Introduction
Lymphoepithelioma-like gastric carcinoma (LELC) is a
rare type of gastric cancer with distinct clinicopathological
characteristics, which was first reported by Watanabe et al
in 1976 (1). Over 80% of gastric
LELCs have been proven to be associated with Epstein-Barr virus
(EBV) infection (2,3). LELC, which has a male predominance and a
favorable prognosis, is usually located in the upper and middle
parts of the stomach. Computed tomography (CT) scan and endoscopic
ultrasound (EUS) may assist in the diagnosis, which is confirmed by
pathology. Since National Comprehensive Cancer Network (NCCN)
guidelines have not been presented seperately for the treatment of
LELC, it is usually treated as gastric adenocarcinoma. The aim of
this report was to describe in detail this rare variant of gastric
cancer and discuss its clinical characteristics and treatment.
Case report
A 41-year-old female patient presented with
epigastric discomfort and general fatigue in April, 2014. A
gastroscopy revealed a sizeable ulcer on the lesser curvature and
posterior wall of the upper gastric body, with irregular borders,
mucosal sclerosis and hemorrhagic tendency. Following biopsy and
histological examination, the lesion was diagnosed as poorly
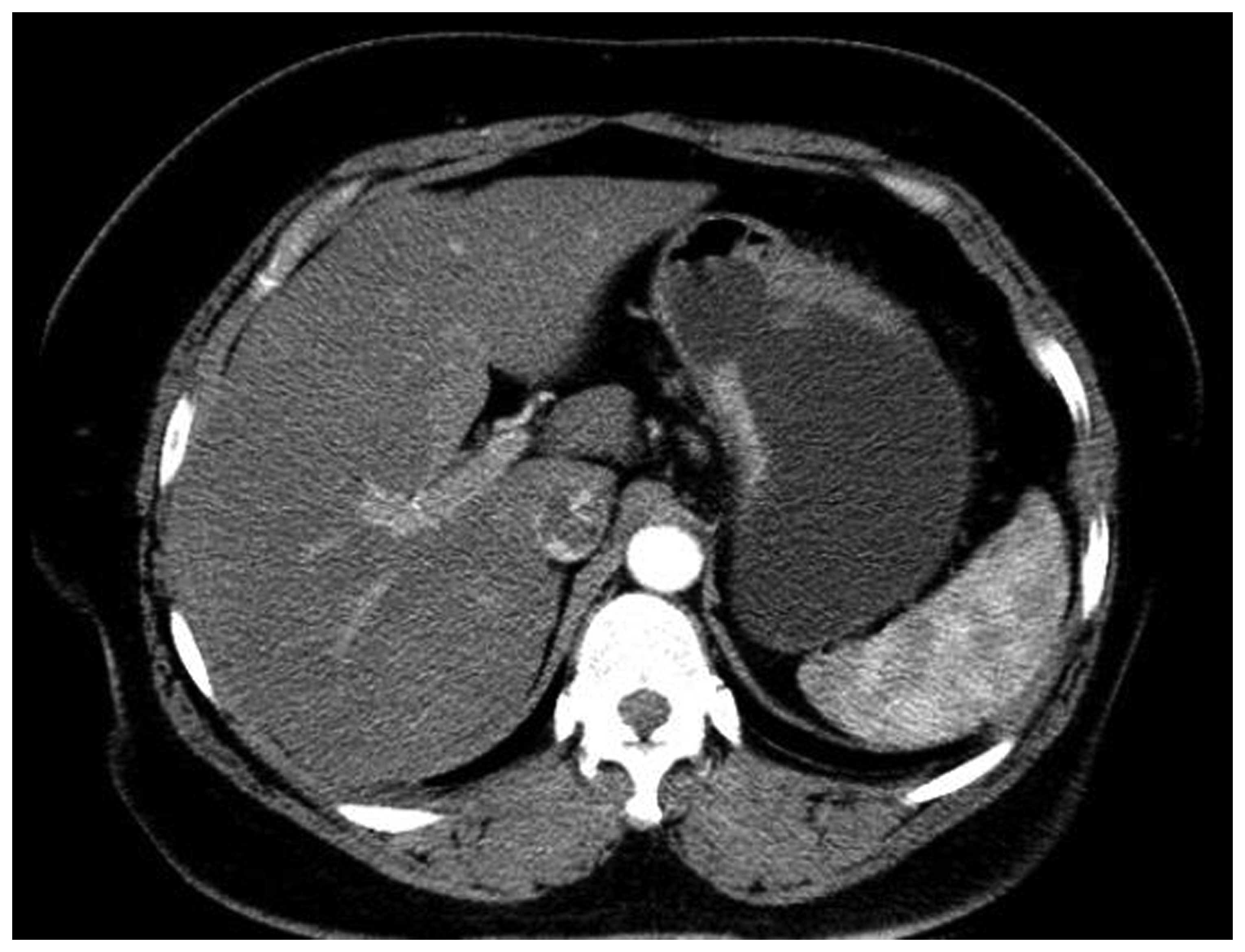
differentiated gastric adenocarcinoma. The CT scan revealed
thickening of the wall in part of the gastric body (Fig. 1). Based on these findings and
considering the patient's age and general condition, a radical
gastrectomy was performed with lymph node dissection and Roux-en-Y
reconstruction.
The gross examination of the gastrectomy specimen
revealed a tumor measuring 3×2.5×1 cm with a sizeable ulcer on the
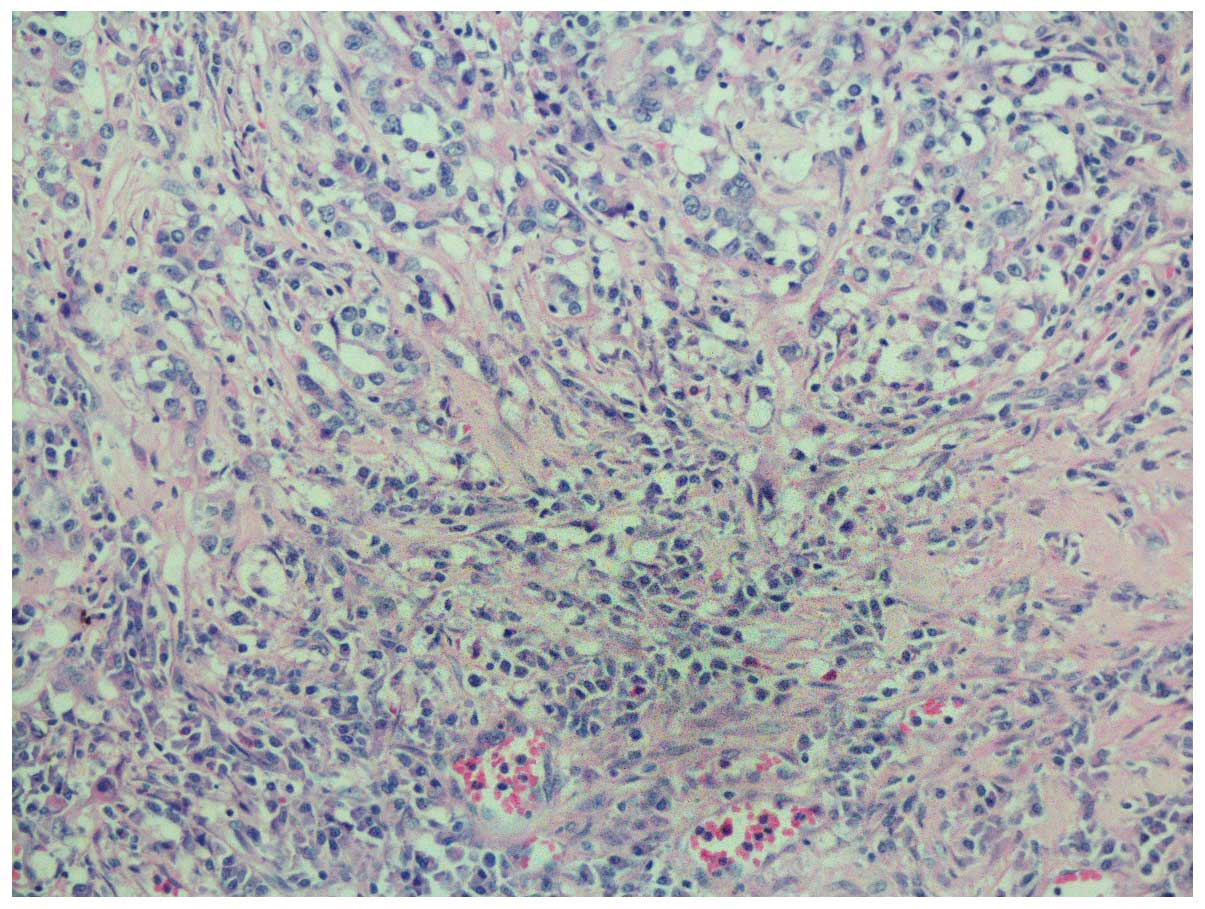
lesser curvature of the gastric body. The pathological examination
revealed that the tumor consisted of nests of neoplastic cells
within a dense lymphoid stromal infiltration (lymphoepitheloid
carcinoma). Furthermore, the tumor invaded the muscular layer of
the gastric wall, with nerve involvement, but without intravascular
cancer emboli. The surgical margins were cancer-free and 2 of the
27 dissected lymph nodes at the lesser curvature were metastatic.
The peritumoral gastric mucosa revealed mild chronic atrophic
gastritis with intestinal metaplasia (Fig. 2).
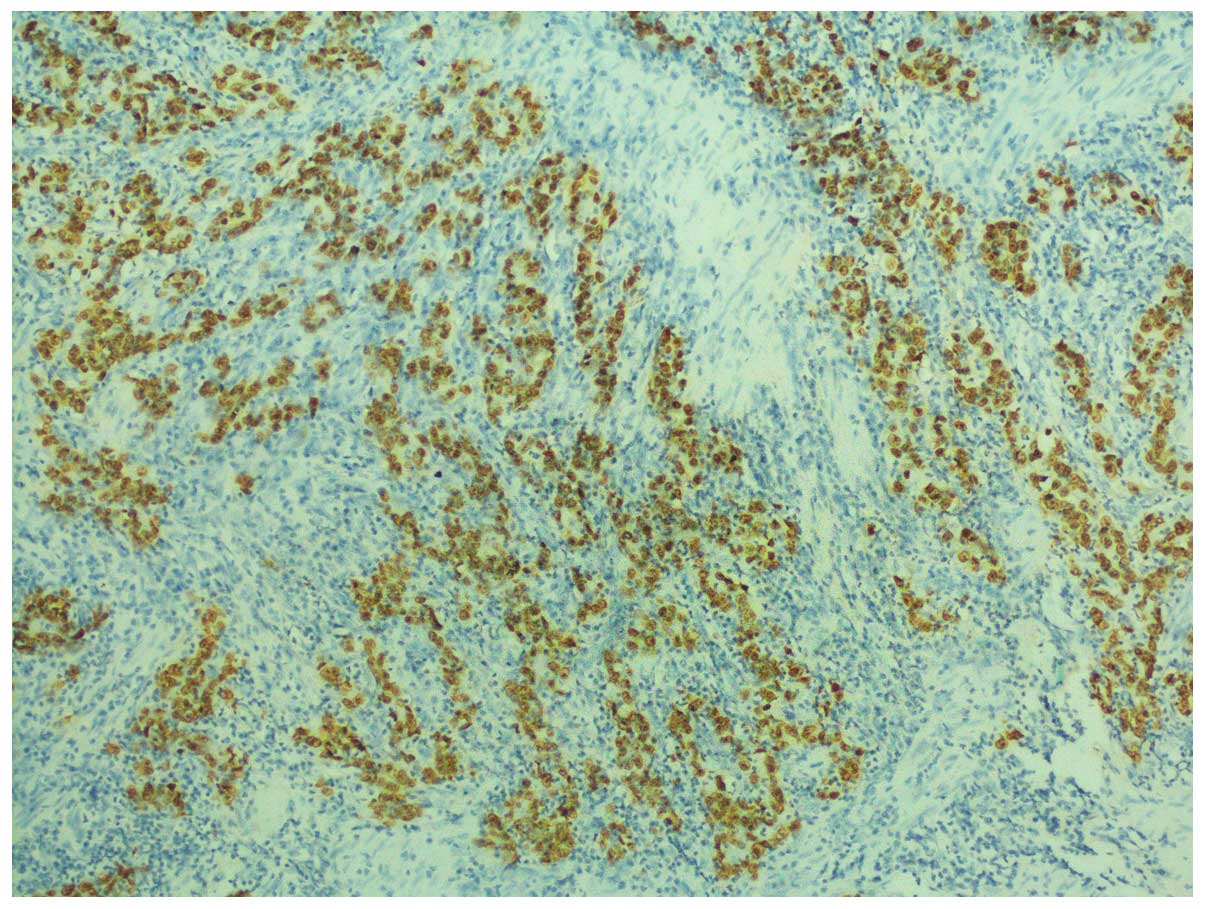
On immunohistochemistry, the tumor cells were
positive for human epidermal growth factor receptor 2 and
E-cadherin, with a Ki-67 index of 60%, but negative for CD133,
epidermal growth factor receptor (EGFR), vascular EGFR2 and c-Met.
In situ hybridization (ISH) confirmed Epstein-Barr encoding
region (EBER) positivity (Fig.
3).
Finally, EBV-associated LELC of the stomach was
diagnosed and staged as IIA (T2, N1, cM0) according to the NCCN
guidelines, 2015 (http://www.nccn.org/professionals/drug_compendium/content/changes_archive.asp?Panel_ID=40).
The patient received postoperative adjuvant
chemotherapy [5-fluorouracil 1.8 g/m2 as a 24-h
continuous intravenous infusion + oxaliplatin 85 mg/m2
volume of distribution (VD) on day 1 + leucovorin 100
mg/m2 VD on day 1], without disease recurrence or
metastasis during the 1 year follow-up after her initial
diagnosis.
Discussion
EBV is a lymphotropic virus consisting of 184
kbp-sized double-stranded DNA, which belongs to the
Herpesviridae family and infects >90% of adults
worldwide. EBV is closely associated with a wide range of human
lymphoid and epithelial malignancies, including Burkitt's lymphoma,
Hodgkin lymphoma, undifferentiated nasopharyngeal carcinoma (NPC)
and EBV-associated gastric carcinoma (EBVaGC) (3). Furthermore, EBV has been isolated from
various anatomic sites, including the salivary glands, thymus,
larynx, lung, esophagus, uterine cervix, urinary bladder and skin
(4).
EBVaGC is identified by the presence of EBV latent
infection in neoplastic cells and its absence from normal
epithelium or dysplastic lesions. Histopathologically, EBVaGC has
two subtypes, namely LELC and ordinary adenocarcinoma (ordinary
EBVaGC) (5). Gastric LELC consists of
two subsets, namely EBV-positive and microsatellite instability
(MSI)-high carcinomas (6,7). As a rare form of gastric carcinoma, LELC
was first reported as ‘gastric cancer with a lymphoid stroma’ by
Watanabe et al in 1976, and was first demonstrated to be
associated with EBV in a study published in 1990 (2).
The frequency of EBV infection in gastric carcinoma
ranges from 2 to 20%, with a worldwide mean frequency of ~10%
(8,9).
However, due to geographical and environmental factors, the
reported frequencies may differ. According to a meta-analysis
published in 2009, the estimate of EBV positivity in gastric cancer
is 8.7% (95% confidence interval: 7.5–10.0%) overall, and the
frequencies are not statistically different among regions (9.9% for
American, 8.3% for Asian and 9.2% for European cases). In addition,
~15–25% of EBVaGCs exhibit the lymphoepithelioma-like pattern,
whereas 86–91% of LELCs are EBV-positive (10,11),
suggesting that EBV infection, although not the sole cause, is
closely associated with gastric LELC. The prevalence of MSI-high
carcinoma in gastric LELC ranges from 7 to 39%, with apparent
geographic variability (6). Among the
annual incidence of 951,600 gastric cancer cases worldwide
(12), the patients who develop
gastric LELC are estimated to be 9, 516–38,064/year.
LELC has distinct clinical characteristics that
distinguish it from ordinary gastric adenocarcinoma. LELC exhibits
a male predominance and is usually located in the proximal stomach.
It was previousy reported that this type of cancer occurs in
relatively younger patients, although the opposite observation has
also been reported (10,11). LELC often presents as an ulcerated or
saucer-like tumor accompanied by marked thickening of the gastric
wall. These characteristics may be well discernible on CT and EUS.
In a CT study including 13 EBV-associated gastric carcinomas, the
authors concluded that the carcinomas were generally located in the
upper gastric region, with a large thickness-to-width ratio, or
presented as a bulky mass projecting from the wall. However,
gastric LELC had various CT appearances, including focal mucosal
thickening, marked thickening of the wall with contrast
enhancement, and bulky mass formation (13). It is difficult to distinguish LELCs
presenting as a bulging mass from lymphomas, gastrointestinal
stromal tumors, neurogenic tumors and glomus tumors by imaging
alone. A comparison with the clinical findings of gastroscopy and
pathology was recommended. EUS may easily detect the nodules of
lymphoid stromal infiltration in the submucosa as a hypoechoic mass
in the hyperechoic third layer (14).
EBER-ISH has been used as a gold standard to identify
EBV-associated gastric cancer (3,15). The
differential diagnosis of gastric LELC includes neuroendocrine
tumors, malignant melanoma, intense lymphoid infiltrate alone, or
even lymphoma.
In recent years, significant progress has been made
in the multimodality treatment of gastric adenocarcinoma,
particularly in terms of novel chemotherapeutic agents, novel
targeted therapies and radiotherapy. However, the optimal treatment
for gastric LELC remains unknown. Due to the rare occurrence of
LELC, there are no specific NCCN guidelines for its treatment
alone; thus, it is usually treated as gastric adenocarcinoma. Since
the tumor boundaries are often well-defined and the majority of the
patients are at a relatively early clinical stage, endoscopic
submucosal dissection or surgical resection remains the mainstay of
treatment. Nasopharyngeal LELC is highly sensitive to radiotherapy,
which has become the main therapeutic approach. Although gastric
LELC shares similar histological characteristics to
undifferentiated NPC, its sensitivity to radiotherapy has not been
reported. However, abdominal radiotherapy is difficult to target
accurately and is associated with a relatively high complication
rate.
Therapeutic approaches require further research on
virus-host interactions in EBV-associated neoplasms (16). Since viral replication is inhibited by
promoter methylation in EBV DNA, demethylating agents, such as
5-azacytidine, may induce lytic infection by EBV, leading to lysis
of infected cells (17). The approach
has particular merits in EBV-associated gastric cancer, in which
methylation of the tumor suppressor gene is also a key abnormality.
However, the efficiency of drug delivery and the side effects of
demethylating agents require further investigation. Since most
gastric LELCs contain the EBV oncoproteins, and cancer-driving
viral antigens are highly attractive therapeutic targets,
therapeutic vaccines targeting the EBV oncoproteins may prove to be
beneficial. Furthermore, adoptive T-cell therapy is emerging as a
promising cancer treatment, and one recently published study
demonstrated that durable, complete regression of metastatic
cervical cancer may occur after a single infusion of HPV-targeted
tumor-infiltrating lymphocytes (TILs) (18). Hence, we must investigate whether an
infusion of EBV-targeted TILs may induce cancer regression in
patients with gastric LELC. Another novel finding, which is
characteristic of EBVaGC, was recurrent amplification at 9p24.1 at
the locus that includes Janus kinase 2, programmed death-ligand 1
(PD-L1) and PD-L2. Blocking the interaction between PD-1 and
PD-L1/L2 may augment the antitumor immune response and clinical
trials investigating the efficacy of immunotherapy by targeting
these molecules are under way (19–21).
LELC has a relatively favorable prognosis. Tak et
al (22) compared the clinical
characteristics and prognostic factors between gastric LELC and
gastric adenocarcinoma, and found that postoperative recurrence or
metastasis tended to occur less frequently in gastric LELC compared
with poorly-differentiated gastric adenocarcinoma. Among prognostic
factors, only the number of lymph node metastases exhibited a
significant difference, with gastric LELC being associated with a
smaller number of lymph node metastases. The disease-free and
overall survival rates of gastric LELC were higher compared with
those of poorly-differentiated gastric adenocarcinoma. Park et
al (23) demonstrated that age,
histological type, Lauren classification, tumor location, depth of
invasion, lymph node metastasis and venous invasion were
independent prognostic factors, whereas the LELC type was not. The
5-year survival rate of the LELC group (97.7%) was better compared
with that of the non-LELC group (89.4%). Kim et al (24) reached the same conclusion by
investigating the clinicopathological characteristics and prognosis
of LELC, signet ring cell, mucinous and papillary carcinomas in
cases with advanced gastric cancer.
Gastric LELC is a distinct subtype of gastric
carcinoma with regard to its clinical characteristics. LELC
generally has a better prognosis compared with other types of
EBV-associated gastric carcinomas and conventional gastric
carcinomas. Pathologists and clinicians should take into
consideration this subset of gastric cancer to make an accurate
diagnosis and select the appropriate treatment.
References
|
1
|
Watanabe H, Enjoji M and Imai T: Gastric
carcinoma with lymphoid stroma. Histopathology. Cancer. 38:232–243.
1976. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Burke AP, Yen TS, Shekitka KM and Sobin
LH: Lymphoepithelial carcinoma of the stomach with Epstein-Barr
virus demonstrated by polymerase chain reaction. Mod Pathol.
3:377–380. 1990.PubMed/NCBI
|
|
3
|
Shinozaki-Ushiku A, Kunita A and Fukayama
M: Update on Epstein-Barr virus and gastric cancer (Review). Int J
Oncol. 46:1421–1434. 2015.PubMed/NCBI
|
|
4
|
Cheng N, Hui DY, Liu Y, Zhang NN, Jiang Y,
Han J, Li HG, Ding YG, Du H, Chen JN and Shao CK: Is gastric
lymphoepithelioma-like carcinoma a special subtype of
EBV-associated gastric carcinoma? New insight based on
clinicopathological features and EBV genome polymorphisms. Gastric
Cancer. 18:246–255. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fukayama M and Ushiku T: Epstein-Barr
virus-associated gastric carcinoma. Pathol Res Pract. 207:529–537.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Grogg KL, Lohse CM, Pankratz VS, Halling
KC and Smyrk TC: Lymphocyte-rich gastric cancer, Associations with
Epstein-Barr virus, microsatellite instability, histology, and
survival. Mod Pathol. 16:641–651. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bittar Z, Fend F and Quintanilla-Martinez
L: Lymphoepithelioma-like carcinoma of the stomach A case report
and review of the literature. Diagn Pathol. 8:1842013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fukayama M: Epstein-Barr virus and gastric
carcinoma. Jpn J Clin Med. 70:1715–1719. 2012.(In Japanese).
|
|
9
|
Chen JN, He D, Tang F and Shao CK:
Epstein-Barr virus-associated gastric carcinoma, A newly defined
entity. J Clin Gastroenterol. 46:262–271. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Murphy G, Pfeiffer R, Camargo MC and
Rabkin CS: Meta-analysis shows that prevalence of Epstein-Barr
virus-positive gastric cancer differs based on sex and anatomic
location. Gastroenterology. 137:824–833. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lee JH, Kim SH, Han SH, An JS, Lee ES and
Kim YS: Clinicopathological and molecular characteristics of
Epstein-Barr virus-associated gastric carcinoma, A meta-analysis. J
Gastroenterol Hepatol. 24:354–365. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Maeda E, Akahane M, Uozaki H, Kato N,
Hayashi N, Fukayama M and Ohtomo K: CT appearance of Epstein-Barr
virus-associated gastric carcinoma. Abdom Imaging. 34:618–625.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bai Y, Gao Q, Ren G, Wang B and Xiang H:
Epstein-Barr virus-associated lymphoepithelioma-like gastric
carcinoma located on gastric high body, Two case reports. Indian J
Pathol Microbiol. 57:463–466. 2014.PubMed/NCBI
|
|
15
|
Uozaki H and Fukayama M: Epstein-Barr
virus and gastric carcinoma - viral carcinogenesis through
epigenetic mechanisms. Int J Clin Exp Pathol. 1:198–216.
2008.PubMed/NCBI
|
|
16
|
Fu DX, Tanhehco Y, Chen J, Foss CA, Fox
JJ, Chong JM, Hobbs RF, Fukayama M, Sgouros G, Kowalski J, et al:
Bortezomib-induced enzyme-targeted radiation therapy in
herpesvirus-associated tumors. Nat Med. 14:1118–1122. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jung EJ, Lee YM, Lee BL, Chang MS and Kim
WH: Lytic induction and apoptosis of Epstein-Barr virus-associated
gastric cancer cell line with epigenetic modifiers and ganciclovir.
Cancer Lett. 247:77–83. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Stevanović S, Draper LM, Langhan MM,
Campbell TE, Kwong ML, Wunderlich JR, Dudley ME, Yang JC, Sherry
RM, Kammula US, et al: Complete regression of metastatic cervical
cancer after treatment with human papillomavirus-targeted
tumor-infiltrating T cells. J Clin Oncol. 33:1543–1550. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Dolan DE and Gupta S: PD-1 pathway
inhibitors: Changing the landscape of cancer immunotherapy. Cancer
Control. 21:231–237. 2014.PubMed/NCBI
|
|
20
|
Naidoo J, Page DB and Wolchok JD: Immune
modulation for cancer therapy. Br J Cancer. 111:2214–2219. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kim SY, Park C, Kim HJ, Park J, Hwang J,
Kim JI, Choi MG, Kim S, Kim KM and Kang MS: Deregulation of immune
response genes in patients with Epstein-Barr virus-associated
gastric cancer and outcomes. Gastroenterology. 148:137–147.e9.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tak DH, Jeong HY, Seong JK, Moon HS and
Kang SH: Comparison of clinical characteristics and prognostic
factors between gastric lymphoepithelioma-like carcinoma and
gastric adenocarcinoma. Korean J Gastroenterol. 62:272–277.
2013.(In Korean). View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Park S, Choi MG, Kim KM, Kim HS, Jung SH,
Lee JH, Noh JH, Sohn TS, Bae JM and Kim S: Lymphoepithelioma-like
carcinoma, A distinct type of gastric cancer. J Surg Res.
194:458–463. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kim KH, Kim MC, Jung GJ and Kim SJ: The
differences in clinicopathological features and prognosis among the
subtypes of signet ring cell, mucinous, papillary, and
lymphoepithelioma-like carcinoma in advanced gastric cancer.
Hepatogastroenterology. 61:2149–2155. 2014.PubMed/NCBI
|