Introduction
Angiomyolipoma is a benign, mesenchymal
hamartomatous neoplasm composed of variable combinations of adipose
tissue, smooth muscle cells and abnormal blood vessels.
Angiomyolipoma often arises from the kidney, but has also been
described in extrarenal locations, such as the liver (1), uterus (2),
and other infrequent sites (3–5).
Angiomyolipomas arising from the skeleton are extremely rare and
have been previously reported in the thoracic (6) and cervical spine (7), as well as the tibia (8). However, the radiological characteristics
of angiomyolipomas arising from the skeleton have not been
adequately described due to our limited experience with this type
of tumor. Thus, the skeletal occurrence of angiomyolipoma
represents a diagnostic challenge prior to surgery, in terms of
unfamiliarity, unusual presentation and absence of characteristic
imaging findings. We herein report a case of angiomyolipoma of the
rib in a 44-year-old male patient that was diagnosed by
pathological examination following surgical resection, and discuss
the imaging findings of angiomyolipomas arising from the skeleton
in combination with relevant published studies.
Case report
Patient history
A 44-year-old male patient presented ~2 months prior
with a 3-year history of repeated attacks of right chest pain and
was found to have a local mass in the right anterolateral chest. On
physical examination, the mass was ovoid, firm, smooth, poorly
mobile and tender to palpation. No pigmented lesions were observed
in the skin. All the laboratory test results were within the normal
range. Written informed consent was obtained from the patient for
the publication of his medical details.
Examination
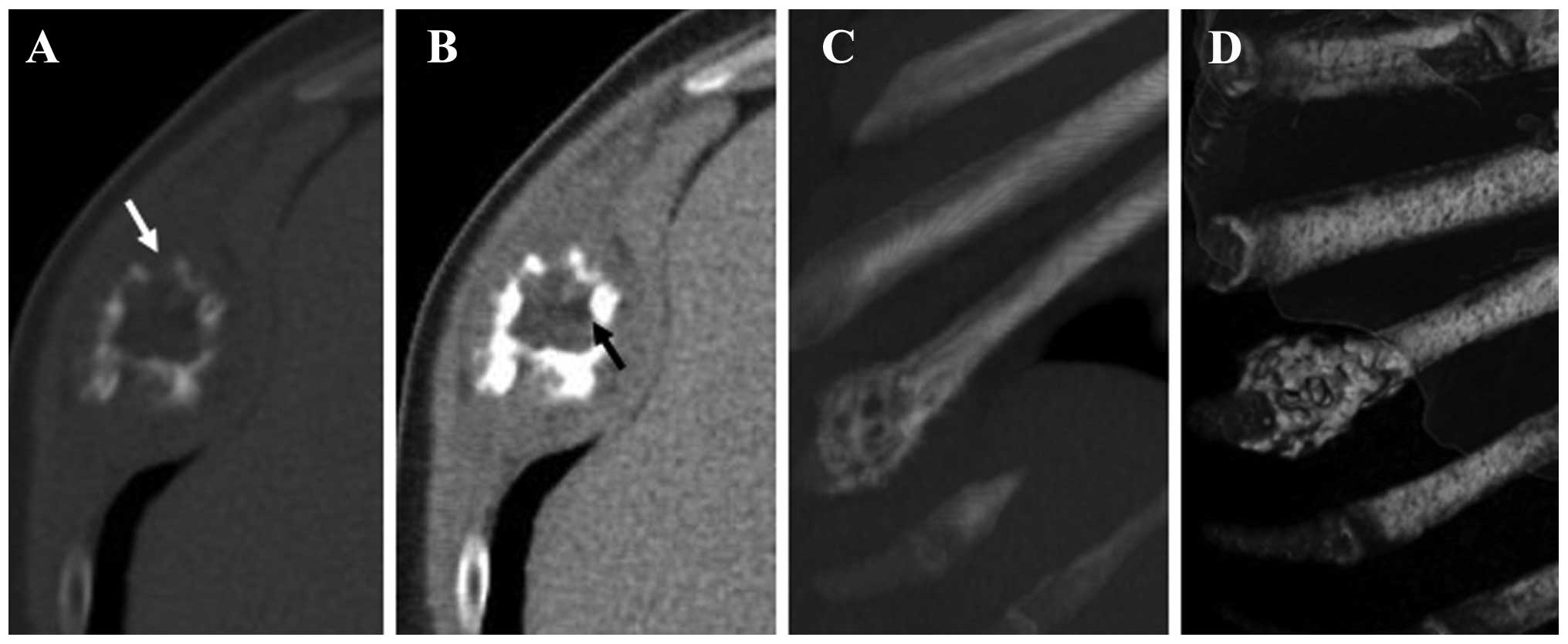
A chest computed tomography (CT) scan revealed that
the mass was located in the right 8th anterior rib, with localized
expansive destruction and a discontinuous bone cortex. The central
bone texture was irregularly destroyed and replaced with
heterogeneous soft tissue density. The margin of the area of bone
destruction was not very sharp, and there was some residual coarse
and thickened bone cortex. The adjacent soft tissue was invaded by
the lesion breaking through the cortex, and an oval soft tissue
mass surrounding the area of bone destruction was observed. Maximum
intensity projection and 3D volume-rendering revealed the
enlargement of the right 8th anterior rib, with patchy destruction
of the bone and internal septum (Fig.
1). The patient also underwent abdominal ultrasonography and a
cerebral CT scan, which did not reveal any other lesions.
Treatment
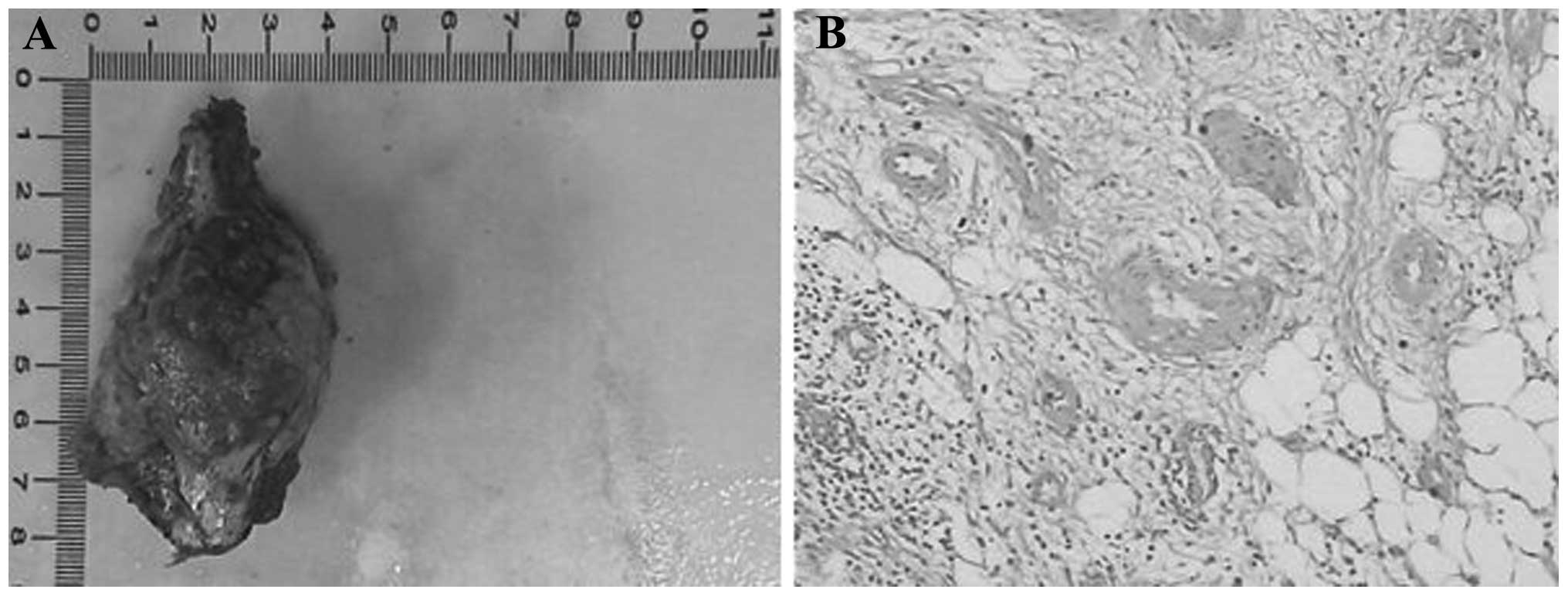
The patient underwent surgical excision of the
lesion with partial costectomy. Macroscopically, there was a
7.2×5.5×3.5-cm well-circumscribed, reddish in color, firm mass in
the proximal segment of the right 8th rib adjacent to the costal
cartilage. The right 8th subcostal nerve and blood vessel were
compressed by the tumor. On pathological examination, the tumor was
confirmed to be an angiomyolipoma, consisting of mature adipocytes,
spindle cells and vascular channels of various sizes (Fig. 2). The patient is being followed up by
clinical physical examinations and CT scan and remains
recurrence-free at 18 months postoperatively.
Discussion
Angiomyolipoma belongs to a family of tumors arising
from perivascular epithelioid cells, referred to as PEComas, with
the kidney being the most frequent site involved (9). Approximately 20% of renal
angiomyolipomas are associated with tuberous sclerosis complex,
which is a multisystemic disease with an autosomal dominant
inheritance (3,10). Extrarenal angiomyolipomas are rare,
apart from those occurring in the liver, and occurrence in the
skeleton is extremely rare. Owing to the lack of experience with
this type of tumor and limited data in the literature reagrding the
radiological manifestations of skeletal angiomyolipomas, this tumor
may be easily misdiagnosed.
The preoperative diagnosis of angiomyolipoma may be
difficult due to the variations in the ratio of the three
components (fat, blood vessels and smooth muscle bundles) among
different tumors, particularly tumors with a minimal amount of
adipose tissue. Therefore, ascertaining the presence of fat is
vital for the diagnosis of angiomyolipoma. CT and magnetic
resonance imaging (MRI) are sensitive methods for detecting adipose
tissue. The fatty component of angiomyolipoma displays low
attenuation on CT and high signal intensity on T1- and T2-weighted
MR images. In the present case, there was a small amount of fat
tissue within the lesion, with a CT value of −38.4 Hounsfield
units. Two previous cases of skeletal angiomyolipomas located in
the thoracic and the cervical spine have been reported (6,7). Insabato
et al (8) reported a case of
primary monotypic epithelioid angiomyolipoma, a distinct and
definable variant of angiomyolipoma, located in the tibia. We took
notice of certain interesting findings in these previously reported
cases of skeletal angiomyolipoma, as well as in the present case.
All the patients were middle-aged or elderly men, and no case was
associated with tuberous sclerosis complex. This is consistent with
the majority of extrarenal angiomyolipoma cases, namely that
extrarenal angiomyolipomas present mostly without evidence of
tuberous sclerosis complex (2). The
tumor morphology was usually consistent, with the tumors being
round or oval in shape. Spinal angiomyolipomas were relatively
common, accounting for two cases in these patients. The skeletal
changes were mainly osteolytic or expansive destruction, mostly
associated with cortical interruption. The margin of bone
destruction was well-defined or unclear; a soft mass with a
well-defined margin was occasionally found to surround the area of
bone destruction. The two cases of spinal angiomyolipoma exhibited
infiltrative properties and they were non-encapsulated, involving
adjacent structures. In the present case, the CT scan revealed an
expansive lesion with a surrounding well-defined soft mass. The
findings were consistent with those of cases previously reported in
the literature, in that the skeletal angiomyolipoma may break
through the bone cortex and invade adjacent soft tissues.
The radiological differential diagnosis for
angiomyolipoma of the skeleton includes chondroma, osteofibrous
dysplasia and tuberculosis (11–13).
Chondroma is associated with characteristic calcifications within
the lesion. Osteofibrous dysplasia presents with expansive
destruction, with a thinner but continuous bone cortex and no soft
mass surrounding the lesion. Skeletal tuberculosis may be
differentiated through the characteristic sequestrum or
calcification, as well as the soft tissue tuberculosis abscess
surrounding the bone destruction. Infiltrative angiomyolipoma must
be distinguished from various malignant tumors, such as sarcoma and
metastatic tumors. In addition to identifying the presence of fat
within the lesion, enhanced performance on CT and MRI may also
contribute to the differential diagnosis of angiomyolipoma. The
blood vessels in the tumor are strongly enhanced during the early
phase of enhancement.
To the best of our knowledge, this is the first
reported case of angiomyolipoma of the rib. Although angiomyolipoma
is a tumor with a benign clinical course, angiomyolipomas of the
skeleton usually exhibit infiltrative properties. When tumors of
the skeleton in adult male patients display areas of fat within the
lesion on imaging, angiomyolipoma of the skeleton should be
considered, regardless of whether there is a well-defined soft mass
surrounding the area of bone destruction.
References
|
1
|
Petrolla AA and Xin W: Hepatic
angiomyolipoma. Arch Pathol Lab Med. 132:1679–1682. 2008.PubMed/NCBI
|
|
2
|
Yaegashi H, Moriya T, Soeda S, Yonemoto Y,
Nagura H and Sasano H: Uterine angiomyolipoma: Case report and
review of the literature. Pathol Int. 51:896–901. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Oishi K, Fukuda S, Sakimoto H, Eto T,
Takahashi M and Nishida T: Angiomyolipoma of the colon: Report of a
case. Surg Today. 39:998–1001. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Saito M, Yuasa T, Nanjo H, Tsuchiya N,
Satoh S and Habuchi T: A case of testicular angiomyolipoma. Int J
Urol. 15:185–187. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mikoshiba Y, Murata H, Ashida A, Saito N,
Koga H, Uhara H and Okuyama R: Case of a cutaneous angiomyolipoma
in the ear. J Dermatol. 39:808–809. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sakaida H, Waga S, Kojima T, Kubo Y,
Matsubara T and Yamamoto J: Thoracic spinal angiomyolipoma with
extracanal extension to the thoracic cavity. A case report. Spine
(Phila Pa 1976). 23:391–394. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Jia N, Wang C, Liu HM, Yu H and Wang J:
Angiomyolipoma occurred at the cervical spine. Joint Bone Spine.
75:620–621. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Insabato L, De Rosa G, Terracciano LM,
Fazioli F, Di Santo F and Rosai J: Primary monotypic epithelioid
angiomyolipoma of bone. Histopathology. 40:286–290. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Alvarez Alvarez C, Fernández Sanromán J,
Fernández Castilla M and Antón Badiola I: Sporadic oral
angiomyolipoma. Case report. Med Oral Patol Oral Cir Bucal.
12:E391–E393. 2007.PubMed/NCBI
|
|
10
|
Nelson CP and Sanda MG: Contemporary
diagnosis and management of renal angiomyolipoma. J Urol.
168:1315–1325. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Qasem SA and DeYoung BR: Cartilage-forming
tumors. Semin Diagn Pathol. 31:10–20. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bethapudi S, Ritchie DA, Macduff E and
Straiton J: Imaging in osteofibrous dysplasia, osteofibrous
dysplasia-like adamantinoma, and classic adamantinoma. Clin Radiol.
69:200–208. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hu N, Tan Y, Cheng Z, Hao Z and Wang Y: Hu
N1: FDG PET/CT in Monitoring Antituberculosis Therapy in Patient
With Widespread Skeletal Tuberculosis. Clin Nucl Med. 40:919–921.
2015. View Article : Google Scholar : PubMed/NCBI
|