Introduction
Breast cancer is the most frequently diagnosed
cancer in women worldwide and the second leading cause of
cancer-related mortality, accounting for 23% of the total new cases
of cancer (1.38 million) and 14% of the total cancer deaths
(458,400) (1).
Breast cancer recurrence usually occurs within the
first 5 years following diagnosis, with the majority of these
recurrences being hormone receptor-negative or human epidermal
growth factor receptor 2 (HER2)-positive. In certain cases, relapse
may occur after 5 years, which is more common in cases of hormone
receptor-positive cancer with indolent disease and HER2-negative
cancer. A retrospective study evaluating 2,838 cases reported that
the 5-year recurrence risk for patients with stage I, II and III
breast cancer receiving adjuvant therapy was 7, 11 and 13%,
respectively (2,3).
T cells are known to play a critical role in tumor
immune surveillance. Although the role of immune response in breast
cancer has yet to be fully elucidated, certain studies reported
that chemotherapy contributes to overall treatment response by
stimulating the immune response. Antibody-dependent cellular
cytotoxicity plays an important role in the mechanism of action of
trastuzumab and peritumoral lymphocyte infiltration has been found
to be associated with improved response and survival rates in
antineoplastic and trastuzumab therapy (4–7).
Platelets play a balancing role in health and
disease and are the origin of active metabolites and proteins.
Platelets release growth factors, such as platelet-derived growth
factor, platelet factor 4, transforming growth factor β and
vascular endothelial growth factor, which may stimulate tumor
growth and angiogenesis. The association of poor prognosis and the
increase in white blood cells, platelets, or their ratio may be
explained through an inflammatory process evoked by cancer cells
(8,9).
The aim of this study was to retrospectively examine
the survival data of breast cancer patients who received adjuvant
trastuzumab and determine the prognostic value of different
peripheral blood parameters in association with disease-free
survival (DFS).
Patients and methods
Patients
A total of 62 patients treated at the Akdeniz
University Hospital between January, 2008 and August, 2010, who
received adjuvant trastuzumab for early and locally advanced breast
cancer, were retrospectively reviewed.
The study was approved by the Akdeniz University
Clinical Research Ethics Committee.
Statistical analysis
Statistical analyses were performed using SPSS
software, version 20.0 (IBM Corp., Armonk, NY, USA). DFS was
defined as the time period between initial diagnosis and detection
of the first tumor recurrence based on radiological criteria.
Survival was analyzed by the Kaplan-Meier method and the univariate
Cox regression analysis. The variables were investigated using
visual (histograms, probability plots) and analytical methods
(Kolmogorov-Smirnov/Shapiro-Wilk's test) to determine whether they
are normally distributed. A descriptive analysis was presented
using means and standard deviations for normally distributed
variables [platelet-lymphocyte ratio (PLR) measurements]. Variables
with a P-value of <0.10 in the univariate analysis were also
evaluated by multivariate analysis. A P-value of <0.05 was
considered to indicate statistically significant differences.
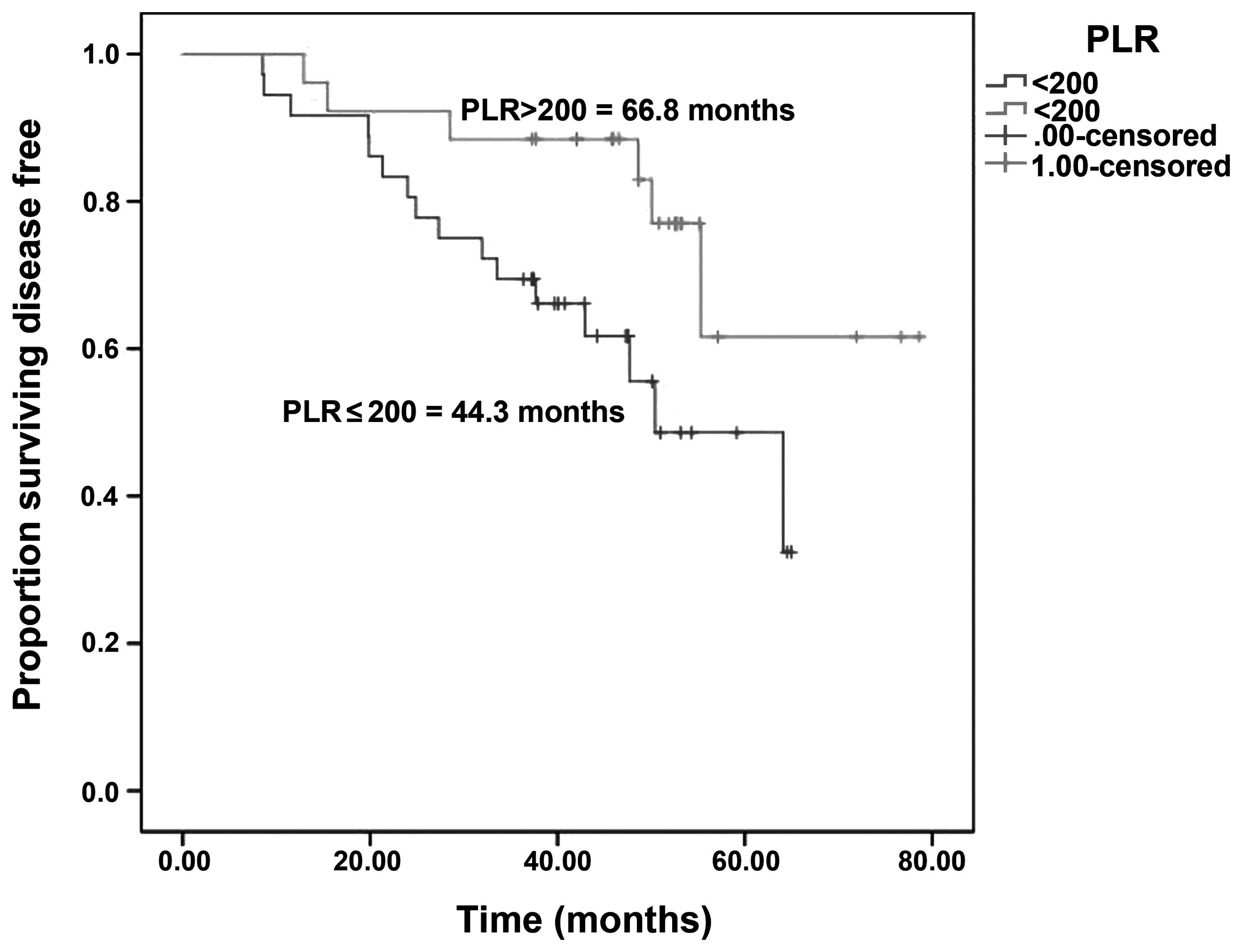
PLR
Prior to treatment, PLR was calculated as the
platelet count divided by the lymphocyte count. Using a number of
different cut-off points, a PLR of 200 was found to represent the
optimum stratification point at which the survival difference
between two groups was maximized.
Results
Patient, disease and treatment
characteristics
In this study, we evaluated the data of 62 patients
diagnosed with breast cancer. The study group consisted of all
patients diagnosed with breast cancer between January, 2008 and
August, 2010. The median follow-up period was 48.4 months. The
median age of the patients was 52 years (range, 24–73 years).
As regards menopausal status, 26 (41.9%) of the
patients were premenopausal and 36 postmenopausal (58.1%). A total
of 75.8% of the patients underwent modified radical mastectomy. The
majority of the tumors were invasive ductal carcinomas (77.4%). At
the time of diagnosis, 11.1% of the patients had stage I, 53.2% had
stage II and 33.9% had stage III disease. Adjuvant chemotherapy
included anthracylines and taxanes in 96.8% of the cases (Table I).
 | Table I.Baseline characteristics of breast
cancer patients. |
Table I.
Baseline characteristics of breast
cancer patients.
| Characteristics | Patient no. (%)
(n=62) |
|---|
| Age, years |
|
|
Median | 52 |
|
Range | 24–73 |
| Stage |
|
| I | 7 (11.3) |
| II | 33 (53.2) |
| III | 21 (33.9) |
|
Missing | 1 (1.6) |
| Menopausal
status |
|
|
Premenopausal | 26 (41.9) |
|
Postmenopausal | 36 (58.1) |
| Tumor type |
|
| Ductal
invasive | 48 (77.4) |
| Lobular
invasive | 14 (22.6) |
| Tumor grade |
|
| I | 6 (9.7) |
| II | 25 (40.3) |
| III | 30 (48.4) |
|
Missing | 1 (1.6) |
| Hormone receptor
status |
|
|
Positive | 35 (56.5) |
|
Negative | 27 (43.5) |
| Chemotherapy
regimens |
|
|
FACa-docetaxel | 46 (74.2) |
|
FECb-docetaxel | 9 (14.5) |
|
TACc | 6 (9.7) |
|
CMFd | 1 (1.6) |
| Operation |
|
| Breast
conserving surgery | 15 (24.2) |
| Modifiied
radical mastectomy | 47 (75.8) |
| Baseline eosinophil
count, ×103/mm3 |
|
|
Median | 70 |
|
Range | 10–680 |
| Baseline PLR |
|
| 200≥ | 36 (58.1) |
|
200< | 26 (41.9) |
A total of 22 patients (35.5%) developed metastasis
after diagnosis, with 18 (29%) of the patients developing distant
and 4 (6.5%) local metastasis, whereas 3 (4.8%) patients developed
brain metastasis (data not shown).
Survival analysis
The median follow-up period was 48.4 months and the
patients had a median DFS of 64.1 months.
There were no significant associations between DFS
and age, menopausal status, stage or hormone receptor status. The
univariate analysis revealed that DFS was significantly affected by
tumor grade [P=0.086 (95% CI for HR: 0.96–1.62)], PLR [P=0.021 (95%
CI for HR: 1.33–4.16)] and eosinophil count [P=0.029 (95% CI for
HR: 1.03–1.91)]. However, eosinophil count [P= 0.017 (95% CI for
HR: 1.23–8.69)] retained significance with multivariate
analysis.
The median DFS was 44.3 vs. 66.8 months in patients
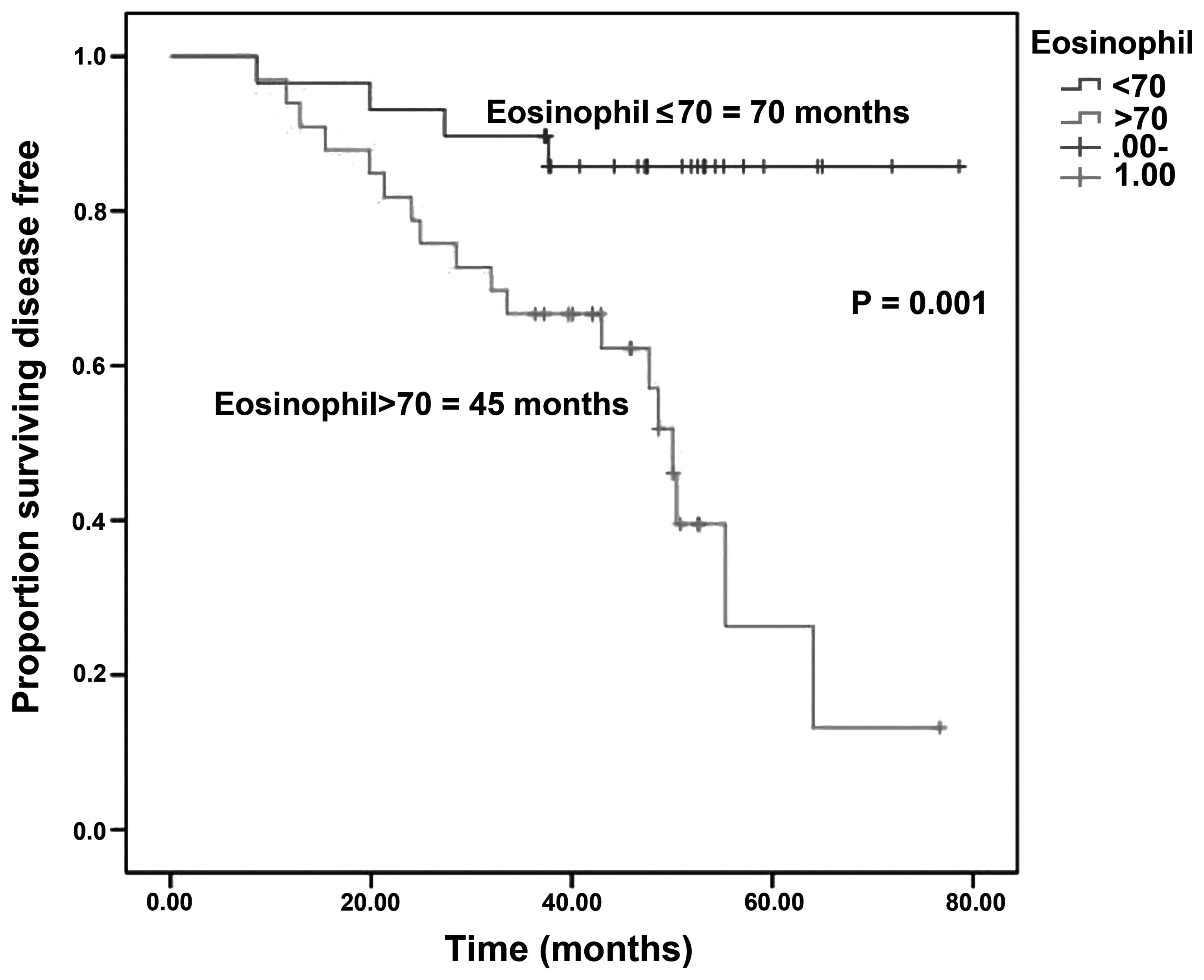
with PLR ≤200 vs. >200 (log-rank test; P=0.001) (Fig. 1) and 70 vs. 45 months in patients with
eosinophil count ≤70 vs. >70×103/mm3
(log-rank test; P=0.001) (Fig.
2).
Discussion
To the best of our knowledge, this study is the
first to demonstrate the significance of PLR and eosinophil count
in breast cancer patients receiving adjuvant trastuzumab
therapy.
Blood markers such as PLR and eosinophil count are
simple, rapidly available laboratory markers. A previous study,
including >25,000 patients, demonstrated the significance of
inflammatory markers in the prediction of the outcome of various
types of cancer (10). Feng et
al found that PLR is associated with tumor progression and may
be considered as an independent marker of poor prognosis in
patients who undergo esophagectomy for esophageal squamous cell
carcinoma without neoadjuvant or adjuvant treatment (11). Certain studies demonstrated that the
presence of pretreatment lymphopenia is associated with poor cancer
survival or tumor response and it has not only prognostic, but also
predictive potential (12–14). In a study conducted by the Radiation
Therapy Oncology Group, lymphopenia and hormone receptor negativity
were found to be independent prognostic factors indicating poor
survival in breast cancer patients with brain metastases (15). A more recent study conducted by the
same group concluded that lymphocyte count and LDH levels may
predict overall survival (16).
Peritumoral lymphocyte infiltration in trastuzumab therapy is known
to enhance treatment response and survival (7). Combination chemotherapies were shown to
reduce peripheral lymphocyte count in cancer patients. These
findings suggest that treatment-induced lymphopenia may be
associated with an increased tumor response (17). In our study, we demonstrated that
patients with PLR >200 and eosinophil count
<70×103/mm3 exhibited better DFS
rates.
In early-stage breast cancer, the recurrence rate
varies between 20 and 30%. Trastuzumab therapy is known to
significantly reduce recurrence and mortality, with a 50% reduced
risk of breast cancer recurrence and 30% improved survival rate. In
patients with HER2-overexpressing early-stage breast cancer treated
with trastuzumab-based therapy, the most common location for
disease progression is the isolated central nervous system
(18–20). This has been associated with the
inability of trastuzumab to penetrate the blood-brain barrier or
the brain-metastatic breast tumor cells losing the expression of
HER2; it may also be explained by the overall effectiveness of
trastuzumab in disease control, except in the central nervous
system (21). In our study, 35.3% of
our patients receiving adjuvant trastuzumab therapy developed
recurrence. Of these patients, 3 (6.3%) developed isolated brain
metastases. The respective percentage was 2.56% in the study
conducted by Olson et al (21).
When recurrence of breast cancer is diagnosed, the
initial evaluation should include hormone receptor status, DFS, age
and menopausal status. Previous research in this field has
demonstrated that estrogen and progesterone receptor status are
independent predictors of survival after the first recurrence
(22). While Clark et al
(23) and Insa et al (24) found that these were independent
predictors of patient survival following relapse, Koenders et
al (25) found no such
association. In our study, we observed no correlations between
hormone receptor status, menopausal status and disease-free
survival.
In conclusion, PLR and eosinophil count are
cost-effective, readily available worldwide, non-invasive and safe
and, when combined with other markers, such as patient age, tumor
stage and tumor histology, may be effectively used for patients
with breast cancer.
References
|
1
|
Jemal A and Bray F: Global Cancer
Statistics. CA Cancer J Clin. 61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel R and DeSantis C: Cancer treatment
and survivorship statistics, 2012. CA Cancer J Clin. 62:220–241.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Brewster AM, Hortobagyi GN, Broglio KR, et
al: Residual risk of breast cancer recurrence 5 years after
adjuvant therapy. J Natl Cancer Inst. 100:1179–1183. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Vicente Conesa MA, Garcia-Martinez E,
Billalabeitia EG, Benito AC, Garcia TG, Garcia VV and Ayala de la
Peña F: Predictive value of peripheral blood lymphocyte count in
breast cancer patients treated with primary chemotherapy. The
Breast. 21:468–474. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mackall CL, Fleisher TA, Brown MR, et al:
Lymphocyte depletion during treatment with intensive chemotherapy
for cancer. Blood. 84:2221–2228. 1994.PubMed/NCBI
|
|
6
|
Smith I, Procter M, Gelber RD, et al: HERA
study team: 2-year follow-up of trastuzumab after adjuvant
chemotherapy in HER2-positive breast cancer: a randomised
controlled trial. Lancet. 369:29–36. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Gennari R, Menard S, Fagnoni F, et al:
Pilot study of the mechanism of action of preoperativetrastuzumab
in patients with primary operable breast tumors overexpressing
HER2. Clin Cancer Res. 10:5650–5655. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Coussens LM and Werb Z: Inflammation and
cancer. Nature. 420:860–867. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nurden AT: Platelets, inflammation and
tissue regeneration. Thromb Haemost. 105:(Suppl 1). 13–33. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Proctor MJ, Morrison DS, Talwar D, et al:
A comparison of inflammation-based prognostic scores in patients
with cancer. A Glasgow Inflammation Outcome study. Eur J Cancer.
47:2633–2641. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Feng JF, Huang Y and Liu JS: Combination
of neutrophil lymphocyte ratio and platelet lymphocyte ratio is a
useful predictor of postoperative survival in patients with
esophageal squamous cell carcinoma. Onco Targets Ther. 6:1605–1612.
2013.PubMed/NCBI
|
|
12
|
Papatestas AE, Lesnick GJ, Genkins G and
Aufses AH Jr: The prognostic significance of peripheral lymphocyte
counts in patients with breast carcinoma. Cancer. 37:164–168. 1976.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pattison CW, Woods KL and Morrison JM:
Lymphocytopenia as an independent predictor of early recurrence in
breast cancer. Br J Cancer. 55:75–76. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ray-Coquard I, Cropet C, Van GM, et al:
Lymphopenia as a prognostic factor for overall survival in advanced
carcinomas, sarcomas and lymphomas. Cancer Res. 69:5383–5391. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Le Scodan R, Massard C, Mouret-Fourme E,
et al: Brain metastases from breast carcinoma: validation of the
Radiation Therapy Oncology Group recursive partitioning analysis
classification and proposition of a new prognostic score. Int J
Radiat Oncol Biol Phys. 69:839–845. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Le Scodan R, Massard C, Jouanneau L,
Coussy F, Gutierrez M, Kirova Y, Lerebours F, Labib A and
Mouret-Fourme E: Brain metastases from breast cancer: proposition
of new prognostic score including molecular subtypes and treatment.
J Neurooncol. 106:169–176. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Delyon J, Mateus C, Lefeuvre D, et al:
Experience in daily practice with ipilimumab for the treatment of
patients with metastatic melanoma: an early increase in lymphocyte
and eosinophil counts is associated with improved survival. Ann
Oncol. 24:1697–1703. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Moja L, Tagliabue L, Balduzzi S, et al:
Trastuzumab containing regimens for early breast cancer. Cochrane
Database Syst Rev. 4:CD0062432012.PubMed/NCBI
|
|
19
|
Slamon D, Eiermann W, Robert N, et al:
Adjuvant trastuzumab in HER2-positive breast cancer. N Engl J Med.
365:1273–1283. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Early Breast Cancer Trialists'
Collaborative Group (EBCTCG), . Effects of chemotherapy and
hormonal therapy for early breast cancer on recurrence and 15-year
survival: an overview of the randomised trials. Lancet.
365:1687–1717. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Olson EM, Abdel Rausoul M, Maly J, Wu CS,
Lin NU and Shapiro CL: Insidence and risk of central nervous system
metastases as site of first recurrence in patients in with
HER2-positive breast cancer treated with adjuvant trastuzumab. Ann
Oncol. 24:1526–1533. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tsuji W, Teramukai S, Ueno M, Toi M and
Inamoto T: Prognostic factors for survival after first recurrence
in breast cancer: a retrospective analysis of 252 recurrent cases
at a single institution. Breast Cancer. 21:86–95. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Clark GM, Sledge GW Jr, Osborne CK and
McGuire WL: Survival from first recurrence: relative importance of
prognostic factors in 1,015 breast cancer patients. J Clin Oncol.
5:55–61. 1987.PubMed/NCBI
|
|
24
|
Insa A, Lluch A, Prosper F, Marugan I,
Martinez-Agullo A and Garcia-Conde J: Prognostic factors predicting
survival from first recurrence in patients with metastatic breast
cancer: analysis of 439 patients. Breast Cancer Res Treat.
56:67–78. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Koenders PG, Beex LV, Kloppenborg PW,
Smals AG and Benraad TJ: Human breast cancer: survival from first
metastasis. Breast Cancer Study Group. Breast Cancer Res Treat.
21:173–180. 1992. View Article : Google Scholar : PubMed/NCBI
|