Introduction
Oligoastrocytoma (OA) is a type of brain tumor
derived from neuroepithelial tissue that contains a variety of
different neoplastic glial cells. OAs may be referred to as mixed
gliomas, whereas OA cells originate from oligodendrocytes,
ependymal cells and astrocytes. The most common types of mixed OA
encountered in clinical practice include OA/OA2 [World Health
Organisation (WHO) grade II] and anaplastic OA (AOA)/OA3 (WHO grade
III) (1,2) OAs may originate anywhere within the
cerebral hemispheres, although the frontal and temporal lobes are
the most common locations. OAs comprise 5–10% of gliomas and 1% of
all brain tumors and they typically develop in young and
middle-aged adults (aged 30–50 years), whereas very few children
are diagnosed with OA (3). The
typical symptoms include seizures, headaches and personality
changes, but the clinical manifestations and imaging
characteristics of OAs are highly variable, which may further
increase the difficulty of clinical diagnosis. In this report, we
present the case of a patient with OA that was initially
misdiagnosed as multiple sclerosis (MS).
Case report
A 46-year-old man was admitted to the Neurology
Department of the China-Japan Union Hospital (Changchun, China).
After recovering from a cold, the patient experienced dizziness and
unsteadiness when walking. These symptoms continued for 5 days. The
patient's medical history revealed that he had previously suffered
from optic neuritis, but his vision improved following
corticosteroid injections. A magnetic resonance imaging (MRI) scan
of the head revealed abnormal, flaky, hypointense T1 and
hyperintense T2 signals near the right basal ganglia and in the
posterior horn of the right lateral ventricle. The visually evoked
potentials (VEPs) were abnormal. The cerebrospinal fluid (CSF)
oligoclonal bands (OCBs) were positive and, therefore, the patient
was diagnosed with MS. Following this diagnosis, methylprednisolone
was administered and the patient was discharged from the hospital
after his symptoms improved. However, 1 week later the patient
returned to the hospital with more severe dizziness and
unsteadiness when walking and was admitted to the Neurology
Department of The First Affiliated Hospital of Jilin University
(Changchun, China) on January 17, 2014. Magnetic resonance
spectroscopy (MRS) and an enhancement scan of the head revealed
multiple abnormal signals, including a significant decrease in
N-acetyl aspartate (NAA), a mild decrease in creatine (Cr), a
significant increase in choline-containing compounds (Cho) and a
mild increase in lactate (Lac). The MRS analysis indicated that a
tumorigenic lesion could not be excluded; however, the results of
the CSF analysis on January 20, 2014 were normal. The patient was
diagnosed with multiple intracranial lesions and a biopsy was
suggested, but was rejected by the patients family. On February 6,
2014, the dizziness and unsteadiness became more pronounced,
whereas additional symptoms appeared, including dysarthria,
dysphagia, blurred vision and numbness of the right-sided limbs.
Due to the worsening of the symptoms, the patient returned to our
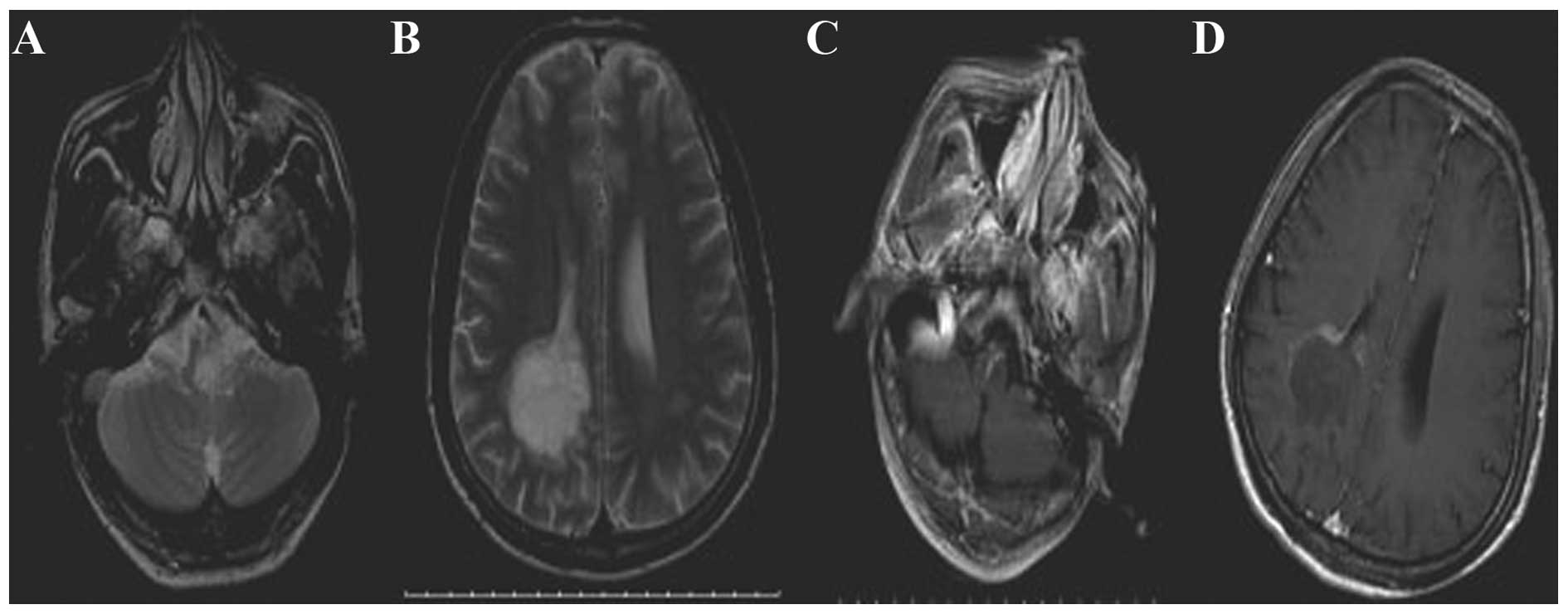
hospital for treatment. A head MRI on February 18, 2014 revealed
flaky, hypointense T1-weighted and hyperintense T2-weighted signals
and a fluid-attenuated inversion recovery (FLAIR) signal with
unclear edges in the medulla oblongata. These signals were
strengthened after an enhancement scan (Fig. 1A and B). The head MRI also revealed
flaky, hypointense T1, hyperintense T2 and FLAIR signals in the
right basal ganglia region and in the white matter around the
anterior and posterior horn of the right lateral ventricle. The
posterior horn lesion appeared flaky, with low-signal intensity
that was marginally strengthened after the enhancement scan,
particularly close to the edges (Fig. 1C
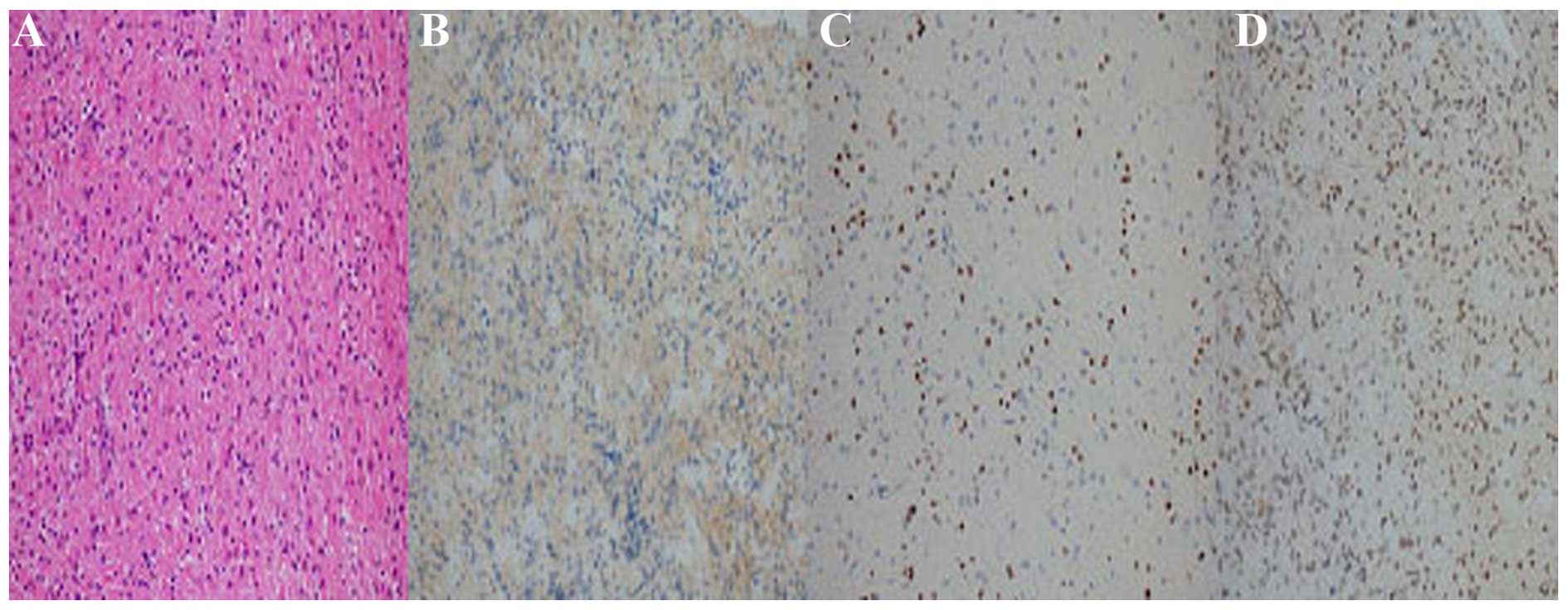
and D). A biopsy below the trigone of the right
parieto-occipital cortex was performed, and differential
immunohistochemistry-based neuropathological examination using a
set of diagnostic glioma markers led to the diagnosis of OA (WHO
grade II). Immunohistochemistry yielded the following results:
Ki-67 (~1%); p53 (−); glial fibrillary acidic protein (GFAP) (+);
IDH1-R132H (−); oligodendrocyte lineage transcription factor 2
(Olig2) (+); O6-methylguanine DNA methyltransferase
(MGMT) (+ in >75% of the tumor cells); epidermal growth factor
receptor (EGFR) (±); CD68 (−); myelin basic protein (partially +);
and neurofilament (+) (Fig. 2). The
biopsied tissue displayed weak staining for the astrocytoma marker
EGFR, but was positive for the oligodendrocyte marker Olig2 and the
OA marker MGMT in ~75% of tumor cells. These results combined were
indicative of WHO grade II OA. The patient underwent craniotomy,
while the symptoms persisted and were gradually exacerbated. The
patient succumbed 1 month later in a local hospital due to a
pulmonary infection.
Discussion
The etiology of OA has not yet been fully
elucidated. Long-term ionizing radiation exposure is the only
currently known risk factor, although it has been suggested that OA
is the result of multiple factors, such as genetic diversity, viral
infections and immune factors. The symptoms of OA are complex and
depend on tumor location and size. OA commonly occurs in the
supratentorial region, particularly in the frontal lobe, followed
by the temporal lobe, parietal lobe, thalamus, corpus callosum,
ventricle, cerebellopontine angle region and brainstem. The tumor
often crosses lobes and, therefore, may involve multiple lobes of
the brain and the superficial cortex. The involvement of multiple
lobes of the brain may explain the appearance of epilepsy-like
symptoms in OA. Epilepsy is the most common clinical symptom in OA
and ~80% of OA patients suffer from seizures (3). Other symptoms include ataxia, headaches,
memory loss, personality changes and other mental changes,
including intelligence decline and dementia (4). Therefore, the clinical symptoms of OA
are frequently not characteristic of glioma.
The initial symptoms of the patient in the present
case were atypical and contributed to the original misdiagnosis.
The patient had previously suffered from optic neuritis, a
condition associated with MS, and his vision had improved following
corticosteroid injections. Finally, the premonitory cold symptoms,
abnormal VEP and OCB reinforced the misdiagnosis of MS.
MS is a common cause of space-occupying lesions. The
treatment of choice is high-dose dexamethasone to reduce the brain
edema, which is empirically associated with clinical and
radiological improvement in 1–3 weeks. However, if there is no
clinical improvement, a stereotactic biopsy of the space-occupying
lesion is recommended (3).
Although CT scans may show patchy lesions,
low-density shadows and unclear edges, the image density may be
lower in cases with cystic tumors and CT lacks the required
specificity for OA diagnosis. Dotted, nodular and short
stripe-shaped calcifications may be detected surrounding the tumor,
and these characteristics may gather, in part, at one end of a
quasi-circular tumor. The sensitivity and specificity of MRI are
significantly better compared with those of CT for lesion detection
and identification. T1-weighted images mainly show low-intensity
signals, whereas T2-weighted images and FLAIR show homogeneous
high-intensity signals with unclear edges. Since OAs grow slowly,
vasogenic edema and mass effects do not commonly occur. Thus,
T1-weighted images may be less efficient at detecting tumor
boundaries. By contrast, T2-weighted images may more effectively
reflect real tumor boundaries; however, it is difficult to
distinguish the tumor from the surrounding edematous area. There is
usually no or only a mild enhancement of the lesion area, as
visualized by MRI. To visualize the infiltration range of the
lesion, MRS is superior to conventional MRI. The MRS results of the
patient revealed a significant decrease in NAA, a mild decrease in
Cr, a significant increase in Cho and a mild increase in Lac. In
contrast to this result, Cho may be decreased in highly malignant
gliomas, which is likely associated with necrosis (5). The change in the ratios of Cho/Cr and
NAA/Cr provides guidance for the classification of the malignant
grade of the tumor and the projected survival time of the patient
(6). These results indicate that a
tumorigenic lesion may be underlying the observed symptoms.
Histopathological examination remains the gold
standard for OA diagnosis. Indirect signs of OA, such as edema of
the brain or the brain stem, basal ganglia or corpus callosum
volume gain and blurring of the lateral fissure may be observed.
Histological examination may show the diffuse distribution of tumor
cells, which are polygonal or circular, with nuclear condensation.
The immunohistochemical markers used are Olig2, a marker of
oligodendrocytes; GFAP, a marker of astrocytes; EGFR, a marker
associated with astrocytomas; and MGMT, a marker associated with OA
(4). Immunohistochemical analysis of
this patient's biopsy revealed tumor cell expression of Olig2, GFAP
and MGMT, indicating that the patient had an OA.
OAs (grade II) are considered to be low-grade
tumors, and they generally grow at a slower rate compared with
malignant anaplastic OAs (grade III). However, OAs may evolve into
anaplastic oligoastrocytomas over time. OA growth generally depends
on the percentage of astrocytoma in the tumor, as astrocytomas tend
to grow more rapidly compared with oligodendrogliomas.
Due to the rarity and high misdiagnosis rate of OA,
it is suggested that clinical physicians update their knowledge
regarding brain tumor classification and increase their awareness
of rare tumors. Promisingly, the rapid advances in imaging
technologies, particularly functional MRI, appears to enable
accurate confirmation of the location and extent of injury in the
brain. With the combination of current imaging technology, biopsy
and pathological examination, it is now possible to accurately
diagnose these relatively rare tumors.
References
|
1
|
Gwak HS, Yee GT, Park CK, Kim JW, Hong YK,
Kang SG, Kim JH, Seol HJ, Jung TY, Chang JH, et al: Temozolomide
salvage chemotherapy for recurrent anaplastic oligodendroglioma and
oligo-astrocytoma. J Korean Neurosurg Soc. 54:489–495. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Louis DN, Ohgak H, Wiestler OD, Cavenee
WK, Burger PC, Jouvet A, Scheithauer BW and Kleihues P: The 2007
WHO classification of tumours of thecentral nervous system. Acta
Neuropathol. 114:97–109. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ruiz J and Lesser GJ: Low-grade gliomas.
Curr Treat Options Oncol. 10:231–242. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gorlia T, Delattre JY, Brandes AA, Kros
JM, Taphoorn MJ, Kouwenhoven MC, Bernsen HJ, Frénay M, Tijssen CC,
Lacombe D and van den Bent MJ: New clinical, pathological and
molecular prognostic models and calculators in patients with
locally diagnosed anaplastic oligodendroglioma or oligoastrocytoma.
A prognostic factor analysis of European Organisation for Research
and Treatment of Cancer Brain Tumour Group Study 26951. Eur J
Cancer. 49:3477–3485. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cheng LL, Anthony DC, Comite AR, Black PM,
Tzika AA and Gonzalez RG: Quantification of microheterogeneity in
glioblastoma multiforme with ex vivo high resolution magic-angle
spinning (HRMAS) proton magnetic resonance spectroscopy. Neuro
Oncol. 2:87–95. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chawla S, Krejza J, Vossough A, Zhang Y,
Kapoor GS, Wang S, O'Rourke DM, Melhem ER and Poptani H:
Differentiation between oligodendroglioma genotypes using dynamic
susceptibility contrast persusion-weighted imaging and proton MR
spectroscopy. AJNR Am J Neuroradiol. 34:1542–1549. 2013. View Article : Google Scholar : PubMed/NCBI
|