
Gasparini S, Zuccatosta L and De Nictolis
M: Transbronchial needle aspiration of mediastinal lesions. Monaldi
Arch Chest Dis. 55:29–32. 2000.PubMed/NCBI
|