Introduction
Despite the improvements in the early detection of
gastric cancer (GC), it remains one of the leading causes of
cancer-related mortality worldwide (1, 2).
Surgical resection is generally recommended as standard treatment
for curable GC. Furthermore, systemic chemotherapy is widely
accepted as palliative treatment for patients with unresectable,
advanced or recurrent GC and was shown to improve the quality of
life and prolong survival time. Previous studies have indicated the
superiority of systemic chemotherapy compared to best supportive
care (BSC) in patients with advanced or recurrent GC (3–5) and
several phase III trials investigating systemic chemotherapy in
advanced GC patients have been conducted (6–11).
Recently, several clinical trials assessed the tolerability or
efficacy of systemic chemotherapy, including adjuvant chemotherapy,
in geriatric patients with advanced or recurrent GC and
demonstrated its feasibility (12–17).
However, the effect of systemic chemotherapy in the prognosis of
geriatric patients with advanced or recurrent GC remains unclear.
In addition, standardized regimens have not been validated. It may
be difficult to standardize cancer treatments for geriatric
patients, as the ability to tolerate intensive chemotherapy is
largely dependent on the patient's physical background.
In the present study, we investigated
clinicopathological characteristics, including the presence of
concomitant illnesses, such as cardiorespiratory disease, in
geriatric patents with advanced or recurrent GC and evaluated the
prognostic significance of intensive chemotherapy. The results of
our study may affect decision making regarding treatment for
geriatric patients with advanced or recurrent GC.
Patients and methods
Patients
A total of 54 geriatric patients (aged ≥75 years)
with histologically confirmed advanced or recurrent adenocarcinoma
of the stomach or gastroesophageal junction were enrolled in this
study. The patients were treated at Kyoto Prefectural University of
Medicine (Kyoto, Japan) between 2002 and 2010. We retrospectively
reviewed the hospital data and evaluated the clinicopathological
characteristics, such as age at diagnosis, gender, tumor stage,
comorbidities and chemotherapeutic regimens. We also collected
follow-up data on tumor recurrence and prognosis up to December 31,
2012.
Statistical analysis
A univariate analysis of the correlation between
clinicopathological characteristics and the administration of
chemotherapy was performed using the Chi-square and Fisher's exact
probability tests. Multivariate logistic regression was used to
assess the factors associated with the administration of
chemotherapy. Kaplan-Meier survival curves were generated and
compared with log-rank tests to assess the survival benefits
between the patient treatment groups. The prognostic factors for
overall survival were evaluated using the Cox proportional hazards
regression. For all analyses, P-value <0.05 was considered to
indicate statistically significant differences. Statistical
analyses were conducted using JMP 10 software (SAS Institute Inc.,
Cary, NC).
Results
Clinicopathological characteristics of
gastric cancer patients
A total of 54 geriatric patients were included in
this study. The patients were staged as follows: stage I, 1
patient; stage II, 17 patients; stage III, 22 patients; and stage
IV, 14 patients, according to the 7th TNM classification (18). Tumor staging was performed at
initial diagnosis. The mean age of the patients was 79.8 years
(range: 75–89 years). Of the 54 patients, 47 (87%) underwent
gastrectomy and regional lymphadenectomy, whereas 7 (13%) were
ineligible for gastrectomy. A total of 31 patients (57%) received
systemic chemotherapy and the remaining 23 (43%) did not receive
chemotherapy (Table I).
 | Table ICharacteristics of geriatric patients
with advanced or recurrent gastric cancer. |
Table I
Characteristics of geriatric patients
with advanced or recurrent gastric cancer.
| Characteristics | Patient no. (%)
(n=54) |
|---|
| Gender |
| Male | 37 | (69) |
|
Female | 17 | (31) |
| Age,
yearsa |
|
75–79 | 31 | (57) |
| >
80 | 23 | (43) |
| Tumor
depthb |
| T1 | 5 | (9) |
| T2 | 3 | (6) |
| T3 | 12 | (22) |
| T4 | 34 | (63) |
| Lymph node
metastasis |
|
Negative | 42 | (78) |
|
Positive | 12 | (22) |
| Distant
metastasis |
|
Negative | 40 | (74) |
|
Positive | 14 | (26) |
| Stagea, b |
| I | 1 | (2) |
| II | 17 | (31) |
| III | 22 | (41) |
| IV | 14 | (26) |
| Resectability |
|
Resectable | 47 | (87) |
|
Non-resectable | 7 | (13) |
| Recurrence
pattern |
|
Peritoneal | 19 | (35) |
|
Liver/lung | 10 | (19) |
| Lymph
node | 11 | (20) |
|
Local | 11 | (20) |
|
Others | 3 | (6) |
| Chemotherapy |
|
Absent | 23 | (43) |
|
Present | 31 | (57) |
Details of chemotherapeutic
regimens
Of the 31 patients who received chemotherapy, 27
(87%) were administered 5-fluorouracil (5-FU)-based regimens (S-1,
S-1 plus cisplatin, uracil-tegafur and 5-FU) as first-line
chemotherapy and the remaining 4 patients received taxane-based
regimens (3 patients) or irinotecan plus cisplatin (1 patient).
Furthermore, 12 patients received second-line chemotherapy, of whom
10 patients received 5-FU-based regimens (S-1 alone, 6 patients;
S-1 plus cisplatin, 2 patients; uracil-tegafur, 1 patient; and 5-FU
i.v., 1 patient).
Concomitant illnesses in geriatric
patients prior to treatment
Of the 54 included patients, 20 (37%) did not
experience any concomitant illness prior to treatment. However, the
remaining 34 patients (63%) exhibited concomitant illnesses,
including hypertension, cardiac disease, cerebrovascular disease,
diabetes mellitus, pulmonary disease and liver disease. In
particular, 20 patients (37%) had cardiorespiratory diseases, such
as atrial fibrillation, myocardial infarction, brain infarction and
pulmonary infarction. The patients with cardiorespiratory diseases
were receiving treatment for their conditions (e.g., antithrombotic
medication, antiarrhythmic agents, or home oxygen therapy)
(Table II).
| Table IIPretreatment classification of
comorbidity in geriatric patients with advanced or recurrent
gastric cancer. |
Table II
Pretreatment classification of
comorbidity in geriatric patients with advanced or recurrent
gastric cancer.
| Comorbidities | Patient no. (%)
(n=54) |
|---|
| Hypertension | 15 | (27) |
| Cardiac disease | 10 | (15) |
| Cerebrovascular
disease | 8 | (14) |
| Diabetes
mellitus | 5 | (9) |
| Pulmonary
disease | 3 | (5) |
| Liver disease | 2 | (3) |
| Cardiorespiratory
diseasea | 20 | (37) |
Correlation of clinicopathological
factors with chemotherapy administration and logistic regression
analysis of independent factors associated with chemotherapy
administration
Using the Chi-square test, the administration of
chemotherapy was found to be significantly correlated with the
absence of cardiorespiratory diseases (P=0.001). Moreover, using a
multivariate logistic regression analysis, lymph node involvement
[odds ratio (OR)=10.0; 95% confidence interval (CI): 1.07–139.05;
P=0.044] and the absence of cardiorespiratory disease (OR=12.09;
95% CI: 2.66–74.94; P<0.001) were independently associated with
the administration of chemotherapy (Table III).
| Table IIIFactors associated with the
administration of chemotherapy in geriatric patients determined by
univariate and multivariate analysis. |
Table III
Factors associated with the
administration of chemotherapy in geriatric patients determined by
univariate and multivariate analysis.
| | Univariate
analysisa | Multivariate
evaluation by logistic regression analysis |
|---|
| |
|
|
|---|
| Factors, no. (%) | Total no. (n=54) | CT (n=31) | No CT (n=23) | P-value | Odds ratio | 95% CI | P-value |
|---|
| Gender |
| Male | 37 | 22 (71) | 15 (65) | 0.653 | 1.00 | 0.02–0.87 | 0.033 |
|
Female | 17 | 9 (29) | 8 (35) | | 0.17 | | |
| Age, years |
|
75–79 | 31 | 18 (58) | 13 (57) | 0.909 | 1.00 | 0.61–19.75 | 0.171 |
| ≥80 | 23 | 13 (42) | 10 (43) | | 3.17 | | |
| Tumor depth |
|
T1–3 | 20 | 12 (39) | 8 (35) | 0.767 | 1.00 | 0.55–24.24 | 0.191 |
| T4 | 34 | 19 (61) | 15 (65) | | 3.38 | | |
| Nodal status |
|
Positive | 42 | 26 (84) | 16 (70) | 0.213 | 1.00 | 1.07–139.05 | 0.044 |
|
Negative | 12 | 5 (16) | 7 (30) | | 10.00 | | |
| Distant
metastasis |
|
Positive | 14 | 7 (23) | 7 (30) | 0.516 | 1.00 | 0.12–3.66 | 0.658 |
|
Negative | 40 | 24 (77) | 16 (70) | | 0.68 | | |
| Stage |
|
I/II | 18 | 12 (39) | 6 (26) | 0.327 | 1.00 | 0.01–1.26 | 0.081 |
|
III/IV | 36 | 19 (61) | 17 (74) | | 0.15 | | |
| Recurrence
pattern |
|
Peritoneal | 19 | 11 (35) | 8 (35) | 0.957 | 1.00 | 0.12–2.50 | 0.465 |
|
Other | 35 | 20 (65) | 15 (65) | | 0.58 | | |
| Cardiorespiratory
disease |
|
Present | 20 | 6 (19) | 14 (61) | 0.001 | 1.00 | 2.66–74.94 | < 0.001 |
|
Absent | 34 | 25 (81) | 9 (39) | | 12.09 | | |
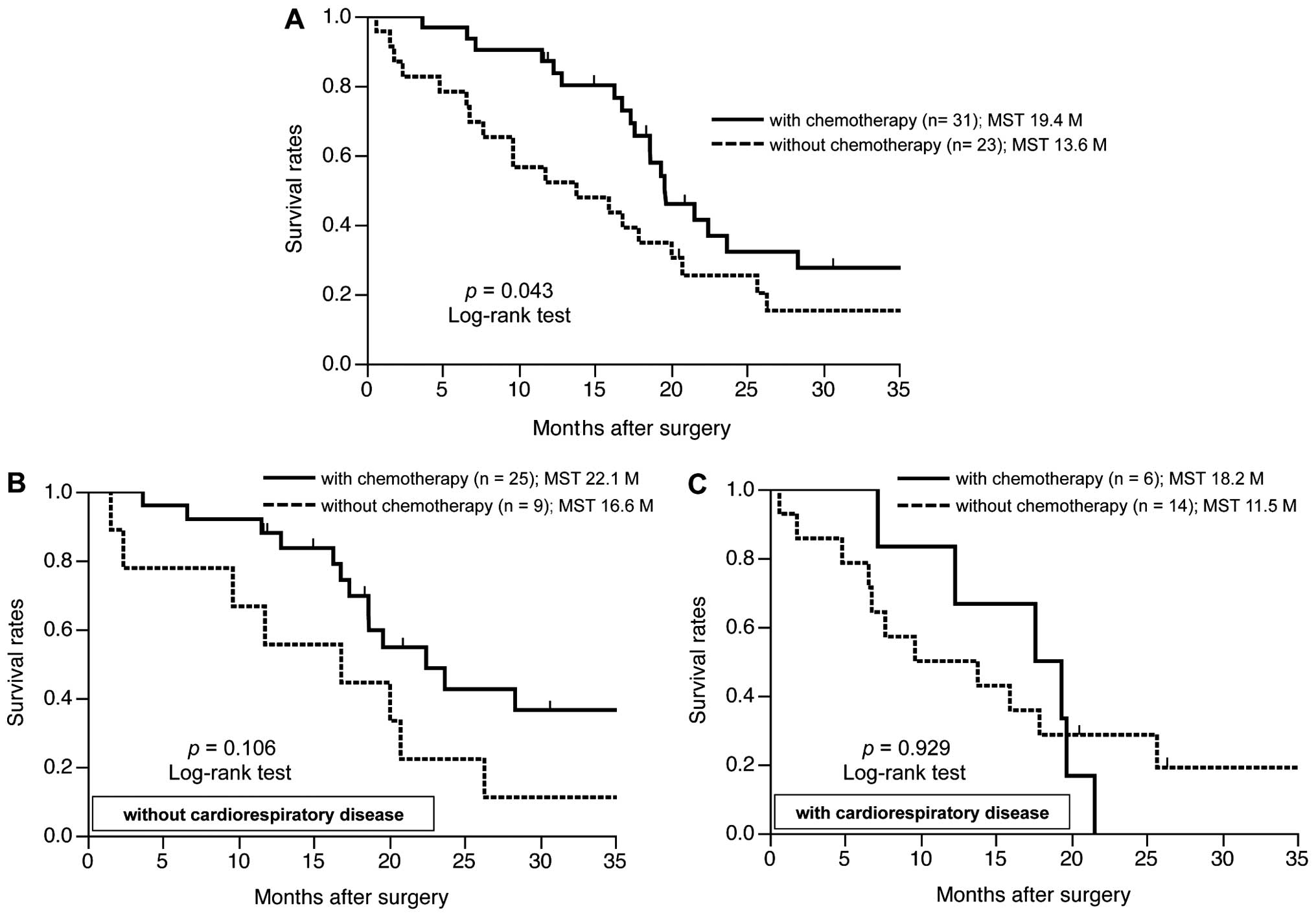
Survival analysis
The geriatric patients treated with chemotherapy
(GPC) had a significantly better prognosis compared to those
without chemotherapy (GP) (median survival time, 19.4 vs. 13.6
months, respectively; P=0.043) (Fig.
1A). As regards cardiorespiratory disease as a concomitant
illness, GPC without cardiorespiratory disease had a better
prognosis compared to GP without cardiorespiratory disease
(P=0.106) (Fig. 1B), whereas there
were no significant differences between GP and GPC with
cardiorespiratory disease (Fig.
1C). The prognostic evaluation using univariate analysis
indicated a significantly better prognosis in patients without
distant metastasis (P<0.001), patients without cardiorespiratory
disease (P=0.020) and patients undergoing chemotherapy (P=0.043).
The multivariate analysis using the Cox proportional hazards model
indicated that the administration of chemotherapy [hazard ratio
(HR)=2.609; 95% CI: 1.173–5.761; P=0.019) and the absence of
distant metastasis (HR=5.169; 95% CI: 2.013–13.651; P=0.001) were
independent factors for better prognosis in geriatric patients with
advanced or recurrent GC, although the absence of cardiorespiratory
disease was not identified as independent factor of a better
prognosis (Table IV).
| Table IVPrognostic factors in geriatric
patients with advanced or recurrent gastric cancer using the Cox
proportional hazards model. |
Table IV
Prognostic factors in geriatric
patients with advanced or recurrent gastric cancer using the Cox
proportional hazards model.
| Univariate
analysisa | Multivariate
analysisb |
|---|
|
|
|
|---|
| Factors | P-value | HR | 95% CI | P-value |
|---|
| Gender |
| Male
vs. female | 0.221 | | - | |
| Age, years |
| 75–79
vs. ≥80 | 0.276 | | - | |
| Tumor depth |
| T4 vs.
T1–3 | 0.228 | | - | |
| Nodal status |
|
Positive vs. negative | 0.211 | | - | |
| Distant
metastasis |
|
Positive vs. negative | <0.001 | 5.169 | 2.013–13.651 | 0.001 |
| Cardiorespiratory
disease |
| Present
vs. absent | 0.020 | 1.368 | 0.627–2.907 | 0.424 |
| Chemotherapy |
| Absent
vs. present | 0.043 | 2.609 | 1.173–5.761 | 0.019 |
Discussion
The overall elderly population is currently
increasing, in Japan as well as other Asian and Western countries
(1, 2). As a result, the number of geriatric
patients with malignant neoplasms is also increasing. Therefore,
there is a need for the development and establishment of a
therapeutic strategy for malignant neoplasms in geriatric patients.
However, the decision to administer chemotherapy to geriatric
patients with malignant neoplasms may be difficult, as the
therapeutic strategy applied to this population is identical to
that for younger patients. The difficulty in standardizing
therapeutic regimens may be due to the fact that the therapeutic
strategies for geriatric cancer patients depend on their physical
and/or social background. Numerous retrospective and prospective
cohort studies regarding the therapeutic indications for geriatric
GC patients are currently performed in Japan; however, the criteria
for selecting surgery or chemotherapy for such patients remain
unclear. It is important to consider clinical characteristics, such
as underlying or concomitant illness, when deciding on the
therapeutic strategy, particularly in geriatric patients.
Therefore, we focused on concomitant illness in geriatric patients
with GC and evaluated its effect on chemotherapeutic
indications.
A significant survival benefit for first- and
second-line chemotherapy compared to BSC in advanced or recurrent
GC was previously reported (19,
20). Therefore, a shift from
first- to second-line chemotherapy may exert a significant effect
on survival benefit. By contrast, although the precise indications
for the administration of first- or second-line chemotherapy for
geriatric GC remains unclear, the non-administration of second-line
chemotherapy was significantly correlated with the presence of
cardiorespiratory disease in the present study (data not
shown).
As regards the survival analysis, the presence of
cardiorespiratory disease was not identified as an independent
factor for poor prognosis. However, the administration of
chemotherapy was an independent factor for better prognosis,
suggesting that chemotherapy safely administered to geriatric GC
patients, even those with cardiorespiratory disease, may contribute
to a better prognosis. Moreover, these findings suggested that the
use of chemotherapy for geriatric GC may be of prognostic
significance regardless of concomitant illness. However,
chemotherapy may exert a beneficial effect on geriatric patients
without critical concomitant illness; thus, the chemotherapeutic
regimen should be adapted for such patients. Therefore, an accurate
assessment of the physical ability of geriatric patients with GC is
required to ensure adequate and safe treatment.
The Comprehensive Geriatric Assessment (CGA) is a
multidimensional tool used to evaluate comorbidities, nutrition,
cognition, functional status and geriatric syndromes. CGA is also
used to identify patients at increased risk of adverse outcomes and
guide management (21). In
previous studies, the CGA tool and the frailty index for geriatric
cancer patients were shown to provide valuable information through
the prediction of complications from chemotherapy and tolerance to
treatment (22, 23).
In the present study, we demonstrated a survival
benefit in geriatric patients with advanced or recurrent gastric
cancer receiving chemotherapy. We also demonstrated that
chemotherapy was safer and better tolerated in geriatric GC
patients without cardiorespiratory diseases. Moreover, geriatric
patients with malignancies commonly exhibit variations in physical
status, cognitive function and social environment. Thus,
assessments of the general condition of geriatric gastric cancer
patients, including various physical, cognitive and social factors,
using methods such as CGA or other modified assessment tools, must
be established as a standard clinical routine. These issues are
currently under evaluation. The clinical application of such
criteria may aid in the decision to administer intensive
chemotherapy to geriatric patients with advanced or recurrent
gastric cancer. Further studies are required to investigate the
reproducibility of the present results in a larger cohort study or
prospective trials and to establish acceptable criteria for cancer
therapy in geriatric gastric cancer patients.
References
|
1
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar
|
|
2
|
Ries LAG, Krapcho M, Mariotto A, Miller
BA, Feuer EJ, Clegg L, Horner MJ, Howlader N, Eisner MP, Reichman M
and Edwards BK: SEE. cancer statistics review. 1975–2004. National
Cancer Institute; Bethesda, MD: 2013
|
|
3
|
Glimelius B, Hoffman K, Haglund U, Nyren O
and Sjoden PO: Initial or delayed chemotherapy with best supportive
care in advanced gastric cancer. Ann Oncol. 5:189–190.
1994.PubMed/NCBI
|
|
4
|
Murad AM, Santiago FF, Petroianu A, Rocha
PR, Rodrigues MA and Rausch M: Modified therapy with
5-fluorouracil, doxorubicin, and methotrexate in advanced gastric
cancer. Cancer. 72:37–41. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pyrhonen S, Kuitunen T, Nyandoto P and
Kouri M: Randomised comparison of fluorouracil, epidoxorubicin and
methotrexate (FEMTX) plus supportive care with supportive care
alone in patients with non-resectable gastric cancer. Br J Cancer.
71:587–591. 1995. View Article : Google Scholar
|
|
6
|
Al-Batran SE, Hartmann JT, Probst S, et al
Arbeitsgemeinschaft Internistische Onkologie: Phase III trial in
metastatic gastroesophageal adenocarcinoma with fluorouracil,
leucovorin plus either oxaliplatin or cisplatin: a study of the
Arbeitsgemeinschaft Internistische Onkologie. J Clin Oncol.
26:1435–1442. 2008. View Article : Google Scholar
|
|
7
|
Boku N, Yamamoto S, Fukuda H, et al:
Fluorouracil versus combination of irinotecan plus cisplatin versus
S-1 in metastatic gastric cancer: a randomised phase 3 study.
Lancet Oncol. 10:1063–1069. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kang YK, Kang WK, Shin DB, et al:
Capecitabine/cisplatin versus 5-fluorouracil/cisplatin as
first-line therapy in patients with advanced gastric cancer: a
randomised phase III noninferiority trial. Ann Oncol. 20:666–673.
2009. View Article : Google Scholar
|
|
9
|
Koizumi W, Narahara H, Hara T, et al: S-1
plus cisplatin versus S-1 alone for first-line treatment of
advanced gastric cancer (SPIRITS trial): a phase III trial. Lancet
Oncol. 9:215–221. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Van Cutsem E, Moiseyenko VM, Tjulandin S,
et al V325 Study Group: Phase III study of docetaxel and cisplatin
plus fluorouracil compared with cisplatin and fluorouracil as
first-line therapy for advanced gastric cancer: a report of the
V325 study group. J Clin Oncol. 24:4991–4997. 2006.PubMed/NCBI
|
|
11
|
Webb A, Cunningham D, Scarffe JH, et al:
Randomized trial comparing epirubicin, cisplatin, and fluorouracil
versus fluorouracil, doxorubicin, and methotrexate in advanced
esophagogastric cancer. J Clin Oncol. 15:261–267. 1997.
|
|
12
|
Catalano V, Bisonni R, Graziano F, et al:
A phase II study of modified FOLFOX as first-line chemotherapy for
metastatic gastric cancer in elderly patients with associated
diseases. Gastric Cancer. 16:411–419. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jin Y, Qiu MZ, Wang DS, et al: Adjuvant
chemotherapy for elderly patients with gastric cancer after D2
gastrectomy. PLoS One. 8:e531492013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim JH, Kim HS, Han AR, et al: Irinotecan,
leucovorin and 5-fluorouracil (modified FOLFIRI) as salvage
chemotherapy for frail or elderly patients with advanced gastric
cancer. Oncol Lett. 4:751–754. 2012.
|
|
15
|
Koizumi W, Akiya T, Sato A, et al: Phase
II study of S-1 as first-line treatment for elderly patients over
75 years of age with advanced gastric cancer: the Tokyo Cooperative
Oncology Group study. Cancer Chemother Pharmacol. 65:1093–1099.
2010.PubMed/NCBI
|
|
16
|
Lee JL, Kang YK, Kang HJ, et al: A
randomised multicentre phase II trial of capecitabine vs S-1 as
first-line treatment in elderly patients with metastatic or
recurrent unresectable gastric cancer. Br J Cancer. 99:584–590.
2008. View Article : Google Scholar
|
|
17
|
Trumper M, Ross PJ, Cunningham D, et al:
Efficacy and tolerability of chemotherapy in elderly patients with
advanced oesophago-gastric cancer: A pooled analysis of three
clinical trials. Eur J Cancer. 42:827–834. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sobin LH, Gospodarowicz MK and Wittekind
C: TN. classification of malignant tumours. 7th. Wiley-Blackwell;
New York, NY: 2009
|
|
19
|
Kang JH, Lee SI, Lim do H, et al: Salvage
chemotherapy for pretreated gastric cancer: a randomized phase III
trial comparing chemotherapy plus best supportive care with best
supportive care alone. J Clin Oncol. 30:1513–1518. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Thuss-Patience PC, Kretzschmar A, Bichev
D, et al: Survival advantage for irinotecan versus best supportive
care as second-line chemotherapy in gastric cancer - a randomised
phase III study of the Arbeitsgemeinschaft Internistische Onkologie
(AIO). Eur J Cancer. 47:2306–2314. 2011. View Article : Google Scholar
|
|
21
|
Caillet P, Canoui-Poitrine F, Vouriot J,
et al: Comprehensive geriatric assessment in the decision-making
process in elderly patients with cancer. ELCAPA study: J Clin
Oncol. 29:3636–3642. 2011.PubMed/NCBI
|
|
22
|
Extermann M and Hurria A: Comprehensive
geriatric assessment for older patients with cancer. J Clin Oncol.
25:1824–1831. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pal SK, Katheria V and Hurria A:
Evaluating the older patient with cancer: understanding frailty and
the geriatric assessment. CA J Clin. 60:120–132. 2010. View Article : Google Scholar : PubMed/NCBI
|