Introduction
Uterine sarcoma is a relatively rare tumor that
accounts for ~8% of all uterine malignancies (1). In the Japanese population, 13–19% of
these tumors are classified as endometrial stromal sarcoma (ESS)
(2,3).
Due to the changes in the World Health Organization classification
in 2003, which classified high-grade ESS as undifferentiated
endometrial sarcoma (4), low-grade
ESS (LG-ESS) may simply be referred to as ESS in some cases,
although the classification reverted to its original form in 2014
(5). LG-ESS presents with lymph node
metastasis in 9–33% cases (6,7) and displays characteristics that include
frequent development as an intravascular tumor with intracardiac
extension (ICE). The number of reported cases of LG-ESS with
clinically obvious intravascular extension was only 19 over the
last 38 years (8,9); however, up to one-third of the cases
presented with extrauterine extension, including microscopic
worm-like plugs within the vessels (4). Such tumors must be differentiated from
deep venous thrombosis, whereas benign leiomyoma presents with
characteristics similar to intravenous leiomyomatosis. Other
uterine malignancies may also rarely present as a tumor embolism
(10).
An intravascular tumor is associated with a direct
risk of sudden death due to pulmonary embolism; thus, it is crucial
to plan a precise surgical strategy based on the exact extent of
the intravascular tumor. We treated a case of LG-ESS with ICE, in
which preoperative contrast-enhanced computed tomography (CT)
indicated a misleading tumor location. We herein describe this case
for educational purposes and provide a literature review on the
imaging modalities.
Written informed consent was obtained from the
patient for the publication of her medical details.
Case report
The patient was a 58-year-old woman who was gravida
5, para 3 and postmenopausal. A fibroid in her uterus had been
diagnosed at 52 years of age, but no medical intervention was
performed due to the imminent menopause. The patient had no other
medical history and had undergone no gynecological follow-up.
During a routine medical checkup, a marginal elevation of the serum
liver enzymes and impaired glucose tolerance were found, but the
patient was asymptomatic.
The patient visited a general hospital for an
investigation of the elevated liver enzymes. a thoracoabdominal CT
revealed an irregular tumor in the uterus, with intravenous spread
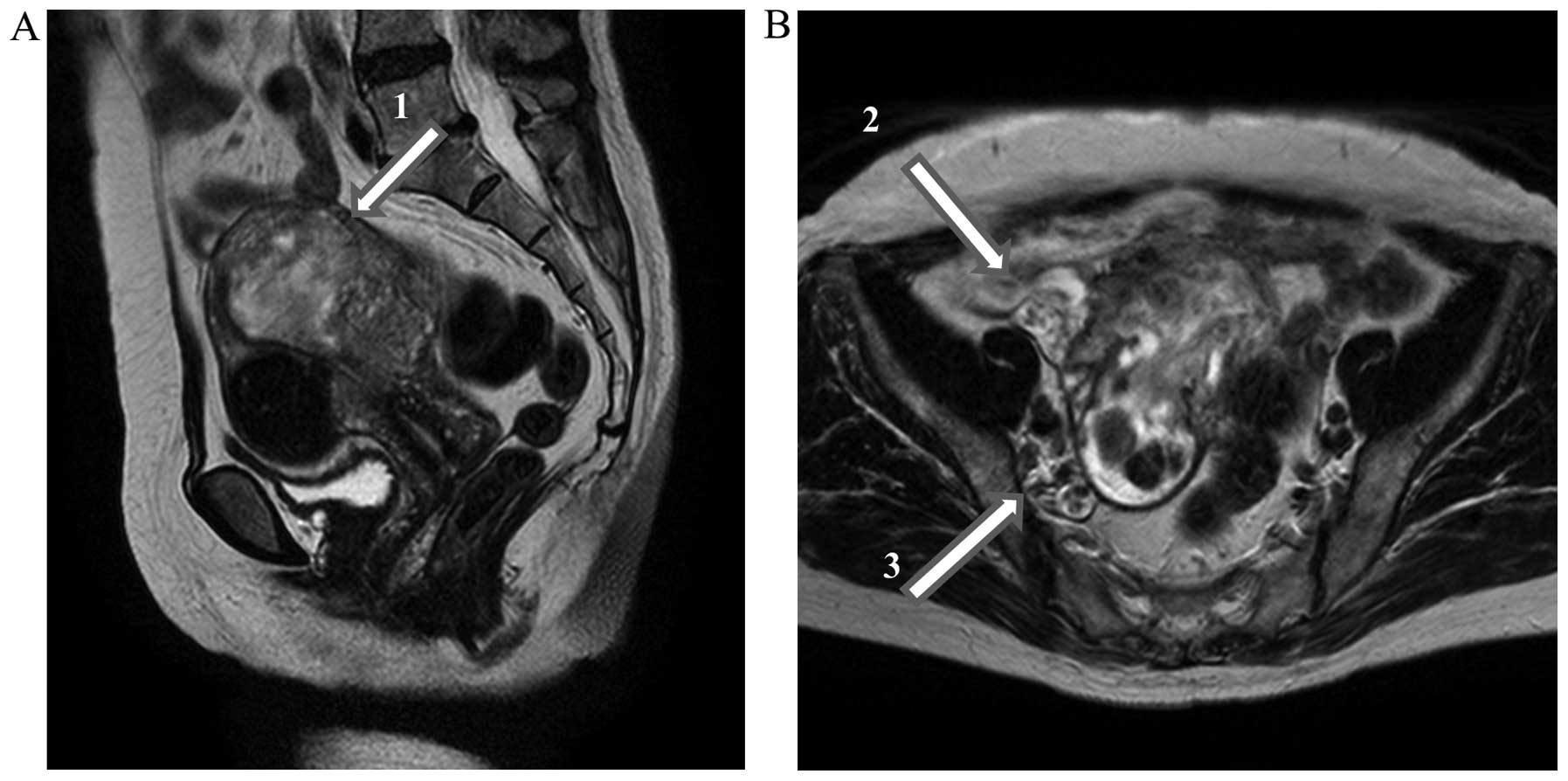
of the tumor to the inferior vena cava (IVC). On pelvic magnetic
resonance imaging (MRI), an irregular tumor was identified in the
right posterior wall of the uterus. The tumor mainly exhibited
low-signal intensity on T1-weighted imaging (T1WI), mainly
high-signal intensity on T2WI (Fig.
1), a mild to intermediate effect with gadolinium contrast
agent, and a high-signal intensity on diffusion weighted imaging
(DWI). The presence of a non-endometrial tumor located near the
cavity suggested that sarcoma had invaded from just below the
endometrium, with a low density on T2WI due to the normal
myometrium underlying the tumor invasion. These findings were
compatible with a diagnosis of ESS.
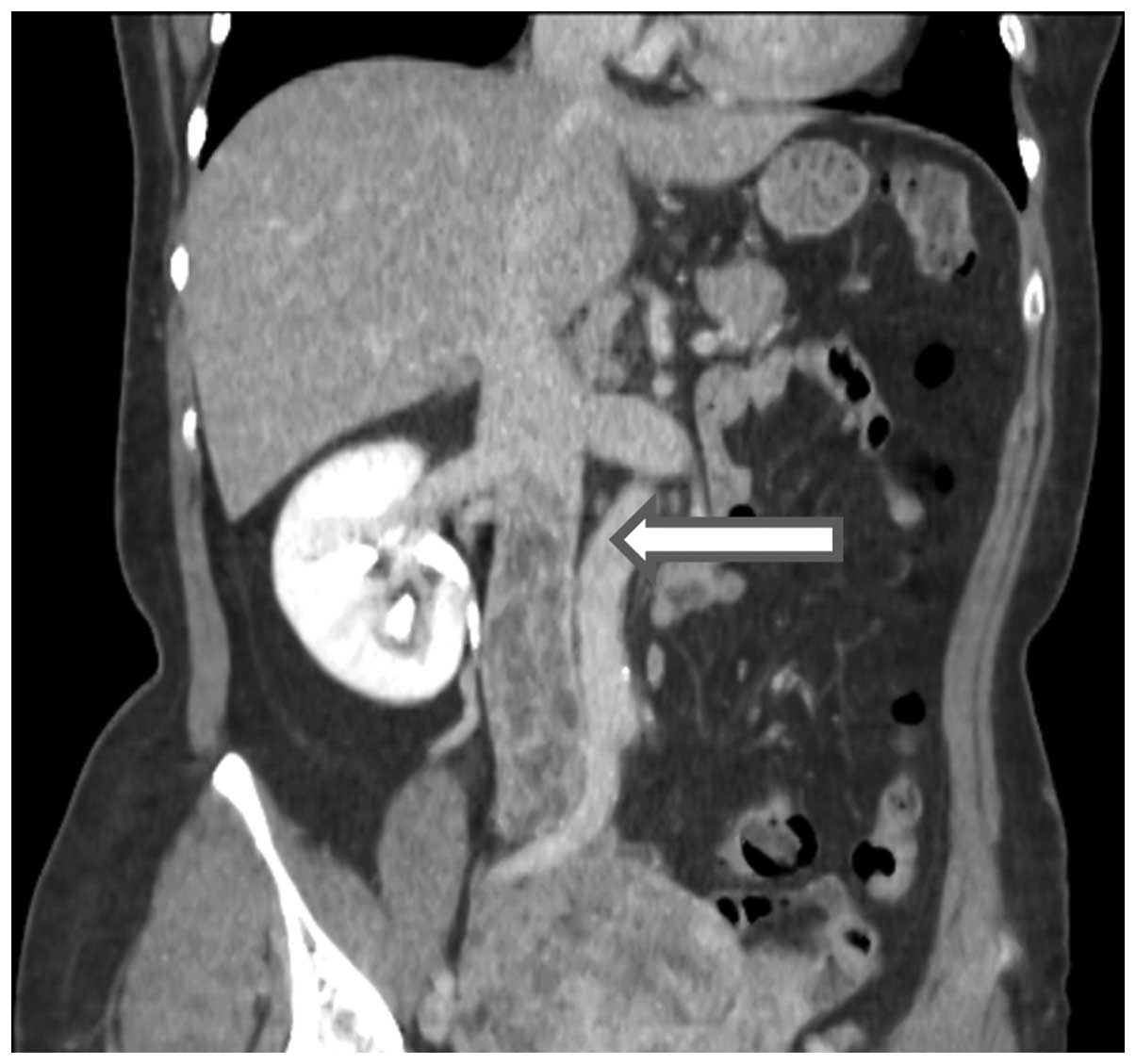
The patient was admitted to our hospital for
treatment of the uterine tumor. Following emergency admission, the
patient underwent dynamic contrast-enhanced CT of the whole body to
determine the extent of the tumor. CT in the venous phase indicated
that the tip of the intravenous tumor was at the level of the renal
veins (Fig. 2), without thrombosis or
a tumor pulmonary embolus. The routes of extension were via the
internal iliac and ovarian veins. The MRI scan indicated that the
tumor was located near the cavity, but the cytological examination
of the endocervix and endometrium was negative for malignancy.
A surgical team of gynecological oncologists and
vascular surgeons was assembled. Anticoagulation with
unfractionated heparin was performed until surgery to prevent
thrombogenesis. Considering the extent of the tumor, it was feared
that insertion of an IVC filter would interfere with the
manipulation of the liver. Thus, a filter for prevention of
pulmonary embolism was not inserted preoperatively. Laparotomy was
performed for hysterectomy, bilateral salpingo-oophorectomy and
debulking of the intravenous tumor. The gynecological oncologist
team performed a hysterectomy with extension of the range of
resection to that of radical hysterectomy on the right side of the
uterus, in which small vessels were invaded by the tumor. However,
it was difficult to remove the tumor completely from the deep
parametrium and paracolpium. A perioperative pathological
examination by frozen section analysis did not indicate obvious
malignancy. Thus, we did not perform a complete resection,
considering the balance between the invasiveness of the operation
and the therapeutic merit.
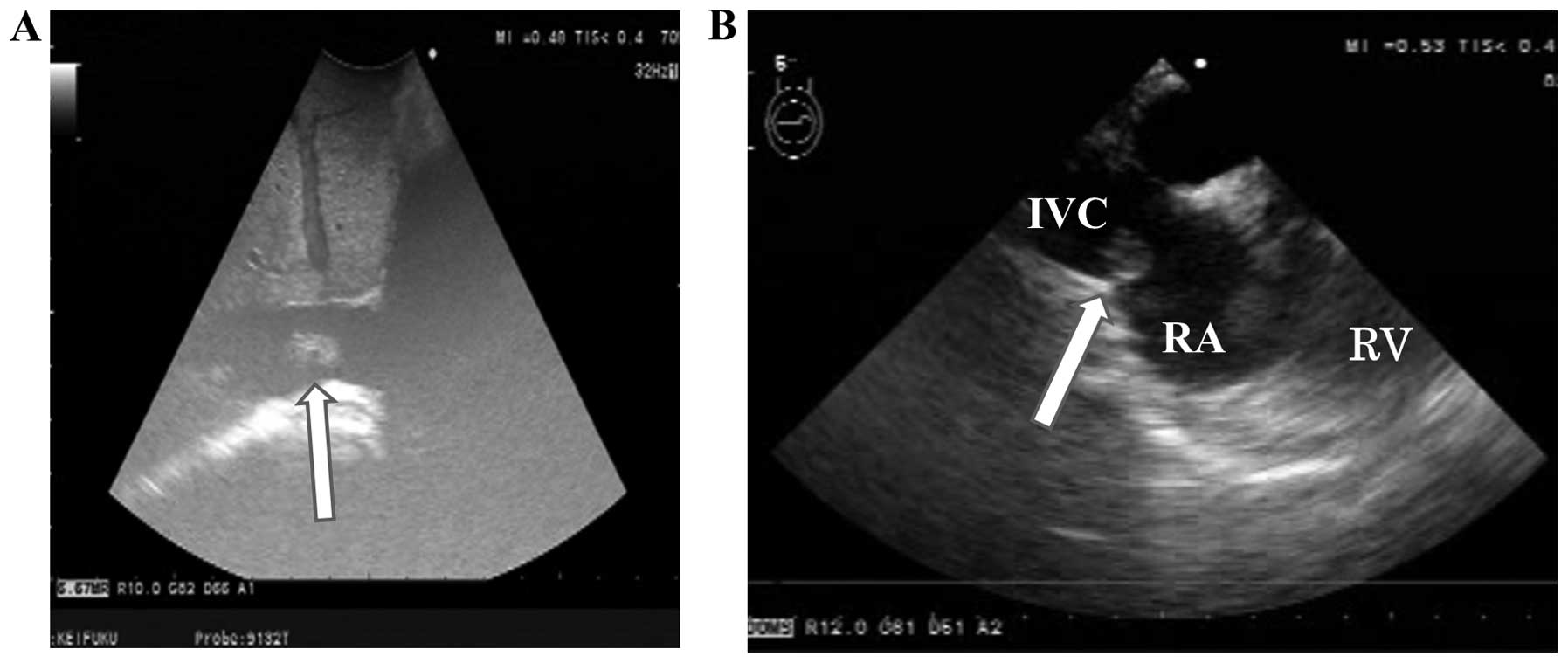
Subsequently, the vascular surgery team took over to
remove the intravascular tumor. On preoperative planning, the tumor
was present below the level of the renal veins; however, a
perioperative ultrasound scanning of the IVC revealed a
free-floating tumor in the form of a thin multinodular plate
extending to the right atrium (Fig.
3). Manipulation of the liver was required, but was associated
with the risk of tumor pulmonary embolisation. a cardiovascular
surgery team performed emergency thoracotomy with median sternotomy
and removed the intracardiac tumor through cardiotomy of the right
atrium using extracorporeal circulation without circulatory arrest.
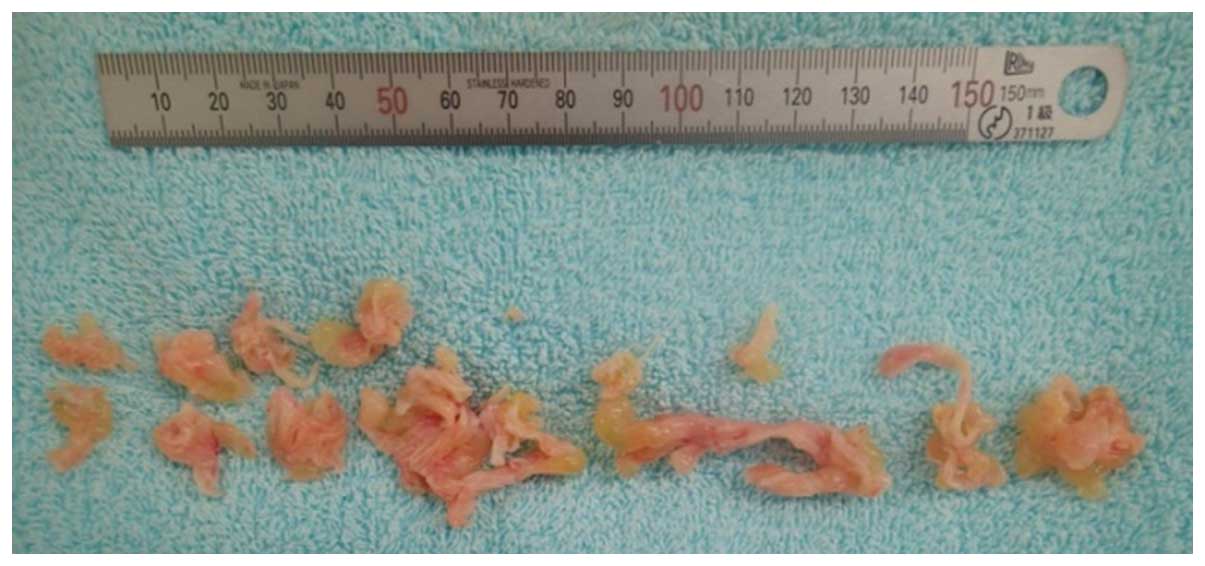
After closing the heart, a radiologist inserted a filter in the IVC
immediately below the right atrium and the vascular surgery team
exposed the IVC behind the liver, cut the vessel wall open and
removed the intravascular tumor under IVC cross-clumping (Fig. 4).
Following removal of the tumor above the renal
veins, the gonadal veins were separated from the IVC, and the IVC
was detached below the level of the renal veins. This procedure was
performed to prevent future tumor pulmonary embolisation, as the
tumor was not removed completely. The amount of perioperative blood
loss was 7,200 ml. Transfusion of 38 units of packed red blood
cells, 30 units of frozen fresh plasma and 10 units of platelets
was required.
On transecting the IVC, bilateral grade 2 pedal
edema appeared immediately after the procedure, but had improved by
postoperative day (POD) 10. Contrast-enhanced CT on POD 10 revealed
a thrombus in the bilateral common to internal iliac veins. The
thrombus was originally right-sided and had an extensive range. It
was difficult to distinguish between the thrombus and tumor growth;
thus, anticoagulation therapy with warfarin was started for
differentiation. No other adverse events occurred, including
surgical site infection, and the patient was discharged on POD
23.
Pathological examination of the resected uterine
tumor established a final diagnosis of LG-ESS. Benign leiomyoma
also existed in the uterine corpus, but the intravascular tumors
were consistent with sarcoma. Thus, the tumor was classed as
clinical stage IIIA (International Federation of Gynecology and
Obstetrics 2008). Residual tumors were present in the right common
iliac vein, internal iliac vein, parametrium, and paracolpium.
Therefore, MRI with a gadolinium contrast agent was performed 1
month after the operation. The range of the poor-contrast area in
the bilateral common to internal iliac veins was reduced by
warfarin, compared with that on enhanced CT immediately after the
operation. The area in which the original intravascular residual
tumor displayed an irregular pattern in T1WI, T2WI and DWI was not
extended. Thus, we concluded that the tumor had not undergone a
sudden increase in size.
Postoperative hormonal therapy was recommended and
the patient received 400 mg/day medroxyprogesterone acetate (MPA)
for a year. The residual tumor almost disappeared and the patient
remains recurrence-free for 1 year following MPA therapy.
Discussion
We treated a case of uterine tumor with
intravascular involvement. The imaging findings indicated a
straightforward diagnosis of sarcoma with tumor thrombus; however,
benign leiomyoma presents similarly to intravenous leiomyomatosis.
A diagnosis of malignancy based on intravenous tumor development
detected by imaging may lead to unnecessary chemotherapy or
radiotherapy (11). MRI is a useful
tool for distinguishing between benign leiomyoma and sarcoma, as in
the present case, but degenerated benign leiomyomas may have
findings similar to those of sarcomas, which may present with
difficulties in differentiating between the two (12,13). As
pathological examination of stromal tumors is difficult to perform
preoperatively, it is crucial to diagnose by surgical resection. In
cases with intravascular lesions, it is also crucial to prevent
future pulmonary embolism. Thus, the principle of treating such
cases is to plan an optimal surgical strategy.
In planning the surgical strategy, it is important
to be able to accurately predict the tumor extent preoperatively;
however, this proved not to be possible in the current case. On
preoperative planning, the tip of the tumor was considered to be
located at the level of the renal veins, based on contrast-enhanced
CT. Intravascular tumors located in the IVC above the renal veins
were not identified on this scan. This may be because these tumors
were flat and plate-like in shape, free-floating and mobile in the
vasculature. Another possibility is that the tumor grew rapidly in
the 5 days between the CT scan and the operation. However, given
that CT at a previous hospital performed 3 weeks earlier indicated
similar findings, it appears reasonable to conclude that the
sensitivity of CT was limited for the detection of free-floating
lesions in the bloodstream. In fact, the sensitivity of CT
angiography for detection of a free-floating thrombus has been
reported to be only 60% (14).
Multislice CT may exhibit a better efficacy (15), although this depends on the clinical
conditions and the form of the intravascular tumor. As regards the
present case, it was crucial to confirm the location of the upper
tip of the tumor by perioperative ultrasound scanning, regardless
of the CT findings. otherwise, instant transection of the IVC may
have caused pulmonary embolism. The key educational point of this
case is that, although CT is widely performed, it is important to
acknowledge the limitations of this method.
It was previously reported that >50% of
intravenous LG-ESS cases exhibited ICE (8). In such cases, the extent of the tumor
should be determined using modalities such as MRI and
ultrasonography, in addition to CT. MRI provides good soft tissue
resolution and helps to distinguish an intravascular tumor from a
non-tumor thrombus (16–18), whereas Doppler ultrasonography is also
useful (16). Transthoracic
ultrasonography of the IVC and heart would normally be performed.
However, the transesophageal method may be selected in a case of
unknown tumor origin or in which the tumor extent is unclear by
transthoracic examination, or when detailed knowledge of the
cardiac function is required, such as cases with tricuspid valve
involvement (19). Indeed,
perioperative transesophageal echocardiography was required in our
patient.
Our case was asymptomatic and was incidentally
discovered during a routine medical checkup. This was rather
fortunate, as fatal congestive heart failure may be the initial
presentation (8,20). In this case, elevation of serum liver
enzymes was most likely caused by another reason, since it
persisted even after tumor removal. However, liver injury may be
caused by liver congestion due to the intravascular tumor in the
IVC and right atrium in similar cases; therefore, transesophageal
echocardiography may be useful prior to surgery.
18-fluorodeoxyglucose (FDG) positron emission tomography-CT
(PET-CT) may also be a viable choice for determining the tumor
location or distinguishing between sarcoma and benign leiomyoma.
PET-CT has been reported as an effective tool for the detection of
uterine sarcoma metastasis (21), but
reports are limited for LG-ESS (22,23).
Certain tumors and metastatic lesions are known to exhibit a low
FDG uptake (24) and its accuracy for
intravascular lesions is unreported to date; thus, even if
performed preoperatively, tumors in the IVC above the level of the
renal veins may not be detected.
Multimodal imaging is costly and time-consuming, but
it is important to determine the extent of a tumor preoperatively,
as it significantly affects surgical resection planning, including
route, order of procedures, methods, devices and the need for
extracorporeal circulation.
We herein presented a case of LG-ESS with ICE, in
which the extent of the tumor was not accurately predicted on
preoperative CT. In similar cases, accurate determination of the
tumor extent for planning the surgical strategy should be performed
using multiple imaging methods.
Acknowledgements
This manuscript was proofread by a native
English-speaking proofreader of the Palabra Language services,
Kyoto, Japan.
References
|
1
|
Brooks SE, Zhan M, Cote T and Baquet CR:
Surveillance, epidemiology and end results analysis of 2677 cases
of uterine sarcoma 1989-1999. Gynecol Oncol. 93:204–208. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sagae S, Yamashita K, Ishioka S, Nishioka
Y, Terasawa K, Mori M, Yamashiro K, Kanemoto T and Kudo R:
Preoperative diagnosis and treatment results in 106 patients with
uterine sarcoma in Hokkaido, Japan. Oncology. 67:33–39. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fujita H, Adachi S, Kigawa J, Sugiyama T
and Takeuchi S: A clinicopathological study of uterine sarcoma in
last decade - a retrospective study of KCOG/USSG inter group study.
Adv obstet Gynecol. 56:463–465. 2004.(In Japanese).
|
|
4
|
Hendrickson MR, Tavassoli FA, Kempson RL,
et al: Mesenchymal tumors and related lesions. Pathology and
genetics of tumours of the breast and female genital organs.
Tavassoli FA and Devilee P: (3rd). (Lyon). International Agency for
Research on Cancer. 233–244. 2003.
|
|
5
|
Oliva E, Carcangiu ML, Carinelli SG, et
al: Mesenchymal tumors. WHO Classification of Tumours of Female
Reproductive Organs (4th). Kurman RJ, Carcangiu ML, Herrington CS
and Young RH: (Lyon). International Agency for Research on Cancer.
135–147. 2014.
|
|
6
|
Leath CA III, Huh WK, Hyde J Jr, Cohn DE,
Resnick KE, Taylor NP, Powell MA, Mutch DG, Bradley WH, Geller MA,
et al: A multi-institutional review of outcomes of endometrial
stromal sarcoma. Gynecol Oncol. 105:630–634. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Riopel J, Plante M, Renaud MC, Roy M and
Têtu B: Lymph node metastases in low-grade endometrial stromal
sarcoma. Gynecol Oncol. 96:402–406. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lo KW, Yu MY and Cheung TH: Low-grade
endometrial stromal sarcoma with florid intravenous component.
Gynecol Obstet Invest. 66:8–11. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gabal S, Ashour Z, Hamada G, Aziz SA,
Khairy H, Badawy H, Hamada EM and Saied K: Low-grade endometrial
stromal sarcoma with intravenous extension to the heart. Medscape J
Med. 11:232009.PubMed/NCBI
|
|
10
|
Dzieciuchowicz ŁS, Słowinski M, Brzeziński
JJ and Kycler W: Tumor embolus due to uterine cancer. Med Sci
Monit. 15:CS155–CS157. 2009.PubMed/NCBI
|
|
11
|
Nagumo M, Kiso I, Misumi T, Yasudo M,
Nakada K and Mukai M: Cardiac extension of intravenous
leiomyomatosis with successful resection. Tokai J Exp Clin Med.
22:125–131. 1997.PubMed/NCBI
|
|
12
|
Tamura R, Kashima K, Asatani M, Nishino K,
Nishikawa N, Sekine M, Serikawa T and Enomoto T: Preoperative
ultrasound-guided needle biopsy of 63 uterine tumors having high
signal intensity upon T2-weighted magnetic resonance imaging. Int J
Gynecol Cancer. 24:1042–1047. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ueda M, Otsuka M, Hatakenaka M and Torii
Y: Uterine endometrial stromal sarcoma located in uterine
myometrium, MRI appearance. Eur Radiol. 10:780–782. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ferrero E, Ferri M, Viazzo A, Labate C,
Pecchio A, Berardi G, Piazza S, Cumbo P and Nessi F: Free-floating
thrombus in the internal carotid artery, Diagnosis and treatment of
16 cases in a single center. Ann Vasc Surg. 25:805–812. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sun C, Wang XM, Liu C, Xv ZD, Wang DP, Sun
XL and Deng K: Intravenous leiomyomatosis, Diagnosis and follow-up
with multislice computed tomography. Am J Surg. 200:e41–e43. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fasih N, Shanbhogue Prasad AK, Macdonald
DB, Fraser-Hill MA, Papadatos D, Kielar AZ, Doherty GP, Walsh C,
McInnes M and Atri M: Leiomyomas beyond the uterus, Unusual
locations, rare manifestations. Radiographics. 28:1931–1948. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cohen DT, Oliva E, Hahn PF, Fuller AF Jr
and Lee SI: Uterine smooth-muscle tumors with unusual growth
patterns: Imaging with pathologic correlation. AJR Am J Roentgenol.
188:246–255. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kang LQ, Zhang B, Liu BG and Liu FH:
Diagnosis of intravenous leiomyomatosis extending to heart with
emphasis on magnetic resonance imaging. Chin Med J (Engl).
125:33–37. 2012.PubMed/NCBI
|
|
19
|
Baca López FM, Martínez-Enriquez A,
Castrejón-Aivar FJ, Ruanova-León D and Yánez-Gutiérrez L:
Echocardiographic study of an intravenous leiomyoma: Case report
and review of the literature. Echocardiography. 20:723–725. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Barksdale J, Abolhoda A and Saremi F:
Intravenous leiomyomatosis presenting as acute Budd-Chiari
syndrome. J Vasc Surg. 54:860–863. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sadeghi R, Zakavi SR, Hasanzadeh M,
Treglia G, Giovanella L and Kadkhodayan S: Diagnostic performance
of fluorine-18-fluorodeoxyglucose positron emission tomography
imaging in uterine sarcomas, Systematic review and meta-analysis of
the literature. Int J Gynecol Cancer. 23:1349–1356. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Luo Y, Feng R and Li F: FDG PET/CT
appearance of tumor thrombus of ovarian vessels masquerading as
retroperitoneal fibrosis. Clin Nucl Med. 40:501–503. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Takizawa M, Tanaka N, Tsunezuka Y,
Katayanagi K and Kurumaya H: Solitary pulmonary metastasis of
low-grade uterine endometrial stromal sarcoma resected 31 years
before. Japan J Thorac Surg. 67:333–336. 2014.(In Japanese).
|
|
24
|
Inoue K, Tsubamoto H, Kawata S, Hao H,
Ikeda Y, Oku N and Hirota S: 18F-fluorodeoxyglucose uptake and
clinicopathological features of recurrent or metastatic endometrial
stromal sarcoma. J Obstet Gynaecol Res. 40:576–582. 2014.
View Article : Google Scholar : PubMed/NCBI
|