Introduction
Elastofibroma dorsi (ED) is a rare tumor that
develops in the space between the lower angle of the scapula and
the posterior thoracic wall. Microscopically, the tumor consists of
proliferated fibroblasts and accumulated abnormal elastic fibers.
The pathogenesis of this tumor has not been fully elucidated,
although mechanical friction between the chest wall and the
inferior tip of the scapula may be involved in the development of
ED. Giebel et al (1)
hypothesized, based on the discovery of pre-elastofibroma-like
changes in 81% of their autopsy series, that ED may be part of the
aging process. The high incidence of bilateral lesions (33–100%)
(2,3) also indicates the reactive nature of
this type of tumor. In a large study of 170 ED cases, Nagamine
et al (2) reported that 32%
of the cases occurred within a single family, suggesting a familial
predisposition for ED. Although the etiology of ED remains unclear,
mechanical and genetic factors have been implicated in its
development.
As ED is a benign, slow-growing tumor, it may be
observed without treatment following diagnosis based on the
clinical and imaging characteristics. Symptomatic patients
typically present with snapping of the scapula, with or without
pain, on abduction and adduction of the shoulder. Surgical excision
is usually indicated for snapping scapula or tumor-related
discomfort. Several authors reported that marginal resection of ED
significantly relieves the symptoms (4–6).
However, a high incidence of postoperative complications, such as
development of seroma or hematoma, has been reported (5,7).
Previous studies recommend 3 weeks of immobilization of the
affected upper extremity (6) or
postoperative wound drainage and a compression bandage to avoid
these complications (8). Due to
the rarity of this tumor, the optimal operative approach and
postoperative treatment have not yet been determined. In this
study, we retrospectively reviewed 20 cases of surgically treated
ED to determine the association between postoperative complications
and preoperative patient characteristics or postoperative
treatment.
Materials and methods
Patients
A total of 20 consecutive cases of ED [8 men and 12
women; mean age, 63 years (range, 41–76 years)] who were surgically
treated at our institution between 2000 and 2012 were
retrospectively analyzed. The preoperative presentation of any
symptoms or disability and postoperative improvement were
reviewed.
Pre- and postoperative evaluation
All the cases were evaluated with magnetic resonance
imaging (MRI) prior to surgery. In 2 cases, biopsy had been
performed by the primary physician prior to referring the case to
our institution. All the patients underwent marginal resection and
the diagnosis was confirmed by a pathologist. To investigate
factors that may affect postoperative complications, the presence
of hypertension, tumor size, intraoperative bleeding and duration
of postoperative wound drainage were evaluated.
Prevalence
To evaluate the prevalence of ED in Japan, the Soft
Tissue Tumor Registry (Musculoskeletal Tumor Committee, Japanese
Orthopaedic Association), available since 2008 for benign and
malignant soft tissue tumors, was reviewed.
The present study was planned and conducted in
accordance with the ethical standards of the responsible committee
on human experimentation and conformed to the principles of the
Declaration of Helsinki.
Results
Clinical presentation
Fourteen patients (70%) presented with symptoms
associated with the tumor, including discomfort (3 cases), pain
around the scapula (6 cases) and snapping of the scapula with
shoulder motion (4 cases). The mass was incidentally discovered by
the patient or by another person, such as a family member, in 6
asymptomatic patients. Although mechanical stress is suspected to
be a cause of this disease, the occupations of the patients varied
and included physical labor (7 cases), office work (7 cases) and
being unemployed or working from home (6 cases) (Table I). ED was preoperatively diagnosed
based on location and imaging findings, although biopsy was
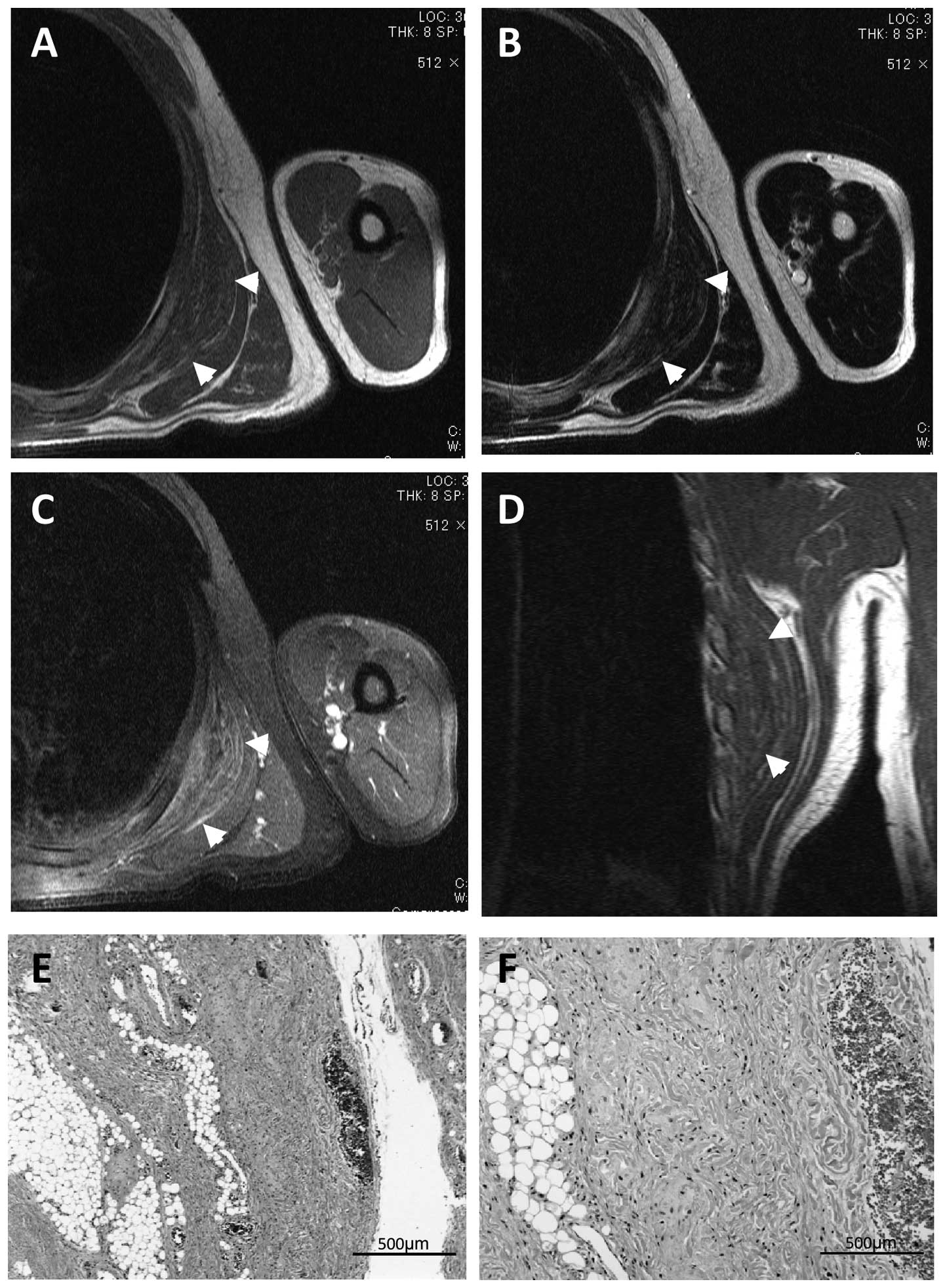
performed in the primary hospital in 2 cases. Preoperative MRI
revealed an unencapsulated and lenticular-shaped mass of low
intensity in T1-weighted images and iso- or low-intensity in
T2-weighted images, reflecting the fibrous tissue content of the
mass (Fig. 1), which is in
contrast to the characteristic high-intensity strands produced by
fatty tissue on T1-weighted images and intermediate-intensity
strands on T2-weighted images.
 | Table I.Summary of patients with elastofibroma
dorsi. |
Table I.
Summary of patients with elastofibroma
dorsi.
| Patient | Gender/Age
(years) | Location | Symptom | Occupation | Hypertension | Intraoperative
bleeding (g) | Hematoma | Wound drainage
(days) | Tumor diameter
(mm) |
|---|
| 1 | M/42 | Ra | Pain | Office worker | | 50 | + | 2 | 110 |
| 2 | M/41 | La | Snapping | Office worker | | 130 | + | 2 | 95 |
| 3 | F/72 | L | | Liquor-shop
employee | + | 10 | + | 4 | 90 |
| 4 | F/70 | R | | Farmer | | 15 | + | 4 | 110 |
| 5 | M/63 | R | | Office worker | | 100 | + | 3 | 90 |
| 6 | M/45 | R | | Office worker | | 80 | | 7 | 55 |
| 7 | F/73 | La | Snapping | | + | 30 | | 3 | 45 |
| 8 | F/76 | L | Discomfort | | + | 35 | | 4 | 50 |
| 9 | F/74 | L | Pain | | | 20 | + | 4 | 55 |
| 10 | F/50 | B | Snapping | Cook | | 40 | + | 7 | 70 |
| 11 | F/49 | La | Discomfort | | | 10 | | 9 | 48 |
| 12 | F/73 | Ra | Discomfort | | + | 10 | + | 7 | 45 |
| 13 | F/49 | R | | Care manager | | 105 | | 5 | 53 |
| 14 | M/71 | L | Discomfort | Liquor-shop
employee | + | 0 | | 7 | 80 |
| 15 | F/85 | L | Pain | Farmer | + | 5 | | 7 | 70 |
| 16 | F/58 | R | Pain | Nurse | | 15 | | 6 | 70 |
| 17 | M/64 | L | Pain | Office worker | | 125 | | 7 | 90 |
| 18 | M/64 | Ra | | Office worker | + | 90 | + | 4 | 80 |
| 19 | F/79 | L | Pain | | + | 5 | | 7 | 60 |
| 20 | M/58 | R | Snapping | Police officer | | 0 | | 7 | 63 |
Treatment
Based on the preoperative diagnosis of ED, all the
patients underwent marginal resection of the tumor. The standard
operative approach starts with a skin incision just superior to the
mass, followed by splitting of the latissimus dorsi muscle to
reveal the edematous serratus anterior muscle. By splitting the
serratus anterior muscle, the white and ill-defined tumor mass is
exposed. In the majority of the cases, the tumor was firmly
adherent to the serratus anterior muscle and thoracic wall,
requiring sharp dissection using scissors or electrocautery.
Macro- and microscopic
characteristics
Macroscopically, the resected tumors were whitish,
firm and an average of 72 mm (range, 45–110 mm) in diameter. The
cut surface was white and yellow, reflecting mixed fibrous and
fatty tissues.
On pathological examination, elastic and collagen
fibers coexisted with mature adipose tissue (Fig. 1E and F).
Complications
Postoperative hematoma occurred in 9 cases (43%) and
resolved with conservative treatment in 8 cases (Table I). One case with a massive
postoperative hematoma was treated with surgical evacuation, which
resulted in successful healing of the wound. Due to the high
incidence of postoperative hematoma, we analyzed the factors that
may affect the development of hematoma following ED resection. Age,
hypertension, the presence of preoperative tumor-related symptoms
and intraoperative bleeding were not found to be significantly
different between patients with (n=9) or without (n=11)
postoperative hematoma (Table II),
although tumor diameter was significantly larger in the hematoma
group (P=0.02) and the duration of postoperative drainage was
significantly longer in the non-hematoma group (P=0.01, Table II).
| Table II.Risk factors for postoperative
bleeding. |
Table II.
Risk factors for postoperative
bleeding.
| Factors | No hematoma
(n=11) | Hematoma (n=9) | P-value |
|---|
| Age, years (mean ±
SD) | 64.3±13.5 | 61±13.3 | 0.60 |
| Hypertension
(%) | 52.6 | 47.3 | 0.46 |
| Preoperative
symptom related to tumor (%) | 47.6 | 52.3 | 0.53 |
| Tumor diameter
(mm) | 62.1±14.1 | 82.8±22.7 | 0.02a |
| Intraoperative
bleeding (g) | 37.3±45.0 | 51.7±44.6 | 0.48 |
| Duration of
postoperative | 6.27±1.7 | 4.1±1.8 | 0.01a |
| drainage
(days) | | | |
Prevalence
The analysis of the Soft Tissue Tumor Registry
database revealed 130 cases of ED among a total of 12,557 soft
tissue tumor cases (1.0%). The distribution analysis of these130
cases revealed no geographic preference regarding the incidence of
ED in Japan. In our department, the incidence of ED was estimated
to be 2.7% of the 735 cases of surgically treated soft tissue
tumors between 2000 and 2012.
Discussion
Although ED is traditionally considered to be a rare
tumor (4,9), it is a well-recognized entity due to
the case reports published by several authors (3–6,9). The
incidence of ED in the general population has not been determined;
however, Brandser et al (10) reported in their computed tomography
(CT) study that ED was found in 2% of asymptomatic adults aged
>60 years. The results of that study were based on asymptomatic
cases; therefore, the actual prevalence of a symptomatic or
palpable ED mass is estimated to be <2%. A review of the
orthopaedic oncology database of the Royal Orthopaedic Hospital in
Birmingham, UK, revealed 15 cases of ED out of 17,500 cases
(0.086%) in >20 years (11). In
that series from UK, 11 patients underwent tumor resection, whereas
1 patient underwent needle biopsy only. We found the incidence of
ED in the Japanese Soft Tissue Tumor Registry to be 1.0%, which is
significantly higher compared to the incidence in the UK. The
incidence of ED was 2.7% in our department, which is more
consistent with the Japanese registry compared to the UK report
(11). This discrepancy may be
partly due to the difference in recognition of this entity between
UK and Japan; however, genetic factors may also play a role in its
geographic distribution. Hisaoka and Hashimoto (12), analyzed 14 cases from Fukuoka,
Japan, and demonstrated that spindle or stellate cells were
positive for CD34. CD34-positive mesenchymal cells are considered
to have the potential to differentiate into different lineages,
such as endothelial, myoid and adipocytic cells. Congenital or
acquired activation of certain factors, including CD34, and
long-term mechanical stimulation may cooperatively contribute to
the development of symptomatic or palpable ED. Positron-emission
tomography (PET) scanning recently became a common screening
technique for malignancies. Blumenkrantz et al (13) reported that, among 1,751 patients
undergoing PET-CT with 18F-fluorodeoxyglucose (FDG), 29
(1.66%) were diagnosed with ED. As the18F-FDG PET scan
has becomes more popular for cancer screening, more asymptomatic
cases of ED may be identified by radiologists. To avoid unnecessary
further examination or biopsy, radiologists and physicians should
be aware of the characteristic findings of ED (14,15).
Several authors recommend resection for symptomatic
cases only (5,7,11,15).
In the past, we recommended resection for symptomatic and
asymptomatic patients with tumors suspicious for ED, in order to
pathologically confirm the diagnosis. However, as the diagnosis of
ED is now easily made based on its clinical and imaging
characteristics, we only perform tumor resection in symptomatic
patients or in those who desire resection of the tumor. Although no
case in our study incurred permanent disability associated with
postoperative hematoma, the high incidence of hematoma discourages
surgical treatment of ED in asymptomatic cases. Other authors
reported the incidence of postoperative hematoma or seroma to be
38.9–87.5% (4,5,7),
which is considered to be a high incidence of postoperative
complication. As the occurrence of hematoma leads to additional
treatment (puncture, immobilization, or surgical evacuation) and
longer hospital stay, we generally recommend a week of
immobilization of the upper extremity on the affected side and
longer suction drainage (∼1 week) for ED. The results of the
present study demonstrated tumor size and duration of wound
drainage to be associated with the incidence of postoperative
hematoma. Surgeons should carefully observe the wound
postoperatively and apply negative pressure through the drainage
tube to facilitate wound healing, particularly in cases of large
(>80-mm) tumors.
In a different type of procedure, postoperative
seroma was shown to be a significant complication in the donor site
of a latissimus dorsi muscle flap (16). Although the dead space is larger in
the case of a latissimus dorsi flap compared to that following ED
resection, plastic surgeons have described several methods to
prevent postoperative seroma. The combination of quilting sutures
and fibrin sealant was recently shown to reduce the incidence of
postoperative seroma at the donor site (17,18);
this may also be applied to surgery for ED.
In conclusion, ED is a rare subscapular lesion
affecting mainly the elderly and it is easily diagnosed by its
characteristic location and imaging findings. Due to the high
incidence of postoperative complications, surgery should be
recommended only for symptomatic patients. To prevent the
development of postoperative hematoma or seroma, careful
observation of the wound with suction drainage and additional
surgical procedures to facilitate adhesion of the wound space are
recommended.
References
|
1.
|
Giebel GD, Bierhoff E and Vogel J:
Elastofibroma and preelastofibroma - a biopsy and autopsy study.
Eur J Surg Oncol. 22:93–96. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Nagamine N, Nohara Y and Ito E:
Elastofibroma in Okinawa. A clinicopathologic study of 170 cases.
Cancer. 50:1794–1805. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Naylor MF, Nascimento AG, Sherrick AD and
McLeod RA: Elastofibroma dorsi: radiologic findings in 12 patients.
AJR Am J Roentgenol. 167:683–687. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Parratt MT, Donaldson JR, Flanagan AM, et
al: Elastofibroma dorsi: management, outcome and review of the
literature. J Bone Joint Surg Br. 92:262–266. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Muramatsu K, Ihara K, Hashimoto T, Seto S
and Taguchi T: Elastofibroma dorsi: diagnosis and treatment. J
Shoulder Elbow Surg. 16:591–595. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Muratori F, Esposito M, Rosa F, et al:
Elastofibroma dorsi: 8 case reports and a literature review. J
Orthop Traumatol. 9:33–37. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Daigeler A, Vogt PM, Busch K, et al:
Elastofibroma dorsi - differential diagnosis in chest wall tumours.
World J Surg Oncol. 5:152007. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Nishio J, Isayama T, Iwasaki H and Naito
M: Elastofibroma dorsi: diagnostic and therapeutic algorithm. J
Shoulder Elbow Surg. 21:77–81. 2011. View Article : Google Scholar
|
|
9.
|
Mortman KD, Hochheiser GM, Giblin EM,
Manon-Matos Y and Frankel KM: Elastofibroma dorsi:
clinicopathologic review of 6 cases. Ann Thorac Surg. 83:1894–1897.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Brandser EA, Goree JC and El-Khoury GY:
Elastofibroma dorsi: prevalence in an elderly patient population as
revealed by CT. AJR Am J Roentgenol. 171:977–980. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Chandrasekar CR, Grimer RJ, Carter SR, et
al: Elastofibroma dorsi: an uncommon benign pseudotumour. Sarcoma.
2008:7565652008. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Hisaoka M and Hashimoto H: Elastofibroma:
clonal fibrous proliferation with predominant CD34-positive cells.
Virchows Arch. 448:195–199. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Blumenkrantz Y, Bruno GL, Gonzalez CJ,
Namias M, Osorio AR and Parma P: Characterization of elastofibroma
dorsi with 18FDG PET/CT: a retrospective study. Rev Esp
Med Nucl. 30:342–345. 2011.(In English, Spanish).
|
|
14.
|
Faccioli N, Foti G, Comai A, Cugini C,
Guarise A and Mucelli RP: MR imaging findings of elastofibroma
dorsi in correlation with pathological features: our experience.
Radiol Med. 114:1283–1291. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Go PH, Meadows MC, Deleon EM and
Chamberlain RS: Elastofibroma dorsi: a soft tissue masquerade. Int
J Shoulder Surg. 4:97–101. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Sajid MS, Betal D, Akhter N, Rapisarda IF
and Bonomi R: Prevention of postoperative seroma-related morbidity
by quilting of latissimus dorsi flap donor site: a systematic
review. Clin Breast Cancer. 11:357–363. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Bailey SH, Oni G, Guevara R, Wong C and
Saint-Cyr M: Latissimus dorsi donor-site morbidity: the combination
of quilting and fibrin sealant reduce length of drain placement and
seroma rate. Ann Plast Surg. 68:555–558. 2012. View Article : Google Scholar
|
|
18.
|
Shin IS, Lee DW and Lew DH: Efficacy of
quilting sutures and fibrin sealant together for prevention of
seroma in extended latissimus dorsi flap donor sites. Arch Plast
Surg. 39:509–513. 2012. View Article : Google Scholar : PubMed/NCBI
|