Introduction
Hepatocellular carcinoma (HCC) is one of the most
common malignancies worldwide. Recent advances in imaging
technology and implementation of surveillance programs for
high-risk patients have led to increased detection of early-stage
HCC, making curative therapies possible in some patients (1,2).
However, the long-term survival of HCC patients remains
unsatisfactory, due to the high frequency of intra- and
extrahepatic recurrence (3,4). In
particular, the development of advanced HCC with extrahepatic
metastasis hinders the use of curative therapies, such as surgical
resection or radiofrequency ablation, therefore contributing to
poor survival. Prior to the approval of sorafenib, several systemic
chemotherapeutic regimens had been evaluated for patients with
advanced HCC, although no effective therapeutic protocols were
identified (5,6). Two randomized placebo-controlled
trials demonstrated a survival benefit associated with sorafenib
for patients with advanced HCC, including those with extra-hepatic
metastasis (7,8). As a result, sorafenib is currently
considered to be the standard treatment for advanced HCC in the
United States, Europe, Japan and a number of other countries
(9,10). However, although sorafenib appears
to prolong survival, this benefit remains unsatisfactory.
Therefore, the development of novel agents and/or combinations is
required for patients with advanced HCC with extrahepatic
metastasis. To design optimal therapies, it is crucial to
understand the clinical characteristics and prognostic factors of
these patients.
In our clinic, we encountered several HCC patients
whose disease progressed to extrahepatic metastasis, despite the
administration of appropriate, repeated treatment for intrahepatic
tumors, whereas we also encountered patients who were initially
diagnosed with HCC with extrahepatic metastasis at presentation
and, therefore, have not been previously treated for HCC. As
regards patients with advanced HCC with extrahepatic metastasis,
several previous studies only reported the clinicopathological
characteristics and prognosis of patients with HCC recurrence or a
combined set of previously treated and untreated patients (11–14).
We hypothesized that the previous treatment of intrahepatic tumors
may affect the subsequent pattern of metastasis and prognosis among
patients with advanced HCC with extrahepatic metastasis. Therefore,
it is crucial to determine the characteristics of pure advanced HCC
with extrahepatic metastasis that has not been previously treated.
In addition, to the best of our knowledge, no studies have compared
the differences between patients with advanced HCC with
extrahepatic metastasis who received and those who did not receive
previous treatment. Consequently, in this study, we aimed to
compare the clinical characteristics and prognostic factors of
previously treated and untreated patients with advanced HCC with
extrahepatic metastasis.
Patients and methods
Patients
Between April, 1998 and April, 2012, a total of 419
patients who were diagnosed with advanced HCC with extrahepatic
metastasis at the Kurume University School of Medicine, Kurume,
Japan, were enrolled in this study. Hepatic functional reserve was
determined using the Child-Pugh classification system. HCC tumor
staging was performed using the 6th edition of the American Joint
Committee on Cancer/Union for International Cancer Control TNM
classification system (15). At
diagnosis of HCC with extrahepatic metastasis, 338 patients (80.7%)
had received previous treatment and 81 patients (19.3%) were
untreated. Previous treatments for intrahepatic tumors included
hepatic resection in 65 patients (19.2%), percutaneous ethanol
injection in 82 patients (24.3%), radiofrequency ablation in 83
patients (24.6%), transcatheter chemoembolization (TACE) in 204
patients (60.4%) and hepatic arterial infusion chemotherapy (HAIC)
in 197 patients (58.3%). The patients included 353 men (84.3%) and
66 women, with a median age of 66.0 years (range, 15–92 years).
Overall, 291 patients (69.5%) were found to be positive for
hepatitis C virus (HCV) and 75 patients (17.9%) were positive for
hepatitis B virus (HBV) infection. A total of 208, 149 and 62
patients were classified as Child-Pugh class A, B and C,
respectively, whereas 55, 186 and 175 patients had T0–2, T3 and T4
stage primary tumors, respectively. Extrahepatic metastases were
detected in the lungs in 225 (53.7%), bones in 165 (39.4%), lymph
nodes in 91 (21.7%) and adrenal glands in 44 patients (10.5%).
Diagnosis of HCC and evaluation of
extrahepatic lesions
The diagnosis of HCC was radiologically confirmed by
hyperintensity in the arterial phase and washout in the venous and
delayed phase, using either contrast-enhanced computed tomography
(CT) or magnetic resonance imaging (MRI) (9) and/or by elevated serum levels of
α-fetoprotein (AFP) and des-γ-carboxy prothrombin (DCP). Tumor
biopsy was performed in cases in which imaging findings were not
consistent with the characteristic features of HCC, or when tumor
marker levels were not elevated. To evaluate extrahepatic
metastasis, pulmonary lesions were detected on chest X-ray or chest
CT, which were routinely performed at the first visit or every 3–6
months during the follow-up period. Additional examinations, such
as bone scintigraphy and brain CT or MRI, were indicated upon
development of symptoms attributable to extrahepatic metastasis.
These examinations were also conducted when AFP and/or DCP levels
were elevated and the elevation(s) could not be attributed to the
status of the intrahepatic lesion(s). Positron emission
tomography/CT studies were performed as a supplemental
examination.
Follow-up and endpoint
Following HCC diagnosis, each patient was carefully
followed up with respect to intrahepatic lesions and extrahepatic
metastases. Serum biochemistries, AFP and DCP levels were measured
and ultrasonography was performed every 1–2 months. Contrast CT or
MRI was performed every 2–6 months. Other imaging modalities were
used as necessary. The endpoint of this study was the date of
death, or last follow-up visit; the closing date was August, 2012.
The median duration of the follow-up was 5.8 months (range,
0.2-111.9 months).
Statistical analysis
The continuous variables are expressed as median
values (range). A comparison analysis between patients who received
and those who did not receive previous treatment was performed
using the Chi-square test for discrete variables and the
Mann-Whitney U test for continuous variables. Overall survival was
determined by the Kaplan-Meier analysis and the differences between
subgroups were compared with log-rank tests. A Cox proportional
hazards stepwise model was used for univariate and multivariate
analysis, in order to identify any independent variables associated
with overall survival. Data from these models are expressed as
hazard ratios (HRs) and 95% confidence intervals (CIs). All P
values were two-tailed and P<0.05 was considered to indicate a
statistically significant difference. The statistical analysis was
performed using SPSS software, version 20 (SPSS, Inc., Chicago, IL,
USA).
Results
Clinical characteristics of patients
A comparison of the clinical characteristics of
patients who received and those who did not receive previous
treatment is shown in Table I.
Previously treated patients were significantly more likely to have
HCV infection, Child-Pugh class B+C and a low primary tumor stage,
compared to previously untreated patients. Previously untreated
patients exhibited a significantly lower neutrophil-lymphocyte
ratio (NLR) and higher aspartate aminotransferase (AST) levels,
white blood cell counts, platelet counts and DCP levels, compared
to previously treated patients. The major metastatic sites, which
were the lungs, bones, lymph nodes and adrenal glands were similar
in the two groups.
 | Table I.Comparison of clinical characteristics
between previously treated and untreated patients. |
Table I.
Comparison of clinical characteristics
between previously treated and untreated patients.
| Characteristics | Previously untreated
patients (n=81) | Previously treated
patients (n=338) | P-value |
|---|
| Gender
(male/female) | 70/11 | 283/55 | 0.523 |
| Age, years
(range) | 63 (15–80) | 67 (30–92) | <0.001 |
| Etiology
(HCV/HBV/other) | 44/18/19 | 246/57/35 | 0.006 |
| Child-Pugh class
(A/B/C) | 56/17/8 | 152/132/54 | <0.001 |
| AST (U/l) | 52 (12–280) | 36 (6–412) | <0.001 |
| White blood cell
count (×109/l) | 5.7 (2.8–20.3) | 4.4 (1.4–20.5) | <0.001 |
| NLR | 2.8 (0.8–18.0) | 3.1 (0.6–46.5) | 0.038 |
| Platelet count
(×109/l) | 139 (33–675) | 101 (20–970) | <0.001 |
| AFP (ng/ml) | 1444.9
(2.2–3,311,794.0) | 524.9
(1.5–1,904,794.0) | 0.177 |
| DCP (mAU/ml) | 11400
(19–75,000) | 887.5
(8–75,000) | <0.001 |
| Primary tumor
stagea
(T0–2/T3/T4) | 2/30/49 | 53/156/126b | <0.001 |
| Site of
extrahepatic metastasis | | | |
| Lungs | 53.1% (43) | 53.8% (182) | 0.905 |
| Bones | 43.2% (35) | 38.5% (130) | 0.410 |
| Lymph nodes | 29.6% (24) | 19.8% (67) | 0.059 |
| Adrenal
glands | 13.6% (11) | 9.8% (33) | 0.306 |
| Peritoneum and
pleura | 2.5% (2) | 7.4% (25) | 0.107 |
| Diaphragm | 4.9% (4) | 5.0% (17) | 0.982 |
| Brain | 1.2% (1) | 3.0% (10) | 0.387 |
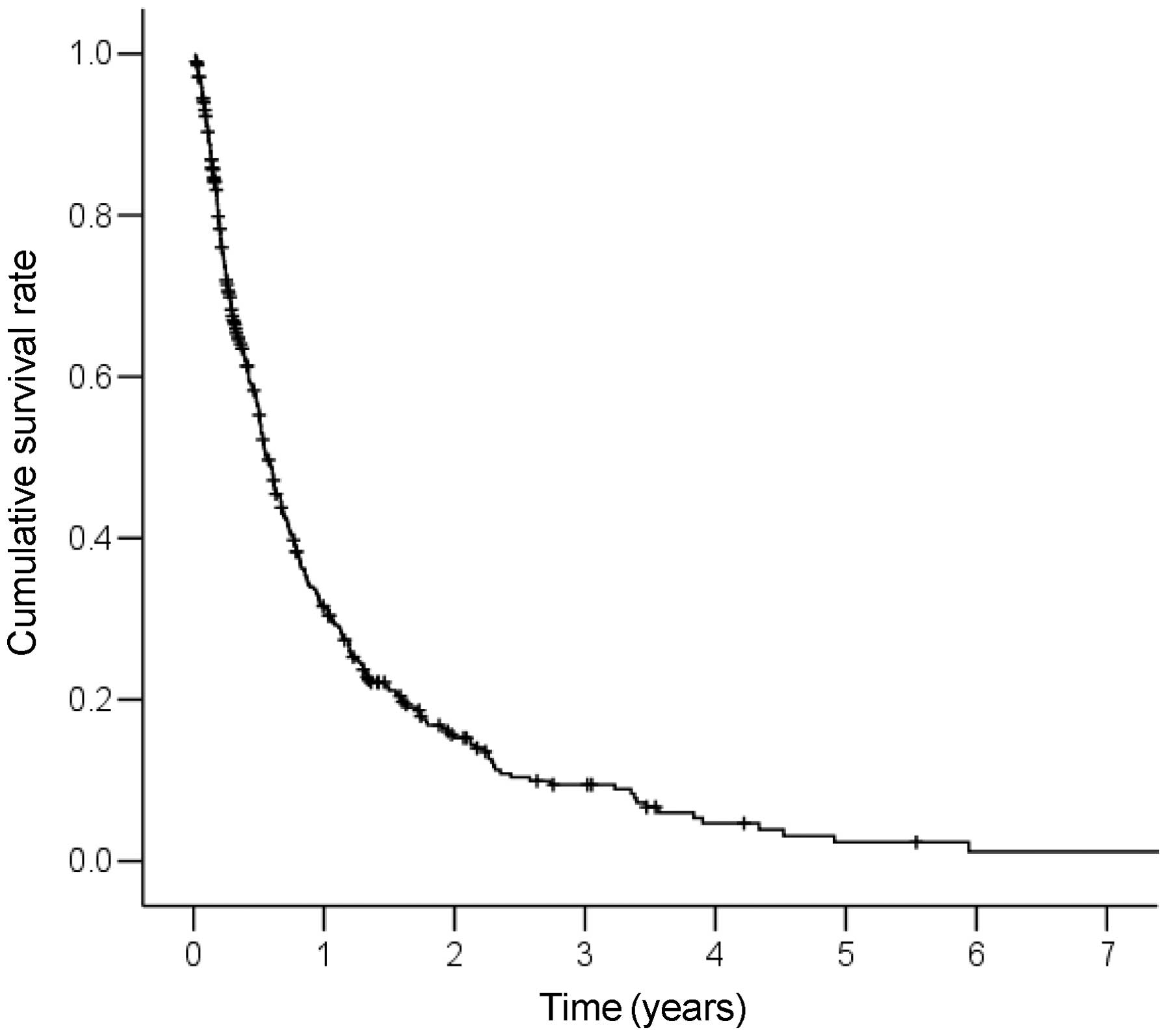
Survival and predictive factors in all
the patients
The cumulative survival curve of the 419 patients is
shown in Fig. 1. The median
survival time (MST) for these patients was 6.8 months. The 1-, 2-,
3- and 5-year survival rates were 31.6, 15.3, 9.5 and 2.3%,
respectively. A Cox proportional hazards regression analysis was
performed to identify independent predictors of survival (Table II). The results of the univariate
analysis demonstrated that Child-Pugh class (B+C), white blood cell
count (≥6.0×109/l), NLR (≥4.0), AFP levels (≥200 ng/ml)
and primary tumor stage (T4) were significant risk factors that
adversely affected survival. The multivariate analysis identified
Child-Pugh class B+C (HR=2.80; 95% CI: 2.23–3.52; P<0.001),
white blood cell count ≥6.0×109/l (HR=1.82; 95% CI:
1.43–2.33; P<0.001), NLR ≥4.0 (HR=1.89; 95% CI: 1.48–2.41;
P<0.001), AFP ≥200 ng/ml (HR=1.48; 95% CI: 1.18–1.87; P=0.001)
and primary tumor stage T4 (HR=1.43; 95% CI: 1.14–1.79; P=0.002) as
independent predictors of survival.
| Table II.Univariate and multivariate analysis
of survival in all 419 patients with HCC and extrahepatic
metastasis. |
Table II.
Univariate and multivariate analysis
of survival in all 419 patients with HCC and extrahepatic
metastasis.
| Variables | Univariate HR (95%
CI) | P-value | Multivariate HR
(95% CI) | P-value |
|---|
| Gender (male) | 0.96
(0.71–1.29) | 0.773 | - | - |
| Age (≥65
years) | 1.10
(0.89–1.37) | 0.374 | - | - |
| Etiology (HCV
infection) | 1.01
(0.80–1.28) | 0.909 | - | - |
| Child-Pugh class
(B+C) | 2.82
(2.25–3.53) | <0.001 | 2.80
(2.23–3.52) | <0.001 |
| AST (≥80 U/l) | 1.15
(0.87–1.51) | 0.335 | - | - |
| White blood cell
count (≥6.0×109/l) | 1.85
(1.45–2.35) | <0.001 | 1.82
(1.43–2.33) | <0.001 |
| NLR (≥4.0) | 2.48
(1.96–3.13) | <0.001 | 1.89
(1.48–2.41) | <0.001 |
| Platelet count
(≥120×109/l) | 0.93
(0.75–1.15) | 0.504 | - | - |
| AFP (≥200
ng/ml) | 1.74
(1.39–2.18) | <0.001 | 1.48
(1.18–1.87) | 0.001 |
| DCP (≥200
mAU/ml) | 1.10
(0.99–1.22) | 0.073 | - | - |
| Primary tumor
stagea (T4) | 1.57
(1.27–1.95) | <0.001 | 1.43
(1.14–1.79) | 0.002 |
| Previous treatment
(present) | 1.13
(0.87–1.48) | 0.370 | - | - |
| Site of
extrahepatic metastasis | | | | |
| Lungs | 0.93
(0.75–1.15) | 0.480 | - | - |
| Bones | 1.23
(0.99–1.52) | 0.066 | - | - |
| Lymph nodes | 0.96
(0.74–1.24) | 0.732 | - | - |
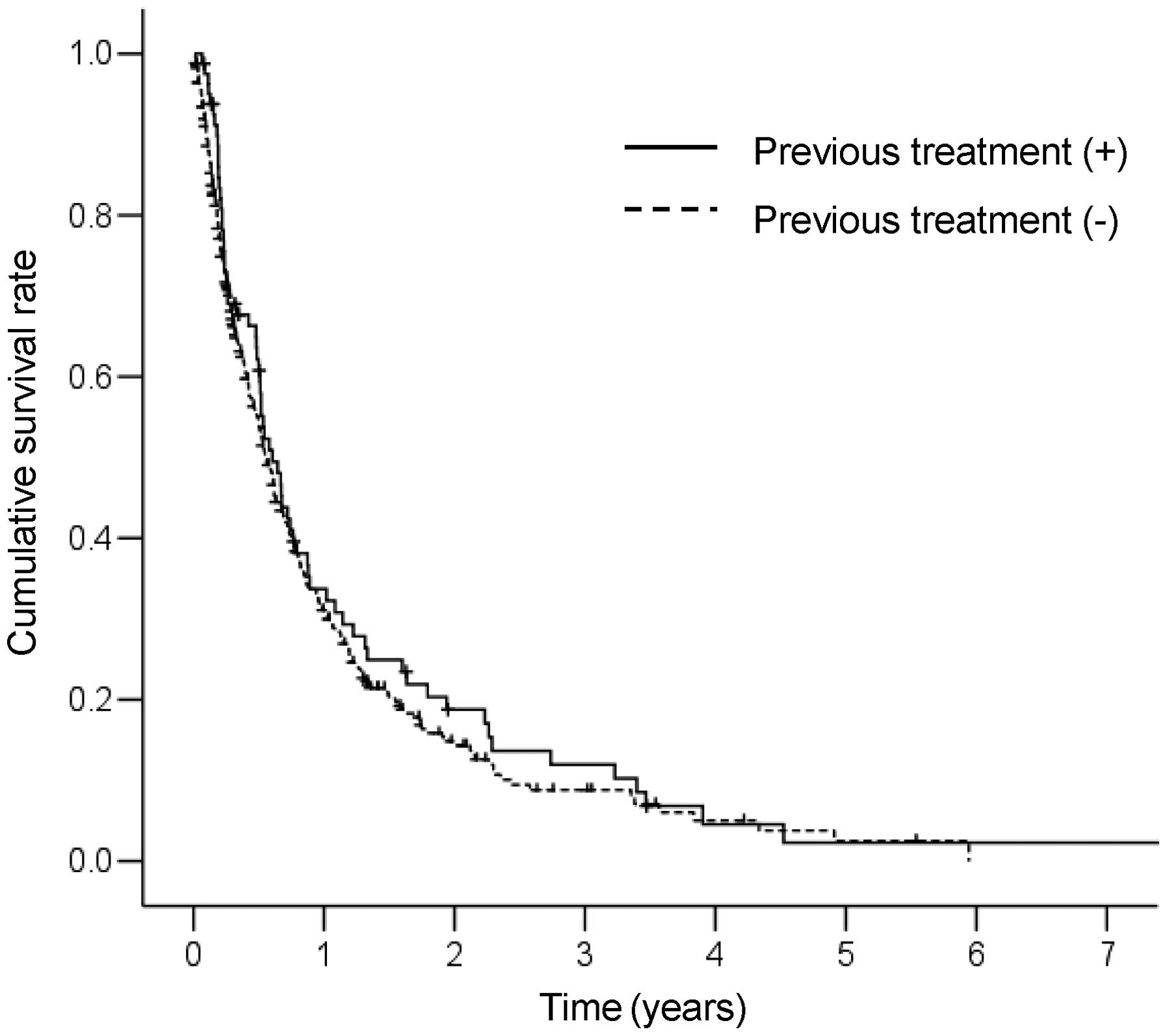
Survival and predictive factors in 81
previously untreated patients
The cumulative survival curve of the 81 patients who
did not receive previous treatment is shown in Fig. 2. The MST for these patients was 7.4
months. The 1-, 2-, 3- and 5-year survival rates were 33.7, 18.8,
11.9 and 2.3%, respectively. No significant differences in survival
between patients who received and those who did not receive
previous treatment were observed (P=0.369). A Cox proportional
hazards regression analysis was performed to identify independent
predictors of survival (Table
III). The results of the univariate analysis revealed that
Child-Pugh class (B+C), white blood cell count
(≥6.0×109/l), NLR (≥4.0) and primary tumor stage (T4)
were significant risk factors that adversely affected survival. The
multivariate analysis identified Child-Pugh class B+C (HR=6.03; 95%
CI: 3.31–10.99; P<0.001), white blood cell count
≥6.0×109/l (HR=1.85; 95% CI: 1.09–3.15; P=0.023), NLR
≥4.0 (HR=1.86; 95% CI: 1.01–3.43; P=0.047) and primary tumor stage
T4 (HR=1.82; 95% CI: 1.10–2.99; P=0.019) as independent predictors
of survival.
| Table III.Univariate and multivariate analysis
of survival in previously untreated patients with HCC and
extrahepatic metastasis. |
Table III.
Univariate and multivariate analysis
of survival in previously untreated patients with HCC and
extrahepatic metastasis.
| Variables | Univariate HR (95%
CI) | P-value | Multivariate HR
(95% CI) | P-value |
|---|
| Gender (male) | 1.33
(0.66-2.72) | 0.427 | - | - |
| Age (≥65
years) | 1.04
(0.64–1.68) | 0.872 | - | - |
| Etiology (HCV
infection) | 0.79
(0.49–1.29) | 0.351 | - | - |
| Child-Pugh class
(B+C) | 5.66
(3.22–9.94) | <0.001 | 6.03
(3.31–10.99) | <0.001 |
| AST (≥80 U/l) | 1.13
(0.66–1.93) | 0.659 | - | - |
| White blood cell
count (≥6.0×109/l) | 1.97
(1.18–3.29) | 0.009 | 1.85
(1.09–3.15) | 0.023 |
| NLR (≥4.0) | 2.57
(1.44–4.56) | 0.001 | 1.86
(1.01–3.43) | 0.047 |
| Platelet count
(≥120×109/l) | 1.25
(0.75–2.08) | 0.387 | - | - |
| AFP (≥200
ng/ml) | 1.43
(0.85–2.39) | 0.175 | - | - |
| DCP (≥200
mAU/ml) | 1.05
(0.56–1.96) | 0.885 | - | - |
| Primary tumor
stagea (T4) | 1.64
(1.00–2.67) | 0.048 | 1.82
(1.10–2.99) | 0.019 |
| Site of
extrahepatic metastasis | | | | |
| Lungs | 0.93
(0.57–1.53) | 0.783 | - | - |
| Bones | 1.30
(0.800–2.13) | 0.292 | - | - |
| Lymph nodes | 1.23
(0.69–2.19) | 0.482 | - | - |
Discussion
It has not been determined whether previous
treatment affects the clinical characteristics and prognosis in
patients with advanced HCC and extrahepatic metastasis. In this
study, we aimed to evaluate whether there are differences between
patients with advanced HCC and extrahepatic metastasis who received
and those who did not receive previous treatment. Our results
revealed differences in various clinical characteristics between
these two groups of patients. Previously treated patients were more
likely to exhibit low white blood cell counts, low platelet counts
and poor liver function compared to previously untreated patients.
A possible explanation for this observation is that leukocytopenia
and thrombocytopenia may have been caused by previously
administered anticancer drugs, as several patients had repeatedly
undergone TACE and HAIC for intrahepatic tumors. In addition,
repeated cancer recurrence and various treatments for intrahepatic
tumors may have contributed to decreased liver function. Of note,
previously untreated patients had more advanced-stage intrahepatic
tumors compared to previously treated patients. Previous studies
suggested that residual HCC following various treatments is
associated with increased malignant potential compared to untreated
HCC (16–18). Therefore, we suggest that
aggressive treatment may result in earlier extrahepatic metastasis,
despite a less advanced intrahepatic tumor stage, in previously
treated patients. In this study, no significant differences in
survival between the two groups were observed, although the groups
differed in liver function and intrahepatic tumor stage. A possible
explanation for this lack of difference is that worse liver
function and an increased malignant potential of previously treated
patients may offset the more advanced stage of intrahepatic tumors
of previously untreated patients.
The major sites of HCC metastasis included the
lungs, lymph nodes, bones and adrenal glands (13,14,19–21).
Yoo et al (20) reported
that the most frequent metastatic sites in 251 previously untreated
HCC patients with extrahepatic metastasis were the lungs (67.3%),
lymph nodes (37.5%), bones (18.3%) and adrenal glands (7.6%). Jun
et al (14) indicated that
in HCC patients with extrahepatic recurrence following hepatic
resection, frequent metastatic sites included the lungs (41.9%),
lymph nodes (19.9%) and bones (13.2%). In the present study, the
most frequent site of extrahepatic metastasis was the lungs,
followed by the bones, lymph nodes and adrenal glands, regardless
of previous treatment of intrahepatic tumors. These results are
similar to those previously reported and suggest that previous
treatment does not affect the metastatic pattern of HCC.
Several studies reported that in HCC patients with
extra-hepatic metastasis, intrahepatic tumor status and Child-Pugh
classification are independent prognostic factors (12,13,20).
Similarly, in the present study, the multivariate analysis
demonstrated that these factors were independent predictors of
survival in HCC patients with extrahepatic metastasis, regardless
of previous treatment. Sorafenib is an oral systemic agent that
prolongs overall survival and has become the standard treatment for
patients with advanced HCC, including those with extrahepatic
metastasis. However, even the survival rates achieved with
sorafenib remain unsatisfactory. Several studies reported that the
characteristics of primary tumor progression, such as vascular
invasion, tumor size and tumor number, are independent risk factors
for extrahepatic metastasis following curative resection (14,22).
Thus, the control of intrahepatic tumors may be important for the
prevention of further extra-hepatic metastasis. Pinter et al
(23) reported that the MST of
TACE alone (9.2 months) was similar to that of sorafenib alone (7.4
months) in patients with advanced HCC, including those with
extrahepatic metastasis. Jun et al (14) reported that in 240 HCC patients
with extrahepatic metastasis, the control of intrahepatic tumors
was a favorable prognostic factor for survival: the MST of patients
exhibiting a treatment response was significantly longer compared
to that of patients who did not respond to treatment (521 vs. 170
days; P<0.001). Consequently, in advanced HCC patients with
extrahepatic metastasis, a combination of intrahepatic local
treatments and sorafenib may be useful, as the malignant potential
of intrahepatic tumors is associated with extrahepatic spread and
survival.
Hepatic reserve is important for hepatic resection
and metabolism of anticancer drugs, including sorafenib. Pinter
et al (24) reported that
the risk of high-grade toxicities associated with sorafenib may be
increased in patients with advanced liver dysfunction. Our previous
study of advanced HCC patients treated with HAIC demonstrated that
liver dysfunction necessitating treatment suspension or
discontinuation occurred more frequently in patients with
Child-Pugh class B compared to patients with Child-Pugh class A
disease (25). Such insufficient
treatment may lead to further liver dysfunction, due to
intrahepatic tumor progression, resulting in poor survival.
Therefore, we considered liver function to be an important
predictor of survival.
In this study, we also demonstrated that an elevated
white blood cell count associated with a high NLR was a significant
independent predictor of survival in HCC patients with extrahepatic
metastasis. Recently, various markers of systemic inflammatory
responses, including cytokines, C-reactive protein and absolute
blood neutrophil or lymphocyte count, as well as their ratio
(including NLR), have been investigated for their prognostic roles
in cancer. Of these, NLR is one of the most simple and effective
markers of inflammation and is linked with poor prognosis in
various cancer types (26–28). Several studies demonstrated that an
elevated NLR was associated with worse survival in patients with
HCC who underwent radiofrequency ablation, TACE, resection and
liver transplantation (29–32).
However, the exact association between a high NLR and poor
prognosis has not been fully elucidated. One possible explanation
is that patients with an elevated NLR have relative
lymphocytopenia, leading to a weaker lymphocyte-mediated immune
response to the tumor due to a decreasing T4/T8 ratio (33). As a result, these patients may
experience a more rapid tumor progression and, therefore, have a
poor prognosis. Another explanation is that the increased
neutrophil numbers may modify and provide an adequate environment
for tumor progression and development. Neutrophils have been shown
to promote tumor growth and metastasis by secreting chemokines,
vascular endothelial growth factor and matrix metalloproteinase-9,
which are involved in the angiogenesis that promotes tumor
development (34–36). Thus, a high neutrophil level may
offer a growth advantage for HCC through the increase of these
pro-angiogenic factors, resulting in increased extrahepatic
metastasis and worse survival in HCC patients.
In conclusion, we demonstrated that there are
differences in the clinical characteristics and no significant
differences in survival between patients with advanced HCC with
extrahepatic metastasis who received and those who did not receive
previous treatment. Moreover, we demonstrated that intrahepatic
tumor status, Child-Pugh classification, white blood cell count and
NLR are independent predictors of survival in HCC patients with
extrahepatic metastasis, regardless of previous treatment of
intrahepatic tumors.
References
|
1.
|
Takayama T, Makuuchi M, Hirohashi S, et
al: Early hepatocellular carcinoma as an entity with a high rate of
surgical cure. Hepatology. 28:1241–1246. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Zhang BH, Yang BH and Tang ZY: Randomized
controlled trial of screening for hepatocellular carcinoma. J
Cancer Res Clin Oncol. 130:417–422. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Portolani N, Coniglio A, Ghidoni S, et al:
Early and late recurrence after liver resection for hepatocellular
carcinoma: prognostic and therapeutic implications. Ann Surg.
243:229–235. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Yang Y, Nagano H, Ota H, et al: Patterns
and clinicopathologic features of extrahepatic recurrence of
hepatocellular carcinoma after curative resection. Surgery.
141:196–202. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Burroughs A, Hochhauser D and Meyer T:
Systemic treatment and liver transplantation for hepatocellular
carcinoma: two ends of the therapeutic spectrum. Lancet Oncol.
5:409–418. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Nowak AK, Chow PK and Findlay M: Systemic
therapy for advanced hepatocellular carcinoma: a review. Eur J
Cancer. 40:1474–1484. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Llovet JM, Ricci S, Mazzaferro V, et al:
Sorafenib in advanced hepatocellular carcinoma. N Engl J Med.
359:378–390. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Cheng AL, Kang YK, Chen Z, et al: Efficacy
and safety of sorafenib in patients in the Asia-Pacific region with
advanced hepatocellular carcinoma: a phase III randomised,
double-blind, placebo-controlled trial. Lancet Oncol. 10:25–34.
2009. View Article : Google Scholar
|
|
9.
|
Bruix J and Sherman M; American
Association for the Study of Liver Diseases: Management of
hepatocellular carcinoma: an update. Hepatology. 53:1020–1022.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Kudo M, Izumi N, Kokudo N, et al HCC
Expert Panel of Japan Society of Hepatology: Management of
hepatocellular carcinoma in Japan: Consensus-Based Clinical
Practice Guidelines proposed by the Japan Society of Hepatology
(JSH) 2010 updated version. Dig Dis. 29:339–364. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Sasaki A, Kai S, Endo Y, et al: Hepatitis
B virus infection predicts extrahepatic metastasis after hepatic
resection in patients with large hepatocellular carcinoma. Ann Surg
Oncol. 14:3181–3187. 2007. View Article : Google Scholar
|
|
12.
|
Uka K, Aikata H, Takaki S, et al: Clinical
features and prognosis of patients with extrahepatic metastases
from hepatocellular carcinoma. World J Gastroenterol. 13:414–420.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Uchino K, Tateishi R, Shiina S, et al:
Hepatocellular carcinoma with extrahepatic metastasis: clinical
features and prognostic factors. Cancer. 117:4475–4483. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Jun L, Zhenlin Y, Renyan G, et al:
Independent factors and predictive score for extrahepatic
metastasis of hepatocellular carcinoma following curative
hepatectomy. Oncologist. 17:963–969. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Pawlik TM, Esnaola NF and Vauthey JN:
Surgical treatment of hepatocellular carcinoma: similar long-term
results despite geographic variations. Liver Transpl. 10(Suppl 1):
S74–S80. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Shim JH, Park JW, Kim JH, et al:
Association between increment of serum VEGF level and prognosis
after transcatheter arterial chemoembolization in hepatocellular
carcinoma patients. Cancer Sci. 99:2037–2044. 2008.
|
|
17.
|
Paez-Ribes M, Allen E, Hudock J, et al:
Antiangiogenic therapy elicits malignant progression of tumors to
increased local invasion and distant metastasis. Cancer Cell.
15:220–231. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Kong J, Kong J, Pan B, et al: Insufficient
radiofrequency ablation promotes angiogenesis of residual
hepatocellular carcinoma via HIF-1alpha/VEGFA. PLoS One.
7:e372662012. View Article : Google Scholar
|
|
19.
|
Katyal S, Oliver JH III, Peterson MS,
Ferris JV, Carr BS and Baron RL: Extrahepatic metastases of
hepatocellular carcinoma. Radiology. 216:698–703. 2000. View Article : Google Scholar
|
|
20.
|
Yoo DJ, Kim KM, Jin YJ, et al: Clinical
outcome of 251 patients with extrahepatic metastasis at initial
diagnosis of hepatocellular carcinoma: does transarterial
chemoembolization improve survival in these patients? J
Gastroenterol Hepatol. 26:145–154. 2011. View Article : Google Scholar
|
|
21.
|
Natsuizaka M, Omura T, Akaike T, et al:
Clinical features of hepatocellular carcinoma with extrahepatic
metastases. J Gastroenterol Hepatol. 20:1781–1787. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Ochiai T, Ikoma H, Okamoto K, Kokuba Y,
Sonoyama T and Otsuji E: Clinicopathologic features and risk
factors for extrahepatic recurrences of hepatocellular carcinoma
after curative resection. World J Surg. 36:136–143. 2012.
View Article : Google Scholar
|
|
23.
|
Pinter M, Hucke F, Graziadei I, et al:
Advanced-stage hepatocellular carcinoma: transarterial
chemoembolization versus sorafenib. Radiology. 263:590–599. 2012.
View Article : Google Scholar
|
|
24.
|
Pinter M, Sieghart W, Graziadei I, et al:
Sorafenib in unresectable hepatocellular carcinoma from mild to
advanced stage liver cirrhosis. Oncologist. 14:70–76. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Niizeki T, Sumie S, Torimura T, et al:
Serum vascular endothelial growth factor as a predictor of response
and survival in patients with advanced hepatocellular carcinoma
undergoing hepatic arterial infusion chemotherapy. J Gastroenterol.
47:686–695. 2012. View Article : Google Scholar
|
|
26.
|
Ding PR, An X, Zhang RX, et al: Elevated
preoperative neutrophil to lymphocyte ratio predicts risk of
recurrence following curative resection for stage IIA colon cancer.
Int J Colorectal Dis. 25:1427–1433. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Jung MR, Park YK, Jeong O, et al: Elevated
preoperative neutrophil to lymphocyte ratio predicts poor survival
following resection in late stage gastric cancer. J Surg Oncol.
104:504–510. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Stotz M, Gerger A, Eisner F, et al:
Increased neutrophillymphocyte ratio is a poor prognostic factor in
patients with primary operable and inoperable pancreatic cancer. Br
J Cancer. 109:416–421. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Gomez D, Farid S, Malik HZ, et al:
Preoperative neutrophil-to-lymphocyte ratio as a prognostic
predictor after curative resection for hepatocellular carcinoma.
World J Surg. 32:1757–1762. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30.
|
Halazun KJ, Hardy MA, Rana AA, et al:
Negative impact of neutrophil-lymphocyte ratio on outcome after
liver transplantation for hepatocellular carcinoma. Ann Surg.
250:141–151. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31.
|
Huang ZL, Luo J, Chen MS, Li JQ and Shi M:
Blood neutrophil-to-lymphocyte ratio predicts survival in patients
with unresectable hepatocellular carcinoma undergoing transarterial
chemoembolization. J Vasc Interv Radiol. 22:702–709. 2011.
View Article : Google Scholar
|
|
32.
|
Chen TM, Lin CC, Huang PT and Wen CF:
Neutrophil-tolymphocyte ratio associated with mortality in early
hepatocellular carcinoma patients after radiofrequency ablation. J
Gastroenterol Hepatol. 27:553–561. 2012. View Article : Google Scholar
|
|
33.
|
Chew V, Tow C, Teo M, et al: Inflammatory
tumour microenvironment is associated with superior survival in
hepatocellular carcinoma patients. J Hepatol. 52:370–379. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
34.
|
Coussens LM, Tinkle CL, Hanahan D and Werb
Z: MMP-9 supplied by bone marrow-derived cells contributes to skin
carcinogenesis. Cell. 103:481–490. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
35.
|
Strieter RM, Burdick MD, Mestas J,
Gomperts B, Keane MP and Belperio JA: Cancer CXC chemokine networks
and tumour angiogenesis. Eur J Cancer. 42:768–778. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
36.
|
Gong Y and Koh DR: Neutrophils promote
inflammatory angiogenesis via release of preformed VEGF in an in
vivo corneal model. Cell Tissue Res. 339:437–448. 2010. View Article : Google Scholar : PubMed/NCBI
|