Introduction
Papillary renal carcinoma (papillary RCC) is a
histological subtype of the renal carcinoma. There are two
morphological subtypes of papillary RCC that are correlated with
their prognosis. Type 1 tumor consists of papillae enclosed with a
single layer of small cells with scanty cytoplasm and low-grade
nuclei. In type 2 tumor, the cells covering the papillae are
pseudostratified, generally have eosinophilic cytoplasm and are
usually of higher nuclear grade compared to the cells of type 1
tumors. Papillary RCC is usually associated with a more favorable
prognosis compared to the carcinoma of renal clear cells, while
type 2 tumors carry a worse prognosis compared to type 1 tumors. At
the cytogenetic level, the most common karyotypic changes in
papillary RCC are trisomy of chromosomes 7 and 17, as well as loss
of chromosome Y in males (1–3).
Microscopically, papillary RCCs were predominantly papillary or
tubulopapillary, often with foam cells, necrosis, hemorrhage and
multifocality (4). This case
report described an incidental finding of a necrotic cavity within
a papillary RCC. The imaging data documented the dynamic progress
of the cavitation within the cystic mass. This study was approved
by the Institutional Review Board of the No. 2 People’s Hospital of
Changshu. Informed consent was obtained from the patient.
Case report
A 66-year-old male patient underwent a second
abdominal computed tomography (CT) scan while being monitored for a
renal cyst at the upper pole of the left kidney that was
inadvertently detected 22 months earlier in another hospital. The
patient’s medical history showed surgery had been performed for
gastric adenocarcinoma in January, 2010 at the same institution.
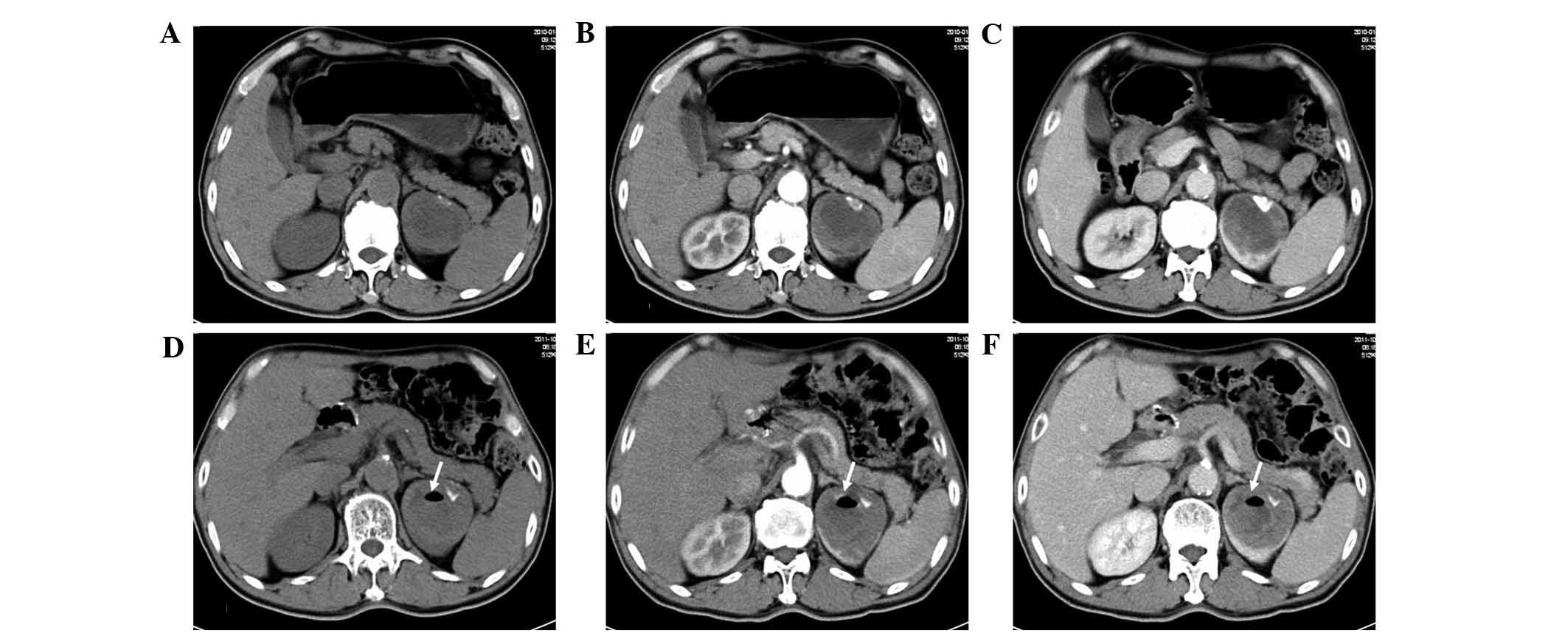
Pre-operative abdominal CT in 2010 detected an unexpected complex
renal cyst at the upper pole of the left kidney (Fig. 1A–C), but no relevant treatment was
administered. Following admission, the patient underwent a contrast
material-enhanced CT and magnetic resonance imaging (MRI)
examination to evaluate the origin of the mass, its correlation
with surrounding structures and possible evidence of metastatic
involvement. CT scans demonstrated a 5.7×5.4 cm well-circumscribed,
exophytic mass arising from the upper pole of the left kidney. A
distinct lesion of 1.8 cm at its greatest diameter within the
exophytic mass was also detected, with a CT value between −600 to
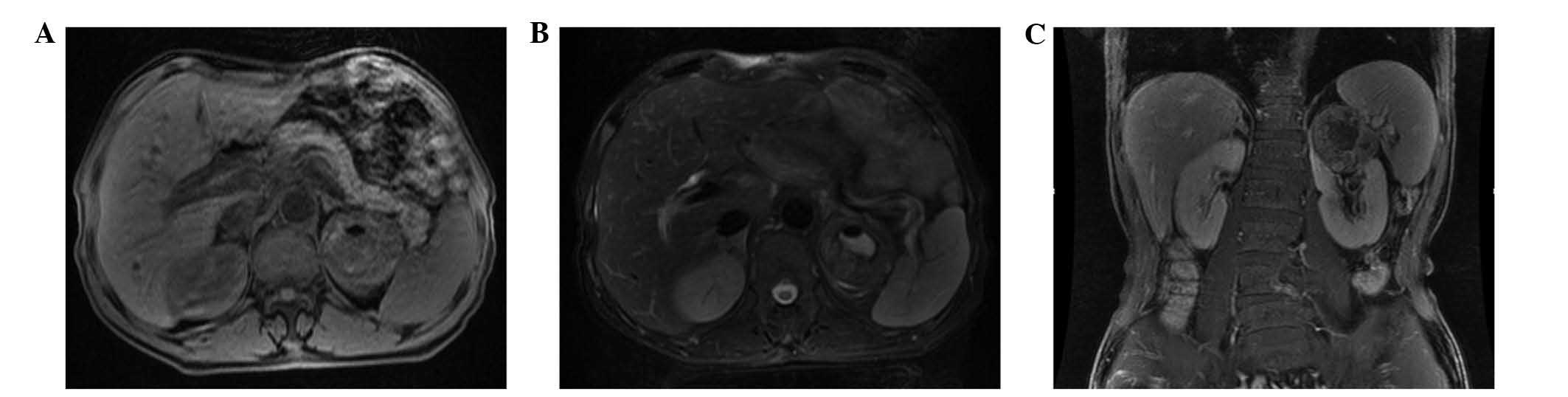
−970 HU (Fig. 1D–F). MRI results
showed that the mass exhibited a pseudocapsule and had low signal
intensity on T1- and T2-weighted images (Fig. 2). This cystic renal lesion was
confirmed as category III on the basis of the Bosniak
classification scheme. The patient analysis did not show any
abnormalities. Concerning current diagnostic criteria, probable
diagnosis for such a heterogeneous cystic mass was limited to a
hemorrhagic renal cyst or cell carcinoma.
Since renal carcinoma involves a potential risk of
metastasis, radical nephrectomy was scheduled for removal of the
left kidney. After general anesthesia was induced, the patient was
placed in the lateral recumbent position and laparoscopic left
radical nephrectomy was successfully performed in October, 2011.
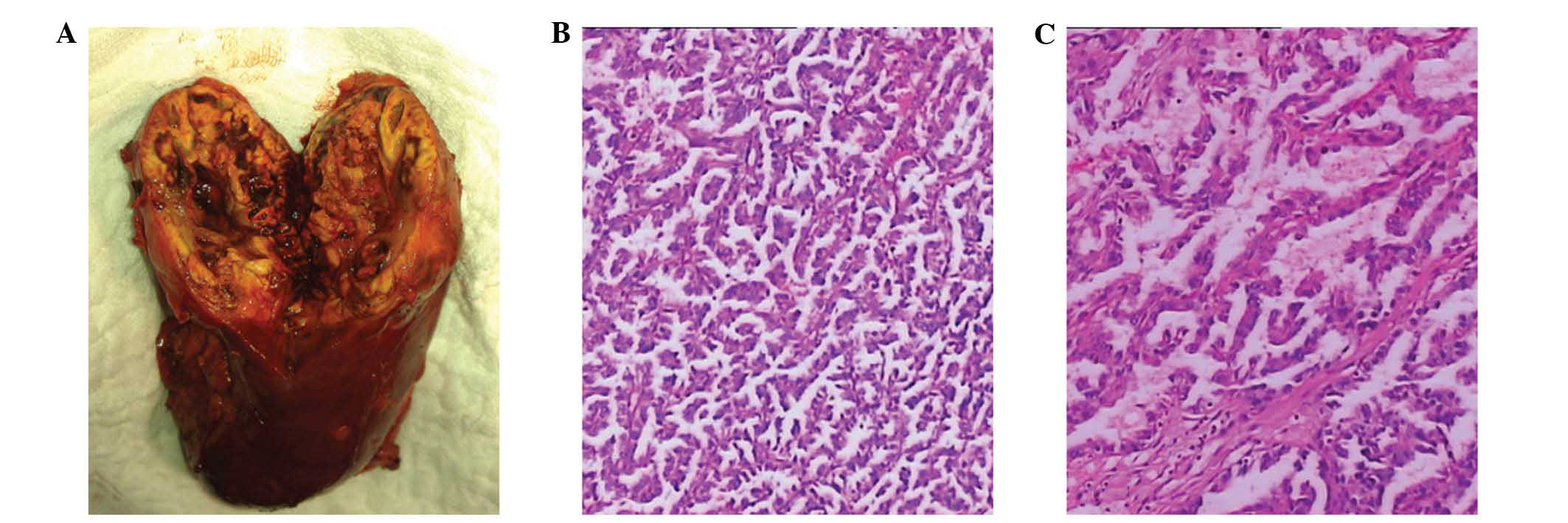
Gross examination was characterized by an irregular-shaped lesion
of mahogany-brown color in the upper pole of the left kidney, with
a maximum diameter of 5.7 cm. The central area in the exophytic
lesion was identified as a 1.8-cm circumscribed cavity, with no
liquid inside but with viscous, chocolate-brown, necrotic and
hemorrhagic material on the cavity wall. The harvested specimen was
processed according to standard surgical pathology protocols.
Microscopic examination results (Fig.
3) showed that the specimen exhibited an outer cystic mass in
the papillary architecture with pleomorphic cells showing prominent
nucleoli and abundant eosinophilic cytoplasm. Papillary
interstitial structure comprises cells arranged on a delicate
fibrovascular core. Infiltration of foamy macrophages into the
papillary structures and extensive tumor necrosis with abundant
hemosiderin granules were detected. Immunohistochemical analyses
showed the tumor cells to be strongly positive for vimentin,
epithelial membrane antigen (EMA) and cytokeratins 7, focally
positive for CD10 and negative for Malan A. Overall, the cyst
characteristics are those of a type 2 papillary RCC of Fuhrman
nuclear grade 3. There was no tumor involvement of the renal
capsule or perinephric fat, no vascular space invasion was
identified and the margins of resection were free of tumor. The
patient was discharged after an uneventful post-operative course.
Follow-up control 6 months later showed normal values in the urine
analysis and renal function.
Discussion
Papillary RCC is the second most frequent carcinoma
of the proximal renal tubules (10–15% of the cases) (5,6). The
clinical and histological details were first described by
Mancilla-Jiménez et al (7)
in 1976. Commonly, it is diagnosed histologically and based on its
characteristic enhanced pattern on CT and MRI. Certain
characteristics of a cystic renal mass including the character of
the lesion wall, septation, calcification, nodularity, CT
attenuation values and enhancement are suggestive of a particular
diagnosis. However, there is a continuum of radiologic findings
often rendering the confident labeling of a cystic renal lesion
benign or malignant difficult.
The papillary RCC in the present case was initially
characterized by a single cyst with an internal cavity and a
calcification filling as part of the cyst. The 1.8-cm diameter
distinct cavity was measured using a CT value between −600 and −970
HU, potentially appreciated as air density. To the best of our
knowledge, the presence of a necrotic cavity within a papillary RCC
has rarely been described. This finding may be considered of
interest with respect to the aetiology of the cavity within the
tumor mass. We first hypothesized that the intracystic vacuum
phenomenon is simply a result of the migration of a
gastrointestinal gaseous collection through disrupted renal
parenchyma or a renal cyst with inflammatory changes. However, the
patient did not experience any fever or abdominal discomfort during
the past 22 months. Additionally, the intact renal capsule of the
renal specimen and evidence of non-infection of perinephric capsule
thickening allows us to exclude the aetiology of gas deposits or
inflammatory changes. At histological analysis, infiltration of
foamy macrophages into the papillary structures and extensive
necrotic tissue with abundant hemosiderin granules suggest a
predisposition for degenerative cyst formation.
Extensive necrosis and bleeding within a tumor is
often thought to reflect poor tumor vascularization, a
characteristic well recognized in angiographic studies of papillary
RCC. The comparison between the CT scan in January, 2010 and 22
months later documented the marked progress of the necrotic
cavitation of the papillary RCC mass.
Acknowledgements
The authors thank Dr Kai Ye for his
valuable technical assistance during the immunohistochemical
analysis.
References
|
1
|
Reuter VE: The pathology of renal
epithelial neoplasms. Semin Oncol. 33:534–543. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Presti JC Jr, Rao PH, Chen Q, Reuter VE,
Li FP, Fair WR and Jhanwar SC: Histopathological, cytogenetic, and
molecular characterization of renal cortical tumors. Cancer Res.
51:1544–1552. 1991.PubMed/NCBI
|
|
3
|
Kovacs G, Wilkens L, Papp T and de Riese
W: Differentiation between papillary and nonpapillary renal cell
carcinomas by DNA analysis. J Natl Cancer Inst. 81:527–530. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yamada T, Endo M, Tsuboi M, Matsuhashi T,
Takase K, Higano S and Takahashi S: Differentiation of pathologic
subtypes of papillary renal cell carcinoma on CT. AJR Am J
Roentgenol. 191:1559–1563. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wein AJ, Kavoussi LR, Novick AC, Partin AW
and Peters CA: Campbell-Walsh Urology. 10th edition. WB Saunders
Company; Philadelphia PA: pp. 1432–1434. 2012
|
|
6
|
Störkel S, Eble JN, Adlakha K, Amin M,
Blute ML, Bostwick DG, Darson M, Delahunt B and Iczkowski K:
Classification of renal cell carcinoma: Workgroup No.1. Union
Internationale Contre le Cancer (UICC) and the American Joint
Committee on Cancer (AJCC). Cancer. 80:987–989. 1997.
|
|
7
|
Mancilla-Jiménez R, Stanley RJ and Blath
RA: Papillary renal cell carcinoma: a clinical, radiologic, and
pathologic study of 34 cases. Cancer. 38:2469–2480. 1976.PubMed/NCBI
|