Introduction
Since the early 1980s, endoscopic resection (ER)
techniques using electrothermal devices, such as polypectomy, strip
biopsy and endoscopic mucosal resection (EMR), have been developed
as diagnostic and curative procedures for gastrointestinal mucosal
lesions (1–6). The latest modality using specialized
electrosurgical knives, referred to as endoscopic submucosal
dissection (ESD), has enabled more complete removal of gastric
lesions and is currently accepted as a standard treatment of early
gastric adenocarcinoma (EGA) (6–8). The
precise histological assessment of ER specimens, such as
pathological diagnosis, the depth of cancerous invasion,
lymphovascular permeation and the status of the surgical margin, is
crucial for the subsequent management of the patients (1,3,4,6–9).
Therapeutic procedures using electrothermal devices may induce
varying artifacts disturbing the histological evaluation in
gastrointestinal and other specimens (1,3,4,9–14).
However, histological artifacts in newly developed ESD specimens
remain poorly understood. In this study, we histologically examined
ESD specimens focusing on artifactual nuclear changes and evaluated
their association with clinical findings.
Materials and methods
Materials
A total of 97 gastric ESD specimens from 79 patients
were retrieved from the surgical pathology files of the Department
of Pathology, Japan Self-Defense Forces Central Hospital, Tokyo,
Japan (2009–2012). Clinical information was available from the
patients’ charts. If necessary, the gross photographs of the ESD
specimens were also reviewed. A total of 18 patients had
metachronously undergone ESD (17, twice; 1, three times) and the
final diagnoses included 74 patients with adenocarcinoma (73
patients with EGA and 1 with advanced cancer), 14 with tubular
adenoma, 3 with carcinoid tumor and 6 with hyperplastic polyp of
the foveolar type. Using an electrical device, preoperative marking
was placed outside the gastric lesions in 95 specimens, 0–6 days
prior to ESD (mean, 1.74 days), once in 37 and twice in 58
specimens. In this study, we defined marking 1–6 days prior to ESD
as ‘previous marking’ and marking on the same day as ‘fresh
marking’; the former was performed in 76 specimens using an argon
plasma coagulator (APC; ERBE Elektromedizin GmbH, Tübingen,
Germany) and the latter was performed from 10 min to a few hours
prior to ESD. An APC was used in 69, flush knife in 5 and
precutting knife in 2 specimens. The 95 specimens with marking were
divided into 19 with fresh marking only, 19 with previous marking
only (including 1 with previous marking twice) and 57 with both
fresh and previous marking. The dissecting device was an
insulation-tipped (IT) knife (Olympus, Tokyo, Japan) with or
without other devices (precutting, flex and/or hook knives) in 82,
flush knife only in 14 and flex knife only in 1. Diathermic
hemostasis using Coagrasper™ (Olympus) was performed in 90
specimens. The procedure time of ESD ranged between 7 and 470 min
(mean, 91.4 min). For a control study, 79 gastrectomy specimens
from patients with gastric cancer who had no history of ESD were
retrieved from the surgical pathology files of the Department of
Pathology, Japan Self-Defense Forces Central Hospital (1997–2008)
and examined. The number of sections examined in each control case
ranged between 8 and 105 (mean, 22.3).
Methods
The ESD specimens were fixed in 15% buffered
formalin for 14–52 h and were completely cut at 3–4-mm intervals,
ranging in each case between 4 and 45 sections (mean, 13.4
sections). The sections (4–5 μm) were serially cut, stained with
hematoxylin and eosin and histologically examined. Selected
sections were immunostained with anti-p53 antibody (DO-7, Histofine
kit; Nichirei, Tokyo, Japan). The association of ESD artifacts with
clinical findings was analyzed using the Chi-square test, Fisher’s
exact test, unpaired t-test and Mann-Whitney U test. P<0.05 was
considered to indicate a statistically significant difference.
Results
Nuclear artifacts
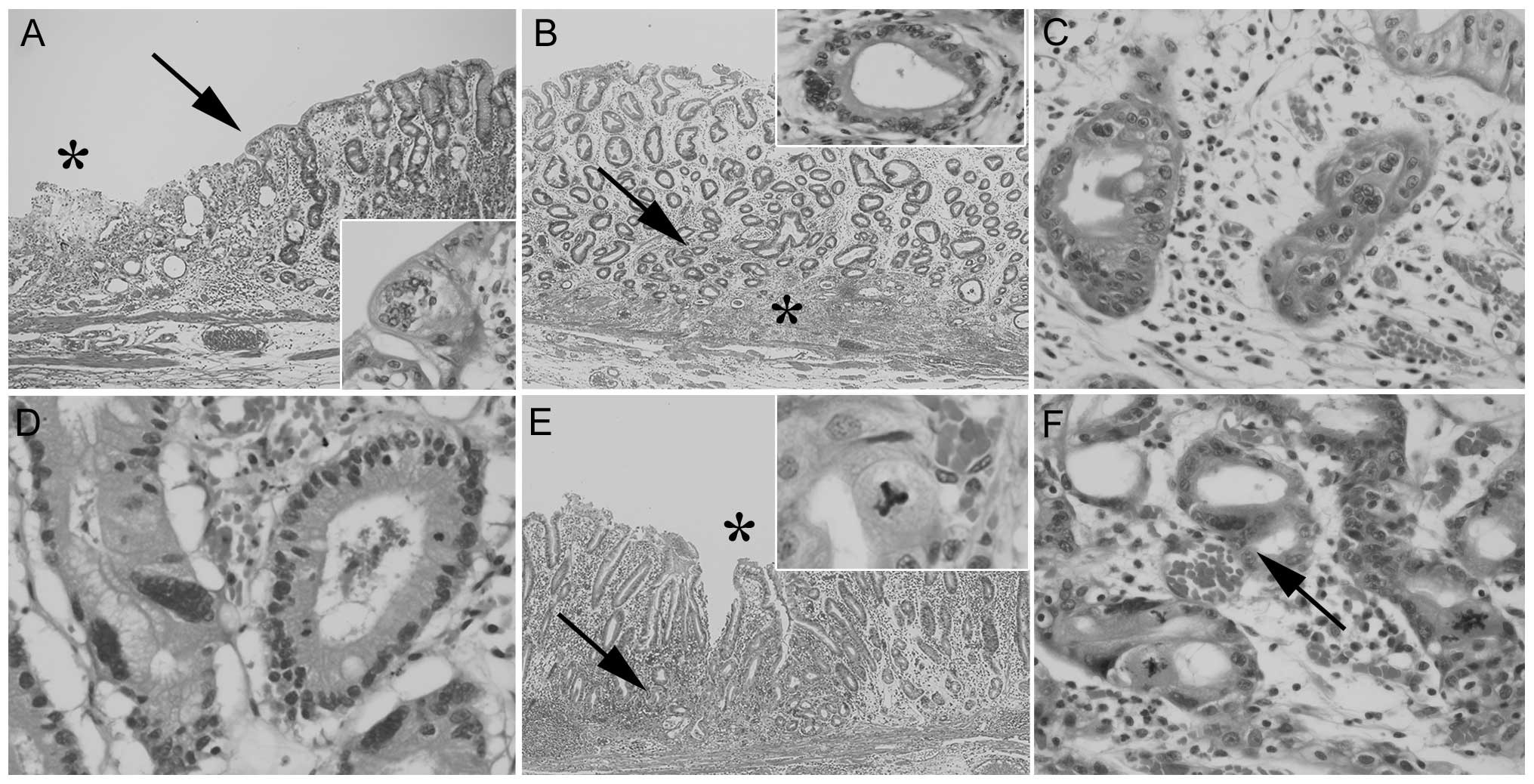
In 69 ESD specimens (71.1%), possible nuclear
artifacts were scattered in the peripheral portions near/beneath
preoperative marking-related erosive and/or coagulated lesions and
exhibited multinucleated figures (68 specimens, 70.1%; Fig. 1A–C) and atypical mitotic-like
figures (28 specimens, 28.9%). The former sometimes simulated
gigantic nuclei (Fig. 1D) and the
latter included a tripolar spindle-like configuration (8 specimens,
8.2%; Fig. 1E) and/or bizarre
asterisk or spindle figures (19 specimens, 19.9%; Fig. 1F). ‘Fresh’ and ‘previous’ marking
areas were not distinguished histologically. The patient sources
for each ESD specimen were 64 men and 5 women and the age at which
each ESD specimen was obtained ranged between 44 and 84 years
(mean, 60.9 years). The final diagnoses included 52 cases with EGA,
1 with advanced gastric cancer, 10 tubular adenomas, 4 hyperplastic
polyps and 2 carcinoid tumors. The ESD changes were mainly minute
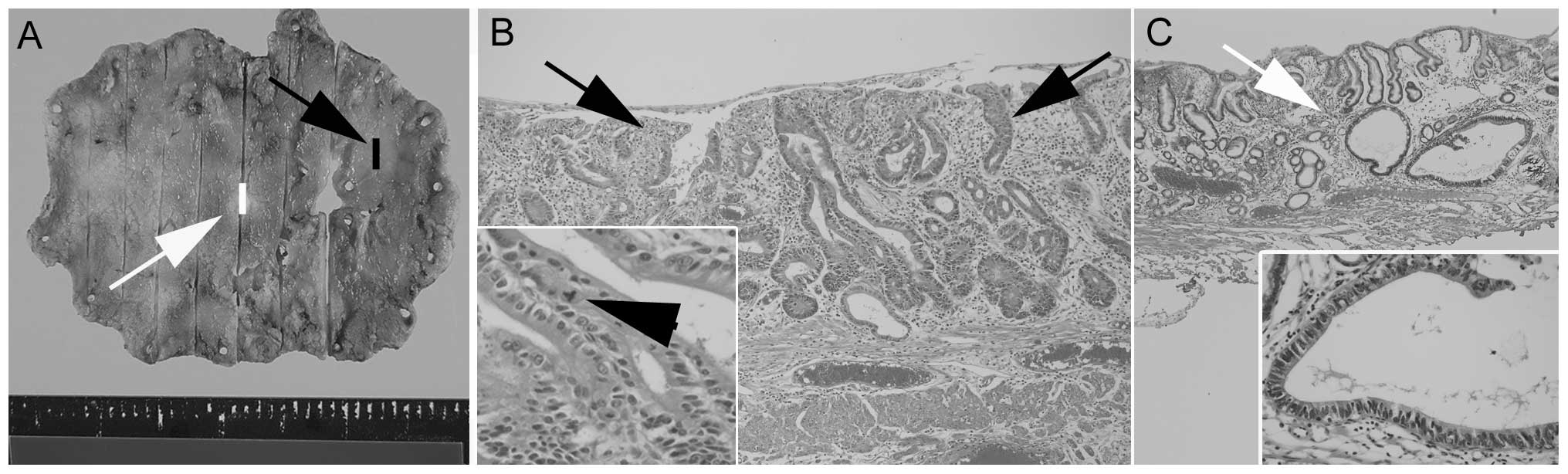
and the majority were easily recognizable as artifacts. In 13 cases
(13.4%), however, they mimicked dysplasia, as they were focally
aggregated concomitant with cribriform-like structures, nuclear
enlargement, nuclear hyperchromatism and/or an irregular nuclear
arrangement. In 1 case, the artifacts were initially misdiagnosed
as adenocarcinoma (Fig. 2).
However, in the deep cut sections, the dysplastic nature tended to
disappear and sometimes other degenerative findings became more
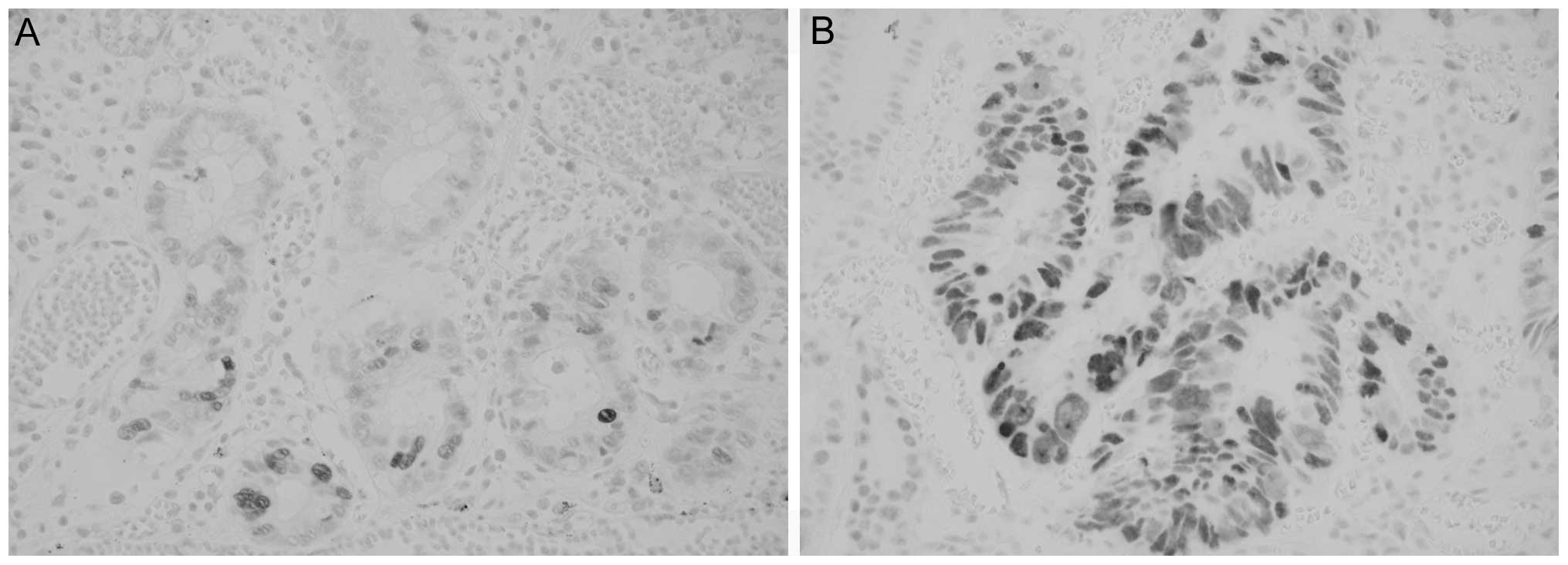
prominent. In 11 of the 12 cases examined (91.7%), scattered
nuclear p53 positivity was detected in dysplasia-like artifacts
(Fig. 3A). However, this staining
pattern was different from diffusely p53-positive adenocarcinoma
cells (Fig. 3B), which were found
in 6 of the 8 EGAs examined. As a control study of ESD artifacts,
we selected 69 age- and gender-matched control cases comprising 64
men and 5 women, with a mean age of 60.9 years (range, 44–84 years)
selected from 79 gastrectomy cases without ESD. Similar nuclear
artifacts were not identified in these gastrectomy specimens.
Association of ESD artifacts with
clinical findings
The association between ESD artifacts and clinical
findings was analyzed in each ESD specimen and is summarized in
Tables I and II. Multinucleated figures were
associated with larger-sized ESD specimens (P=0.003), presence of
previous marking (P<0.001) and higher frequency of marking
(P<0.001), but not with age at ESD, number of ESD specimens in
individual patients, ESD procedure time, previous vs. fresh
marking, the device used in fresh marking (APC vs. non-APC), the
dissecting device (IT vs. non-IT knife), or diathermic hemostasis.
Atypical mitotic-like figures were associated with previous
(P=0.002) as well as fresh marking (P=0.007), but not with other
findings. Dysplasia-like artifacts were associated with older age
(P=0.031), but not with other findings.
 | Table IAssociations of artifactual nuclear
changes in ESD specimens with clinical findings. |
Table I
Associations of artifactual nuclear
changes in ESD specimens with clinical findings.
| Variables | Multinucleated
figures (+)(n=68) | Multinucleated
figures (−) (n=29) | P-value | Atypical mitotic-like
figures (+)(n=28) | Atypical mitotic-like
figures (−) (n=69) | P-value |
|---|
| Age at ESDa, years Mean (range) | 60.9 (44–84) | 59.5 (40–84) | 0.779 | 60.4 (46–84) | 60.6 (40–81) | 0.954 |
| Size of ESD
specimens, cm Mean (range) | 3.9 (1.2–9.0) | 3.1 (1.4–5.6) | 0.003 | 3.4 (1.2–5.4) | 3.8 (1.4–9.0) | 0.321 |
| Procedure time of
ESD, min Mean (range) | 94.3 (15–470) | 85.5 (7–250) | 0.381 | 75.9 (15–470) | 97.7 (15–470) | 0.199 |
| Preoperative marking
+/− | 68/0 | 27/2 | 0.159 | 28/0 | 67/2 | 0.729 |
| Previousb marking +/− | 66/2 | 10/19 | <0.001 | 28/0 | 48/21 | 0.002 |
| Freshc marking +/− | 50/16 | 26/3 | 0.135 | 17/11 | 59/10 | 0.007 |
| Used device in fresh
marking APC/non-APCd | 44/6 (n=50) | 25/1 (n=26) | 0.454 | 15/2 (n=17) | 54/5 (n=59) | 0.950 |
| Frequency of marking
Mean (range) | 1.7 (1–2) | 1.24 (0–2) | <0.001 | 1.6 (1–2) | 1.6 (1–2) | 0.965 |
| Used electrical knife
IT/non-ITe | 57/11 | 25/4 | 0.992 | 25/3 | 48/21 | 0.075 |
| Diathermic
hemostasisf +/− | 61/7 | 29/0 | 0.172 | 24/4 | 66/3 | 0.200 |
| Table IIAssociation of dysplasia-like
artifacts in ESD specimens with clinical findings. |
Table II
Association of dysplasia-like
artifacts in ESD specimens with clinical findings.
| Variables | Dysplasia-like
artifacts (+) (n=13) | Dysplasia-like
artifacts (−) (n=84) | P-value |
|---|
| Mean age at
ESDa, years (range) | 66.9 (50–84) | 59.5 (40–81) | 0.031 |
| Mean size of ESD
specimens, cm (range) | 4.1 (2.5–7.6) | 3.6 (1.2–9) | 0.254 |
| Mean procedure time
of ESD, minutes (range) | 89.8 (46–204) | 91.6 (7–470) | 0.935 |
| Preoperative marking
+/− | 13/0 | 83/1 | 0.280 |
| Previousb marking +/− | 12/1 | 64/20 | 0.342 |
| Freshc marking +/− | 10/3 | 66/18 | 0.820 |
| Used device in fresh
marking, APC/non-APCd | 9/1 (n=10) | 60/6 (n=66) | 0.621 |
| Mean frequency of
marking, (range) | 1.7 (1–2) | 1.6 (0–2) | 0.409 |
| Used electrical
knife, IT/non-ITe only | 10/3 | 72/12 | 0.686 |
| Diathermic
hemostasisf +/− | 13/0 | 77/7 | 0.612 |
Patient outcome
Of the 62 patients with nuclear artifacts, 2 died
from other causes (1 from pulmonary fibrosis and 1 from heatstroke)
≥2 years after ESD. The remaining 60 patients were alive, with a
mean follow-up period of 30.3 months (range, 4–53 months), although
3 underwent additional gastrectomy due to positive submucosal
margins (2 patients) and multiple carcinoid tumors (1 patient). No
patients exhibited recurrent cancerous growth adjacent to the
post-ESD sites.
Discussion
In this study, we observed unique multinucleated
and/or atypical mitotic-like figures in 71% of the ESD specimens.
These figures were not found in age- and gender-matched control
gastrectomy specimens, suggesting that the artifacts were
ESD-related. Regarding ER/ESD-related gastrointestinal changes,
previous studies emphasized that the artifacts disturbed
histological diagnosis and assessment of marginal status (1,3,4,9,10,12),
but did not focus on the nuclear changes. To the best of our
knowledge, the present study is the first to describe ESD-related
nuclear artifacts in detail. Nuclear artifacts were found close to
marking-related erosive and/or depressed coagulation, corresponding
to thermal artifacts, also called electrothermal, diathermic, or
cautery-related changes (1,3,4,9–11).
Therefore, nuclear artifacts themselves would have contributed to
the thermal artifacts. By examining 1 section only, the associated
marking-related thermal changes may be unclear. However, we believe
that further examination of the next adjacent and/or deep cut
sections and comparative observation with the gross photographs of
the ESD specimens may reveal the distinct marking points close to
the nuclear changes.
The multinucleated artifacts partly resembled
previously described multinucleated cells in esophageal and
colorectal biopsy specimens without use of electrothermal devices,
which may represent a non-specific, regenerative or degenerative
response to injury (15,16). The incidence of such artifacts has
been considered rare (15,16), whereas multinucleated artifacts
were identified in 70% of our ESD specimens. These findings suggest
that the ESD procedure frequently evokes fundamentally rare,
degenerative or regenerative multinucleated changes of gastric
mucosal cells.
Multinucleated figures were statistically associated
with ESD specimen size, frequency of marking and ‘previous’
marking, but not with ‘fresh’ marking. Larger ESD specimens may be
correlated with a higher frequency of marking. Hence, these
findings indicate that multinucleated artifacts are closely
associated with frequent thermal injury and subsequent
degeneration. However, atypical mitotic-like artifacts were
associated with ‘previous’ as well as ‘fresh’ marking history, but
not with the size of ESD specimens or the frequency of marking,
denoting the effect of both super-acute destruction and reactive
regenerative changes. There may be certain differences in the
pathogenesis between these artifacts. Both characteristics were not
associated with the number of ESD in the same patient, suggesting
that their development may not be associated with the individual
vulnerability of each patient.
ESD-related nuclear changes may infrequently mimick
dysplasia due to concomitant nuclear enlargement, overlapping, or
hyperchromatism and structural abnormality, which have been
mentioned in gastric post-EMR biopsy sites (5) and electrical device-related
extragastrointestinal specimens (10,13,14).
Moreover, in our experience, ESD-related artifacts may be
misdiagnosed as adenocarcinoma. Therefore, these artifacts should
be distinguished from true neoplasia and dysplasia. Our results
suggested the usefulness of further conventional examinations,
including histological examination of a deep cut and/or the
adjacent section and careful comparison with gross ESD photographs,
on the basis of anatomical and histological characteristics of
ESD-related artifacts.
The present immunohistochemical study demonstrated a
high incidence of p53 positivity in dysplasia-like artifacts (92%
of cases examined), although the staining pattern was scattered and
differed from the diffuse p53-positive pattern of adenocarcinoma,
which was found in 75% of the EGAs examined. Hibi et al
(17) reported scattered
p53-positive nuclei in gastric mucosa with persistent
Helicobacter pylori infection and suggested that this type
of gastritis may induce DNA damage, resulting in nuclear
accumulation of wild-type p53 protein. We believe that ESD may
induce similar DNA damage, contributing to scattered p53
accumulation in dysplasia-like artifacts.
In conclusion, we described ESD-related multinuclear
and atypical mitotic-like artifacts, which, in older patients, may
be reminiscent of dysplasia. Further conventional examinations
focusing on histological characteristics and favored location of
such artifacts may prove useful for discrimination from true
dysplasia or cancer.
Acknowledgements
The authors would like to thank Kenji Okada for
excellent technical assistance and Daniel Mrozek for editing the
manuscript.
References
|
1
|
Cooper HS, Deppisch LM, Kahn EI, et al:
Pathology of the malignant colorectal polyp. Hum Pathol. 29:15–26.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Matsukuma S, Goda K, Sakai Y, Ikegawa K,
Morita D and Kuwabara N: Histopathologic studies of colorectal
postendoscopic resection sites: ‘skipping electrothermal injury’
associated with endoscopic resection procedures. Am J Surg Pathol.
23:459–464. 1999.PubMed/NCBI
|
|
3
|
Lauwers GY, Ban S, Mino M, et al:
Endoscopic mucosal resection for gastric epithelial neoplasms: a
study of 39 cases with emphasis on the evaluation of specimens and
recommendations for optimal pathologic analysis. Mod Pathol.
17:2–8. 2004. View Article : Google Scholar
|
|
4
|
Hull MJ, Mino-Kenudson M, Nishioka NS, et
al: Endoscopic mucosal resection: an improved diagnostic procedure
for early gastroesophageal epithelial neoplasms. Am J Surg Pathol.
30:114–118. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mitsuhashi T, Lauwers GY, Ban S, et al:
Post-gastric endoscopic mucosal resection surveillance biopsies:
evaluation of mucosal changes and recognition of potential mimics
of residual adenocarcinoma. Am J Surg Pathol. 30:650–656. 2006.
View Article : Google Scholar
|
|
6
|
Kim SG: Endoscopic treatment for early
gastric cancer. J Gastric Cancer. 11:146–154. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ono H: Early gastric cancer: diagnosis,
pathology, treatment techniques and treatment outcomes. Eur J
Gastroenterol Hepatol. 18:863–866. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kakushima N, Ono H, Tanaka M, Takizawa K,
Yamaguchi Y and Matsubayashi H: Factors related to lateral margin
positivity for cancer in gastric specimens of endoscopic submucosal
dissection. Dig Endosc. 23:227–232. 2011. View Article : Google Scholar
|
|
9
|
Tanabe H, Iwashita A, Haraoka S, et al:
Pathological evaluation concerning curability of endoscopic
submucosal dissection (ESD) of early gastric cancer including
lesions with obscure margins. Stomach Intestine. 41:53–66. 2006.(In
Japanese).
|
|
10
|
Fechner RE: The surgical pathology of
iatrogenic lesions. Principles and Practice of Surgical Pathology.
Silverberg SG: 1. Churchill Livingstone; New York, NY: pp. 77–99.
1988
|
|
11
|
Goldstein NS, Watts JC, Neill JS, et al:
The effect of electrothermal cautery-assisted resection of
diminutive colonic polyps on histopathologic diagnosis. Am J Clin
Pathol. 115:356–361. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dahl J and Greenson JK: Colon. Histology
for Pathologists. Mills SE: 4th edition. Lippincott Williams &
Wilkins; Philadelphia PA: pp. 673–695. 2012
|
|
13
|
Gan E, Costello A, Slavin J and Stillwall
RG: Pitfalls in the diagnosis of prostate adenocarcinoma from
holmium resection of the prostate. Tech Urol. 6:185–188.
2000.PubMed/NCBI
|
|
14
|
Clarke B and McCluggage WG: Iatrogenic
lesions and artefacts in gynaecological pathology. J Clin Pathol.
62:104–112. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Singh SP and Odze RD: Multinucleated
epithelial giant cell changes in esophagitis: a clinicopathologic
study of 14 cases. Am J Surg Pathol. 22:93–99. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kambham N, Troxell M and Longacre TA:
Multinucleated epithelial giant cells in colorectal polyps: a
potential mimic of viropathic and/or dysplastic changes. Am J Surg
Pathol. 29:912–919. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hibi K, Mitomi H, Koizumi W, Tanabe S,
Saigenji K and Okayasu I: Enhanced cellular proliferation and p53
accumulation in gastric mucosa chronically infected with
Helicobacter pylori. Am J Clin Pathol. 108:26–34.
1997.PubMed/NCBI
|