Introduction
Nasopharyngeal carcinoma (NPC) has a unique racial
and geographical epidemiology, with the highest rate of occurrence
in Guangdong (southern China). The majority of NPC cases that occur
in this high-risk area are poorly-differentiated and prone to
infiltrative growth and metastasis. The metastatic incidence of
neck lymph node may be as high as 78.9% (1).
Radiotherapy is indispensable for comprehensive NPC
treatment. With the development of radiotherapy techniques, the
5-year overall survival (OS) rate of NPC has increased from 40% in
the 1960s (2) to 75% by the end of
the 1990s (3), and to >80% due
to the introduction of intensity-modulation radiation therapy
(IMRT) (4). As survival rates have
increased, the concern of the late complications due to
radiotherapy have also increased. The clinical target volume (CTV)
of the lymph node neck levels is one critical area for reducing the
side-effects of radiotherapy. The most problematic one is the CTV
of the level Ib lymph node, which mainly comprises the
submandibular lymph node surrounding the submandibular gland (SMG)
(5).
The metastatic incidence of the level Ib lymph node
ranges from 2.0–8.5% according to image-based analysis (6–8).
During the 2D radiotherapy era, the entire region of level Ib was
included in the CTV. As the irradiation of the level Ib lymph node
can significantly increase the dose absorbed by the surrounding
normal tissues, the function of SMG could be extremely damaged.
Damage to the salivary glands results in xerostomia in >90%
patients (9). The study by Kuten
et al (10) reported that a
reduced dose to the SMG could effectively alleviate xerostomia.
Certain surgeons have developed SMG-transfer surgery to preserve
the SMG and this procedure achieves good results (11,12),
but the invasiveness limits its use in clinical practice. In the
IMRT era, numerous studies identified the importance of SMG
protection as it was observed that xerostomia could not be
sufficiently reduced when the parotid gland was well preserved and
the SMG was not (13–16). In principle, determining the target
volume for the level Ib lymph node is problematic. Due to the
low-metastatic rate of level Ib, selective irradiation may be
reasonable. Specific indications for the irradiation of level Ib
lymph nodes have been formulated (17,18),
but the clinical evidence is not convincing.
Therefore, the present study was performed to
provide certain evidence-based indications for the irradiation of
level Ib lymph node in NPC. First, the independent risk factors for
the metastasis of level Ib lymph node were identified based on the
analysis of the magnetic resonance imaging (MRI)/computed
tomography (CT) images from a large sample of 1,145 cases in the
training set. Subsequently, a score model was built according to
those independent risk factors. The model was used to separate the
patients into low- and high-risk groups. In the validating set, 43
low-risk and 42 high-risk patients underwent a pathological biopsy
of the level Ib lymph nodes to validate the accuracy of the model.
A further 327 patients with a long-term outcome were included in
the prognosis-research set. The prognostic effects of level Ib
lymph node irradiation were assessed in low- and high-risk
patients.
Patients and methods
Patients
The study enrolled 1,557 patients with primary NPC.
All the patients were diagnosed and initially treated at the Sun
Yat-Sen University Cancer Center or the First Affiliated Hospital
of Guangzhou Medical University (Guangdong, China). All the
patients underwent CT/MRI scans of the nasopharynx prior to
radiotherapy.
Of those patients, 1,145 cases were included in the
training set. The training set comprised of two patient groups. One
group of 933 patients was randomly selected from 6,519 hospitalized
patients at the Sun Yat-Sen University Cancer Center between
January 1990 and December 1999. The 212 patients of the second
group were from a clinical trial by the National High Technology
Research and Development Program 863 (2006AA02Z4B4) and treated by
Dr Y.F. Xia between January 2004 and April 2010.
A total of 85 patients were included in the
validation set. All the patients consented to a biopsy in level Ib
lymph nodes prior to radiotherapy. The pathological biopsy of the
level Ib lymph node was obtained between April 2003 and February
2011 in the Sun Yat-Sen University Cancer Center or The First
Affiliated Hospital of Guangzhou Medical University.
In the prognostic-research set, all the patients who
underwent 3D radiotherapy between November 2001 and November 2004
in the Sun Yat-Sen University Cancer Center were investigated.
There were 335 patients who had complete follow-up data and no
distance metastasis prior to the treatment. In the practical work,
the level Ib lymph nodes that fulfilled the radiographic standard
of metastasis were recognized as requiring irradiation. However,
the small lymph nodes that did not fulfill the standard were of
more concern. Therefore, eight patients were excluded, as they
fulfilled the radiographic standard of level Ib lymph nodes
metastasis. There were 327 patients remaining in the
prognostic-research set. No overlap existed among the training,
validation and prognostic-research sets.
Tumor-node-metastasis stage
The tumors were staged using the 7th edition of the
Union for International Cancer Control/American Joint Commission on
Cancer stage manual in all the patients (19).
Metastatic criteria of the level Ib lymph
node
The radiographic diagnostic criteria for the
metastasis of the level Ib lymph node followed the standard of van
den Brekel et al (20), as:
i) Lymph nodes with a minimal axial diameter >10 mm; ii) groups
of three or more borderline lymph nodes with a minimal axial
diameter of 8 mm; and iii) nodes with a central necrosis or a rim
of enhancement.
Biopsy of the level Ib lymph node
The methods for the biopsy of level Ib lymph nodes
included ultrasound-guided core and excisional biopsies. Excisional
biopsy was used in 39 patients who were willing to undergo
SMG-transfer surgery prior to radiotherapy. All the level Ib lymph
nodes of the 39 patients were removed for pathological examination.
Ultrasound-guided core biopsy was used in 46 patients. In those
patients, at least one level Ib lymph node (diameter >6 mm) was
examined. No less than two tissue specimens were obtained in each
examined lymph node.
Treatment
All the patients were irradiated using an
accelerator producing 6–8 MV X-rays. The primary tumor was
irradiated with a dose of 66–70 Gy. Additional radiotherapy boosts
of 8–12 Gy were administered following the delivery of the standard
dose for residual tumors or if the skull base was involved. The
neck received 50–70 Gy, depending on the lymph node involvement.
The radiotherapy techniques consisted of opposing lateral
faciocervical fields to cover the nasopharynx and upper cervical
lymphatic drainage region, with one low anterior cervical field to
cover the lower cervical region. Following 36–40 Gy, opposing
lateral preauricular fields were used for the primary tumor, and
anterior split-neck fields were used for the cervical region. When
the nasal cavity was involved, a supplementary anterior facial
field was added.
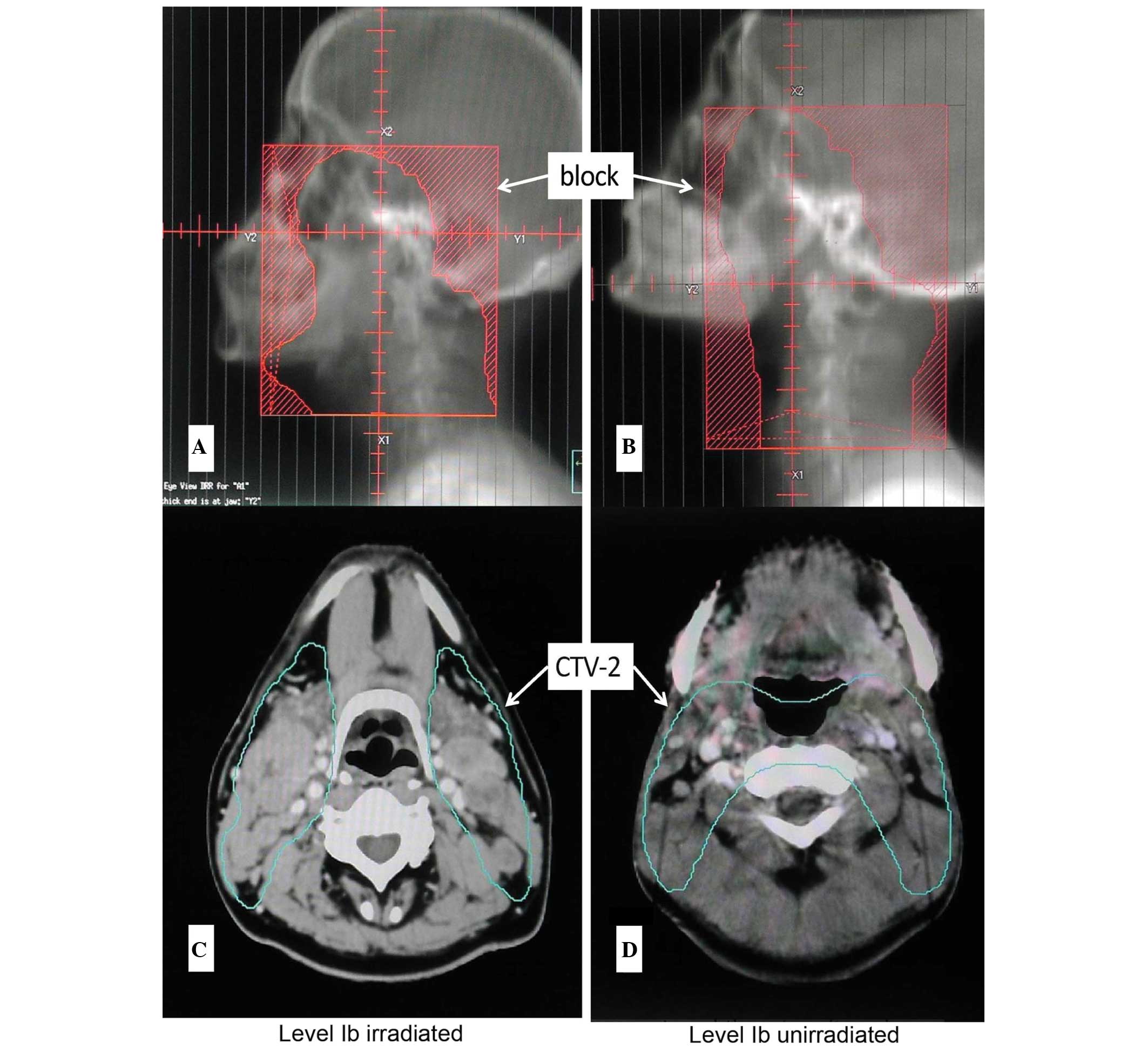
Irradiation of level Ib lymph node
In the prognostic-research set, 327 patients
underwent 3D radiotherapy. The CTV2 of 180 patients covered all the
visible lymph nodes of level Ib (the front line included
prevascular lymph nodes). The prescribed dose of CTV2 was 50 Gy.
The CTV2 of another 147 patients did not cover all the visible
level Ib lymph nodes (Fig. 1).
Follow-up
The patients were followed up by phone calls,
letters or outpatient reviews at least once a year. The follow-up
time was calculated from the start date of radiotherapy and ceased
on 31 December 2012.
Statistical analysis
Statistical analysis was performed using the SPSS
16.0 package (SPCC, Inc., Chicago, IL, USA). In the training set,
the occurrence of level Ib lymph nodes metastasis as a binary
outcome was analyzed by multivariate binary logistic regression,
considering 10 explanatory variables. The multivariated logistic
regression included the factors associated with level Ib lymph node
metastasis, either by significance in univariate analysis or by
clinical experience. A reduced model was obtained by a backward
stepwise selection procedure with the stay criterion set at 0.10.
The part and partial correlations and collinearity diagnostics were
used to test for collinearity. The tolerance <0.1, or variance
inflation factor >2, were considered problematic. The adequacy
of the logistic regression models was assessed using the Hosmer and
Lemeshow goodness-of-fit test. The regression coefficient of each
independent variable was subsequently modified into an integer
numerical value to simplify the computation (21).
In the prognostic-research set, the Kaplan-Meier
plots and the log-rank test were used to estimate the OS, the
locoregional recurrence rate (LRR) and the distant metastatic rate
(DMR) for all the 327 patients. The multivariable Cox
proportional-hazards model analysis was conducted to determine
whether the association between level Ib irradiation and
post-treatment outcomes was independent of other known prognostic
factors. The age, gender, chemotherapy, T stage and N stage were
assessed and entered in a backward stepwise Cox
proportional-hazards model to identify the predictors of the
clinical outcomes. The level of significance chosen was 0.05. The
hazard ratios in the prognostic research were used to calculate the
relative risk of recurrence or distance metastasis. Those
calculations were based on the Pike estimate, using the observed
and expected numbers of events, as calculated in the log-rank test
statistic; 95% confidence intervals used variances derived from the
information matrix.
The proportions were compared using Fisher’s exact
test and P<0.05 was considered to indicate a statistically
significant difference. All the reported P-values were
two-sided.
Results
Clinicopathological characteristics
The characteristics of the 1,145 patients in the
training set and 85 patients in the validating set are described in
Table I.
 | Table IClinicopathological characteristics in
the training and validating sets. |
Table I
Clinicopathological characteristics in
the training and validating sets.
| Training set | Validating set |
|---|
|
|
|
|---|
| Characteristic | n=1145 | % | n=85 | % |
|---|
| Age |
| ≤45 years | 590 | 51.5 | 48 | 56.5 |
| >45 years | 555 | 48.5 | 37 | 43.5 |
| Gender |
| Male | 864 | 75.5 | 65 | 76.5 |
| Female | 281 | 24.5 | 20 | 23.5 |
| Histology |
| WHO I | 10 | 0.9 | 1 | 1.2 |
| WHO II/III | 1135 | 99.1 | 84 | 98.8 |
| Clinical stage
(UICC) |
| I | 82 | 7.2 | 4 | 4.7 |
| II | 437 | 38.2 | 22 | 25.9 |
| III | 362 | 31.6 | 33 | 38.8 |
| IV | 264 | 23.1 | 26 | 30.6 |
| T classification |
| T1 | 251 | 21.9 | 8 | 9.4 |
| T2 | 466 | 40.7 | 26 | 30.6 |
| T3 | 227 | 19.8 | 34 | 40.0 |
| T4 | 201 | 17.6 | 17 | 20.0 |
| N classification |
| N0 | 317 | 27.7 | 20 | 23.5 |
| N1 | 533 | 46.6 | 26 | 30.6 |
| N2 | 207 | 18.1 | 26 | 30.6 |
| N3 | 88 | 7.7 | 13 | 15.3 |
Construction of score model in the
training set
Identification for metastatic risk
factors of level Ib lymph node
In the training set, the metastatic rate of the
level Ib lymph node was 5.9% (67/1,145). Univariate and
multivariate analyses were used to identify the association between
the clinical factors and level Ib metastasis (Table II). In total, 10 explanatory
variables were considered. The multivariate logistic regression
included the factors associated with level Ib lymph node metastasis
either by significance in univariate analysis or by clinical
experience. Those factors included: Age, gender, pathology [type
World Health Organization (WHO) I vs. type WHO II/III], T stage, N
stage, nasal cavity involvement, maxillary sinus involvement,
carotid sheath involvement, neck lymph node level involvement
(uninvolved vs. level II/III involved vs. level IV involved) and
maximum neck lymph node diameter of >20 vs. <20 mm. The age
was dichotomized at the median value of 45 years. The test for
collinearity indicated that N stage was problematic, and therefore
it was excluded. The multivariated logistic regression indicated
that the carotid sheath involvement, maximal diameter of the neck
lymph node (≥20 mm) and involvement of level II/III/IV lymph nodes
were three independent risk factors that were significantly
associated with the metastasis of level Ib lymph node.
| Table IIUnivariate and multivariate analysis
for the clinical predictors of level Ib metastasis. |
Table II
Univariate and multivariate analysis
for the clinical predictors of level Ib metastasis.
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|---|
| Characteristic | Level Ib metastasis
(−) | Level Ib metastasis
(+) | P-value | Hazard ratio | 95% confidence
interval | P-value |
|---|
| Age |
| ≤45 years | 557 | 33 | 0.708 | - | - | - |
| >45 years | 521 | 34 | | | | |
| Gender |
| Male | 809 | 55 | 0.241 | 0.630 | 0.322–1.232 | 0.177 |
| Female | 269 | 12 | | | | |
| Histology |
| WHO I | 10 | 0 | 1.000 | - | - | - |
| WHO II/III | 1068 | 67 | | | | |
| T stage |
| T1 | 240 | 11 | 0.240 | 0.813 | 0.580–1.139 | 0.229 |
| T2 | 436 | 30 | | | | |
| T3 | 209 | 18 | | | | |
| T4 | 193 | 8 | | | | |
| N stage |
| N0 | 317 | 0 | <0.001a | - | - | - |
| N1 | 506 | 27 | | | | |
| N2 | 184 | 23 | | | | |
| N3 | 71 | 17 | | | | |
| Nasal cavity
involvement |
| No | 866 | 52 | 0.635 | 1.288 | 0.665–2.495 | 0.453 |
| Yes | 212 | 15 | | | | |
| Maxillary sinus
involvement |
| No | 1033 | 45 | 0.515 | 0.420 | 0.049–3.623 | 0.430 |
| Yes | 66 | 1 | | | | |
| Carotid sheath
involvement |
| No | 544 | 20 | 0.001a | 2.106 | 1.204–3.682 | 0.009a |
| Yes | 534 | 47 | | | | |
| Neck lymph node
level involvement |
| No | 327 | 0 | <0.001a | 6.965 | 3.866–12.548 | <0.001a |
| Level II/III | 708 | 49 | | | | |
| Level IV | 43 | 18 | | | | |
| Maximum neck lymph
node diameter |
| <20 mm | 449 | 6 | <0.001a | 2.212 | 0.907–5.394 | 0.081a |
| ≥20 mm | 629 | 61 | | | | |
Risk score model for the metastasis of
level Ib lymph node
To create a systemic and feasible score model in a
clinical practice, an integral score derived from the n value for
each risk factor was assigned. The n value was calculated by the
regression coefficients of each independent risk factor: n=1n odds
ratio (OR) (21). When the risk
factor was absent, a score of 0 was recorded, and 1 was recorded
when there was carotid sheath involvement, maximal diameter of neck
lymph node (≥20 mm) or involvement of level II/III lymph nodes. If
a level IV lymph node was involved, a score of 2 was recorded
(Table III). The total scores
were calculated by collating all the scores of all three risk
factors. This indicated that patients with total scores of 0–1 had
a low-metastatic rate of level Ib lymph node (0.5%). However, the
patients with total scores of 2–4 had a much higher metastatic rate
of level Ib lymph node (8.5%). Therefore, the patients with total
scores of 0–1 were identified as low-risk patients, and the
patients with total scores of 2–4 were identified as high-risk
patients. The statistical difference of the level Ib metastatic
rate between the two groups was significant (P<0.001) (Table III).
| Table IIICalculation of the risk score and
risk group. |
Table III
Calculation of the risk score and
risk group.
| Variable | n=1n OR | Score |
|---|
| Neck lymph node
level involvement |
| No | 1.940 | 0 |
| Level II/III | | 1 |
| Level IV | | 2 |
| Maximum neck lymph
node diameter |
| <20 mm | 0.794 | 0 |
| ≥20 mm | | 1 |
| Carotid sheath
involvement |
| No | 0.745 | 0 |
| Yes | | 1 |
|
| Risk group | Level Ib metastatic
rate, % | Total score |
|
| Low, n=381 | 0.5 | 0–1 |
| High, n=764 | 8.5 | 2–4 |
Test of score model in the validating
set
The level Ib lymph nodes in 85 patients were
pathologically examined. According to the score system established
by the aforementioned training set, 43 cases were classified as
low-risk and 42 cases as high-risk patients. Notably, the score
model accurately predicted the observed outcomes in the
pathological validating set. A total of 13 of the 85 patients had
the metastasis of level Ib lymph node. There was no metastasis of
the level Ib lymph node in the low-risk patients. However, in the
high-risk patients, there were 13 cases of level Ib lymph nodes
metastasis. The metastatic rate of level Ib lymph node was as high
as 31%. The statistical difference between the low- and high-risk
patients was significant.
Prognostic research
The prognostic effect of level Ib irradiation in
low- and high-risk patients was evaluated in another group of 327
cases. Those patients were followed-up for a mean of 58 months
(range, 4–93 months). Their clinical characteristics are shown in
Table IV.
| Table IVClinical characteristics of the 327
patients for the prognostic research. |
Table IV
Clinical characteristics of the 327
patients for the prognostic research.
| Low-risk patients,
n=137 | | High-risk patients,
n=190 | |
|---|
|
| |
| |
|---|
| Characteristic | Level Ib
unirradiated | Level Ib
irradiated | P-value | Level Ib
unirradiated | Level Ib
irradiated | P-value |
|---|
| Age |
| ≤45 | 38 | 31 | 0.395 | 40 | 54 | 0.658 |
| >45 | 32 | 36 | | 37 | 59 | |
| Gender |
| Male | 46 | 48 | 0.468 | 54 | 78 | 1.000 |
| Female | 24 | 19 | | 23 | 35 | |
| Clinical stage |
| I | 17 | 6 | 0.091 | 0 | 0 | 0.105 |
| II | 24 | 28 | | 23 | 21 | |
| III | 18 | 17 | | 30 | 60 | |
| IV | 11 | 16 | | 24 | 32 | |
| T
classification |
| T1 | 18 | 10 | 0.349 | 7 | 11 | 0.176 |
| T2 | 24 | 26 | | 36 | 36 | |
| T3 | 17 | 15 | | 19 | 42 | |
| T4 | 11 | 16 | | 15 | 24 | |
| N
classification |
| N0 | 53 | 41 | 0.101 | 0 | 0 | 0.028 |
| N1 | 15 | 19 | | 43 | 51 | |
| N2 | 2 | 7 | | 23 | 54 | |
| N3 | 0 | 0 | | 11 | 8 | |
| Chemotherapy |
| No | 47 | 44 | 0.859 | 19 | 39 | 0.199 |
| Yes | 23 | 23 | | 58 | 74 | |
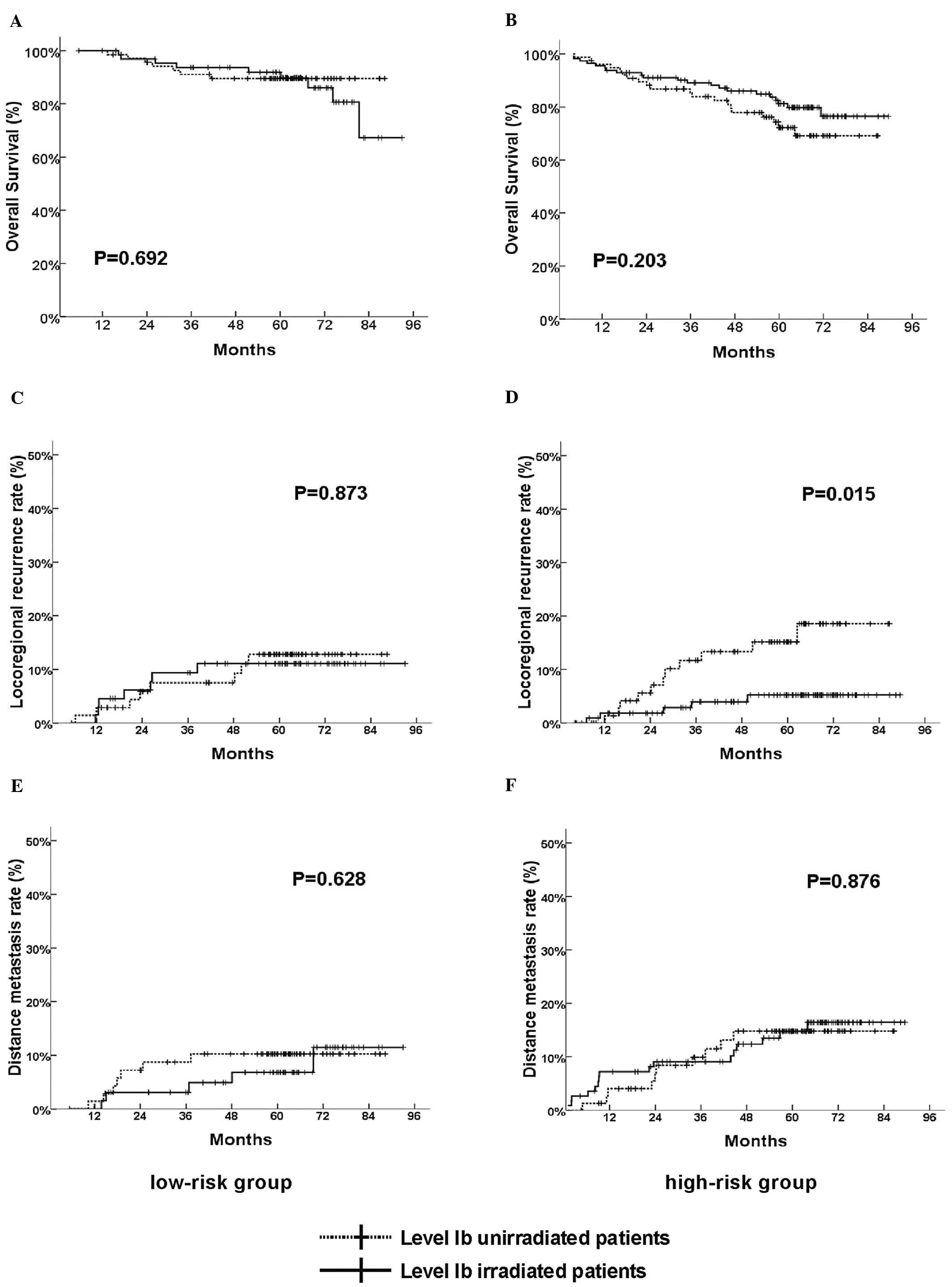
When the 327 patients were analyzed collectively,
the level Ib irradiation did not influence the OS, LRR and DMR
significantly (data not shown). Subsequently, further analysis was
conducted. Those patients were separated into low- (137 cases) and
high-risk patients (190 cases) according to the aforementioned
risk-score model. In the low-risk patients, level Ib irradiation
still had no significant influence on OS, LRR or DMR (Fig. 2A, C and E). In the high-risk
patients, unadjusted survival analysis revealed that LRR was
significantly low in level Ib-irradiated patients (Fig. 2D). The 5-year LRR in unirradiated
patients was 14.3%, however, in level Ib-irradiated patients it was
only 4.4%. Multivariate survival analysis included variants of T
stage, N stage, chemotherapy, gender and age, which indicated that
level Ib irradiation was the independent prognostic factor for LRR
in the high-risk group (Table V).
However, level Ib irradiation had no significance influence on OS
and DMR in the high-risk group (Fig.
2B and F).
| Table VMultivariate prognostic analysis of
the 190 high-risk patients in LRR and DMR. |
Table V
Multivariate prognostic analysis of
the 190 high-risk patients in LRR and DMR.
| LRR | DMR |
|---|
|
|
|
|---|
| Prognostic
factor | Relative risk (95%
CI) | P-value | Relative risk (95%
CI) | P-value |
|---|
| Age | 0.816
(0.303–2.196) | 0.686 | 1.112
(0.481–2.569) | 0.804 |
| Gender | 0.711
(0.229–2.210) | 0.556 | 0.711
(0.229–2.210) | 0.556 |
| Chemotherapy | 1.260
(0.396–4.006) | 0.696 | 1.525
(0.556–4.182) | 0.412 |
| T stage | 0.926
(0.539–1.591) | 0.781 | 0.940
(0.604–1.463) | 0.782 |
| N stage | 1.029
(0.466–2.273) | 0.944 | 2.332
(1.328–4.095) | 0.003 |
| Level Ib
irradiation | 0.291
(0.101–0.837) | 0.022 | 1.066
(0.478–2.378) | 0.875 |
Discussion
Based on the comprehensive analysis of the large
sample, the carotid sheath involvement, maximal diameter of neck
lymph node and involvement of neck level II/III/IV lymph node were
identified as the credible metastatic risk factors for level Ib
lymph nodes in primary NPC. These risk factors could be interpreted
by lymphotomy.
In general, the metastasis of lymph nodes in NPC is
characterized by systematic spreading down the neck along the deep
cervical lymph nodes (6,22). The level Ib lymph nodes are
superficial cervical lymph nodes and they drain the lymph from the
floor of the mouth, buccal mucosa, gingiva, face and anterior
region of the orbit and nasal cavity to the deep cervical lymph
nodes. Therefore, the tumor cells of NPC could not reach the level
Ib lymph nodes by direct lymph drainage. Lymphatic reflux caused by
blockage of the deep cervical lymph nodes could be the possible
reason for level Ib lymph nodes metastasis.
The first risk factor of carotid sheath involvement
is caused by the primary NPC invasion or metastasis of the
retropharyngeal nodes, which are usually difficult to identify by
CT images. The retropharyngeal lymph nodes are the first echo node
of the NPC (6,22), which is regarded as an indicator of
neck metastasis. Certain studies have indicated that carotid sheath
involvement is the transfer station for neck metastasis (23). In the present study, metastasis of
the level Ib lymph node was rarely found without carotid sheath
involvement. The second risk factor, maximum diameter of the neck
lymph nodes, was also significantly associated with level Ib lymph
nodes metastasis. The patients with ≤20 mm maximum diameter of neck
lymph nodes had the lower level Ib metastatic rate (only 1.3%).
When the maximum diameter of the neck lymph nodes was 20–39 mm, the
rate quickly reached 8.5%. However, the level Ib metastatic rate
moderately reached 9.4% when the maximum diameter of neck lymph
nodes was >40 mm. This indicated that the enlarged lymph nodes
could block the lymph drainage and generate reflux efficiently in
the 20 mm maximum diameter of those metastatic lymph nodes.
However, further enlargement of the lymph nodes could not
significantly increase the reflux. The third risk factor,
involvement of neck level II/III/IV lymph nodes, had a greater
role. This risk factor was closely and positively associated with
metastasis of the level Ib lymph nodes (24). When the level IV lymph node was
involved, the metastatic incidence of the level Ib lymph node
(18/61, 29.5%) was almost five times higher than the general
average (61/1,145, 5.3%). According to a comprehensive analysis of
the aforementioned results, when the carotid sheath was involved or
the neck lymph nodes were ≥20 mm, the reflux to level Ib may occur.
Additionally, the involved extension of the neck levels was the
most important risk factor for level Ib lymph nodes metastasis.
Other various factors, including nasal cavity and
maxillary sinus involvement, were previously considered to be
associated with level Ib metastasis. However, the present study
could not support those assumptions. For nasal cavity involvement,
it is possible that the tumor could spread to the level Ib lymph
nodes following the lymphatic drainage from the anterior one-third
of the nasal cavity. However, this situation was rarely clinically
observed as almost all the patients had been treated prior to the
occurrence. The maxillary sinus involvement was also observed, but
not associated with the metastasis of level Ib lymph nodes as the
lymph of the maxillary sinus drained to the nasopharynx without
direct linkage with the level Ib lymph node.
In the validation process, certain significant
identifications were of note. By comparing the pathological and
radiographic results of 85 patients, two noteworthy indications
were found. In the low-risk group, the radiographic and
pathological diagnoses were consistent in 41 out of 43 patients. In
the high-risk group, the CT/MR imaging only diagnosed 4 cases of
level Ib lymph node metastases in all 13 patients who were proved
by the pathological result. These results showed that the imagine
diagnosis of the level Ib lymph node metastasis was more credible
in the low-risk patients. This phenomenon may be generated by two
factors. Firstly, level Ib lymph nodes are the superficial lymph
node, and they drain lymphatic fluid from the oral and
maxillofacial, which are easy to inflame. Therefore, the level Ib
lymph nodes are often reactively enlarged due to the inflammation.
If the inflammatory lymph node is large enough to fulfill the
diagnostic standard in the CT/MR image, a false-positive diagnosis
occurs. Secondly, the metastasis of the lymph node is a continuous
process that begins with a single or a cluster of tumor cells
migrating into the lymph nodes, which may take months to grow large
enough to be detected by CT or MR (25). This second situation causes a
false-negative diagnose that usually occurs in high-risk
patients.
Subsequent to the construction and validation of the
risk model, it was assumed that: i) There was an extremely low risk
to omit irradiation in level Ib in low-risk patients due to the
small chance of metastasis; and ii) level Ib lymph node should be
irradiated in high-risk patients due to the relatively high
possibility of metastasis. Further studies on the prognosis could
also support this assumption. In the low-risk group, level Ib
irradiation had no significant effect on the prognosis. In the
high-risk group, level Ib unirradiation was an independent
prognostic factor of LRR.
In fact, the recurrence of the level Ib lymph nodes
may be the best indicator for evaluating the risk of level Ib
irradiation. In the present study, recurrences of the level Ib
lymph nodes were observed in five patients (pathological diagnosis
or minimal diameter >10 mm) of the 327 prognostic-research set
patients. However, four out of five cases were accompanied by
locoregional recurrence, possibly due to the tumor spreading to the
level Ib lymph nodes following nasopharynx or neck recurrence. Only
one case of level Ib lymph nodes metastasis occurred without
locoregional recurrence in a high-risk patient without level Ib
irradiation. This illustrates the importance of level Ib
irradiation in high-risk patients. However, the study had
particular limitations. First, the sample size of the validation
set was not large enough. Second, the study was entirely based on
clinical factors, which limited the ability to define the high-risk
patients more precisely.
In conclusion, the present study suggested a simple,
practical and appropriate score model to predict the metastasis
risk of level Ib lymph nodes. The factors included in the model
were easily available in clinical practice. The model may be a
valuable reference in CTV delineation of level Ib. More prospective
future clinical studies are required to verify the results of the
study.
References
|
1
|
Xia YF, Qian JY and Zhang EP: Practical
Radiotherapy for Nasopharyngeal Carcinoma. PeKing University
Medical Press; Beijing: pp. 86–87. 2003, (In Chinese).
|
|
2
|
Chen WZ, Gu BH, Chen HY, Gu ZY and Lin YG:
Analysis of the results of treatment and the cases of failure
following radiotherapy in 1083 cases of nasopharyngeal carcinoma.
Ai Zheng. 3:160–162. 1983.
|
|
3
|
Yi JL, Gao L, Huang XD, et al:
Nasopharyngeal carcinoma treated by radical radiotherapy alone:
Ten-year experience of a single institution. Int J Radiat Oncol
Biol Phys. 65:161–168. 2006.PubMed/NCBI
|
|
4
|
Su SF, Han F, Zhao C, et al: Treatment
outcomes for different subgroups of nasopharyngeal carcinoma
patients treated with intensity-modulated radiation therapy. Chin J
Cancer. 30:565–573. 2011. View Article : Google Scholar
|
|
5
|
Grégoire V, Levendag P, Ang KK, et al:
CT-based delineation of lymph node levels and related CTVs in the
node-negative neck: DAHANCA, EORTC, GORTEC, NCIC, RTOG consensus
guidelines. Radiother Oncol. 69:227–236. 2003.PubMed/NCBI
|
|
6
|
Sun Y, Ma J, Lu TX, Wang Y, Huang Y and
Tang LL: Regulation for distribution of metastatic cervical lymph
nodes of 512 cases of nasopharyngeal carcinoma. Ai Zheng. 23(11
Suppl): 1523–1527. 2004.(In Chinese).
|
|
7
|
Wang XS, Hu CS, Wu YR, Qiu XX and Feng Y:
Analysis of computed tomography-based distribution of metastatic
cervical nodes in 218 cases of nasopharyngeal carcinoma. Ai Zheng.
23:1056–1059. 2004.(In Chinese).
|
|
8
|
Luo DH, Zhou CW, Yao XS and Zhao YF: The
CT manifestations of the cervical lymph node metastasis of the
nasopharyngeal carcinoma. J Clin Radiol. 26:1199–1203. 2007.(in
Chinese).
|
|
9
|
Yeh SA, Tang Y, Lui CC, Huang YJ and Huang
EY: Treatment outcomes and late complications of 849 patients with
nasopharyngeal carcinoma treated with radiotherapy alone. Int J
Radiat Oncol Biol Phys. 62:672–679. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kuten A, Ben-Aryeh H, Berdicevsky I, et
al: Oral side effects of head and neck irradiation: correlation
between clinical manifestations and laboratory data. Int J Radiat
Oncol Biol Phys. 12:401–405. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jha N, Seikaly H, Harris J, et al:
Prevention of radiation induced xerostomia by surgical transfer of
submandibular salivary gland into the submental space. Radiother
Oncol. 66:283–289. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Al-Qahtani K, Hier MP, Sultanum K and
Black MJ: The role of submandibular salivary gland transfer in
preventing xerostomia in the chemoradiotherapy patient. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod. 101:753–756. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lee N, Xia P, Quivey JM, et al:
Intensity-modulated radiotherapy in the treatment of nasopharyngeal
carcinoma: an update of the UCSF experience. Int J Radiat Oncol
Biol Phys. 53:12–22. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kam MK, Teo PM, Chau RM, et al: Treatment
of nasopharyngeal carcinoma with intensity-modulated radiotherapy:
the Hong Kong experience. Int J Radiat Oncol Biol Phys.
60:1440–1450. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Liu WS, Kuo HC, Lin JC, et al: Assessment
of salivary function change in nasopharyngeal carcinoma treated by
parotid-sparing radiotherapy. Cancer J. 12:494–500. 2006.
View Article : Google Scholar
|
|
16
|
Kam MK, Leung SF, Zee B, et al:
Prospective randomized study of intensity-modulated radiotherapy on
salivary gland function in early-stage nasopharyngeal carcinoma
patients. J Clin Oncol. 25:4873–4879. 2007. View Article : Google Scholar
|
|
17
|
Tham IW, Hee SW, Yeo RM, et al: Treatment
of nasopharyngeal carcinoma using intensity-modulated
radiotherapy-the national cancer centre singapore experience. Int J
Radiat Oncol Biol Phys. 75:1481–1486. 2009. View Article : Google Scholar
|
|
18
|
Radiation Therapy Oncology Group. RTOG
0615 Protocol Information. http://www.rtog.org/ClinicalTrials/ProtocolTable/StudyDetails.aspx?study=0615.
Accessed February 2, 2011
|
|
19
|
International Union Against Cancer. TNM
Classification of Malignant Tumors. Sobin LH, Gospodarowicz MK and
Wittekind CH: 7th edition. Wiley & Sons, Inc; New York, NY:
2009
|
|
20
|
van den Brekel MW, Stel HV, Castelijns JA,
et al: Cervical lymph node metastasis: assessment of radiologic
criteria. Radiology. 177:379–384. 1990.PubMed/NCBI
|
|
21
|
Apfel CC, Läärä E, Koivuranta M, Greim CA
and Roewer N: A simplified risk score for predicting postoperative
nausea and vomiting: conclusions from cross-validations between two
centers. Anesthesiology. 91:693–700. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Pan WR, Suami H, Corlett RJ and Ashton MW:
Lymphatic drainage of the nasal fossae and nasopharynx: preliminary
anatomical and radiological study with clinical implications. Head
Neck. 31:52–57. 2009. View Article : Google Scholar
|
|
23
|
Zheng GL: Mode of spread in nasopharyngeal
carcinoma as seen on CT scan. Zhonghua Zhong Liu Za Zhi.
10:293–295. 1988.(In Chinese).
|
|
24
|
King AD, Ahuja AT, Leung SF, et al: Neck
node metastases from nasopharyngeal carcinoma: MR imaging of
patterns of disease. Head Neck. 22:275–281. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
van den Brekel MW, van der Waal I, Meijer
CJ, Freeman JL, Castelijns JA and Snow GB: The incidence of
micrometastases in neck dissection specimens obtained from elective
neck dissections. Laryngoscope. 106:987–991. 1996.PubMed/NCBI
|