Introduction
Intravenous leiomyomatosis (IVL) is a rare tumor,
which is usually of uterine origin. Birch-Hirschfeld (1) first described this disease in 1896, and
following its discovery, Dürck (2)
reported IVL with right atrium extension in the autopsy. This tumor
type is characterized by intravascular nodular masses of
histologically benign smooth muscle that may extend variable
distances, including into the inferior vena cava, right atrium and
pulmonary arteries. The tumor may arise from uterine leiomyoma,
walls of uterine vessels, or myometrium. The age of presentation is
usually between 20 and 70 years, with a mediun age of 45 years. The
most commonly affected women are pre-menopausal and multiparous.
Intracardiac extension may represent a diagnostic challenge, as it
is usually misdiagnosed as a right atrial myxoma and may cause
multiple symptoms, including shortness of breath, tachycardia,
chest pain, syncope and even mortality. The present study reported
two separate cases of IVL resected at the General Hospital of
Shenyang Military Command.
Case report
Case 1
A 60-year-old female was admitted to General
Hospital of Shenyang Military Command due to a right atrium
neoplasm identified during examination. A hysteromyomectomy for
uterine fibroids was performed 41 years ago. Following the
operation, the patient stopped menstruating. The patient was
pregnant twice, however, only gave birth to one child. An
echocardiogram revealed a neoplasm in the inferior vena cava and
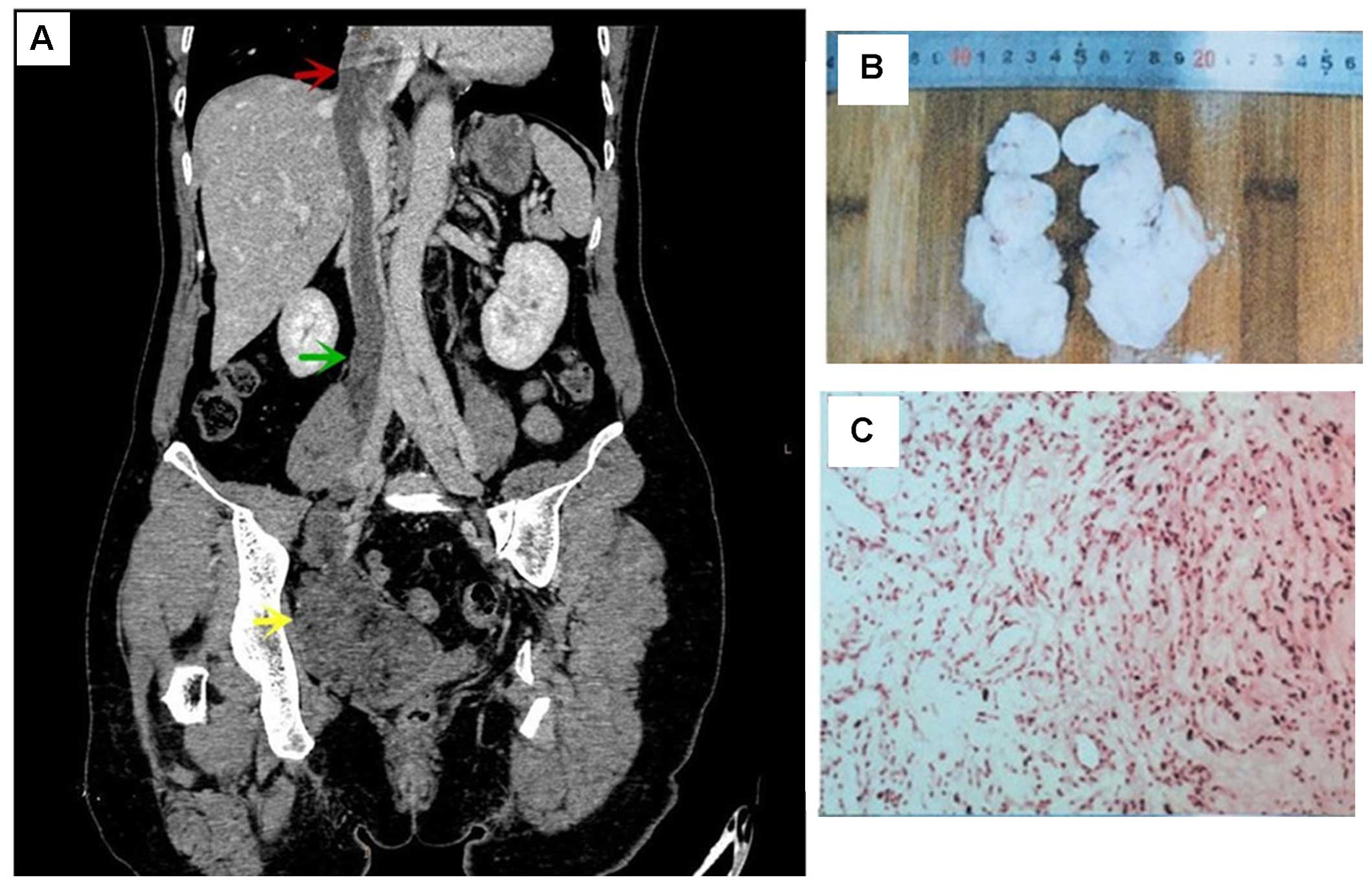
right atrium. Computed tomography (CT) revealed a neoplasm in the
right pelvic cavity, which had invaded into vena iliaca interna,
common iliac vein and inferior vena cava, finally reaching into
right atrium. The neoplasm was round-like in the right atrium
(Fig. 1A). The tumor spread via the
vein system and was shown low density in the vein system. Following
surgery, gross pathology of two sections of smooth grey white mass
demonstrated sections of calcification. These masses measured
9.0×4.5×3.0 cm (Fig. 1B). Following
surgery, microscopy revealed a muscle-like cell arranged in a
cord-like formation and shaped as a long fusiform and nucleus
shaped long rod with an abundant blood supply (Fig. 1C). The diagnosis was intravenous
leiomyomatosis (IVL) with right atrium and inferior vena cava
extension. The patient recovered 39 days after surgery.
Regrettably, no follow up was performed.
Case 2
A 49-year-old female presented with frequent chest
pain after activity over the last half-month. A hysteromyomectomy
for uterine fibroids was performed two years ago. The patient
stopped menstruating one year ago. She was pregnant once and gave
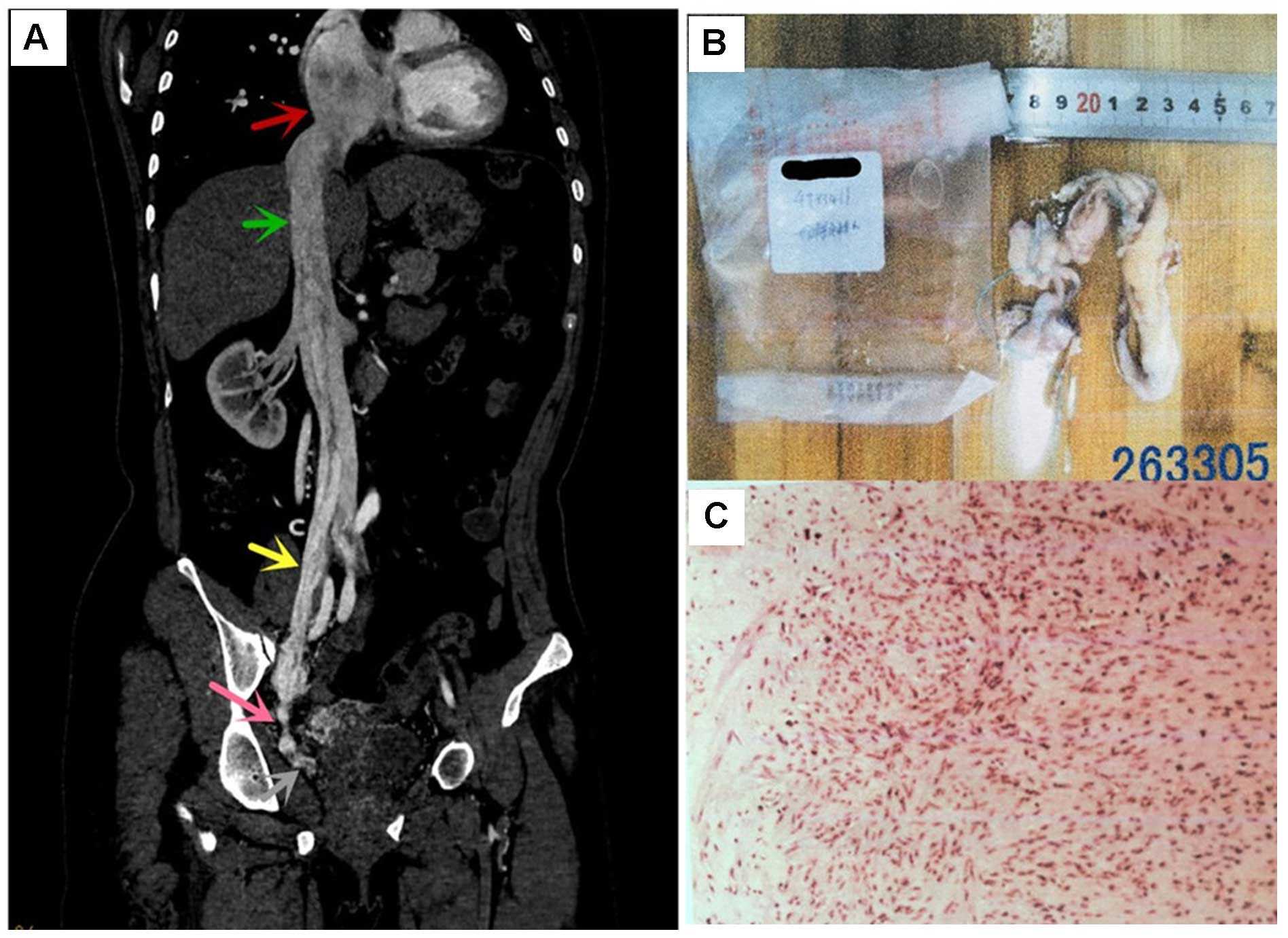
birth to the child. An echocardiogram revealed a neoplasm in the
right atrium. CT revealed a right atrium neoplasm with a smooth
surface, stretched inferior vena cava, vena iliaca interna and vena
iliaca externa (Fig. 2A). Following
surgery, gross pathology was shown in sections of smooth grey white
and grey red masses. One mass measured 9.0×4.5×3.0 cm and the
others measured 4.0×3.5×1.5 cm in total (Fig. 2B). Histology revealed muscle-like
cell arranged in a cord-like formation and shaped as a long
fusiform and nucleus shaped long rod (Fig. 2C). The diagnosis was IVL with right
atrium and inferior vena cava extension. The patient recovered 28
days later. Regrettably, no follow up was performed.
Discussion
The symptoms of IVL are atypical and have no
specialty; therefore, it is often clinically misdiagnosed. Clinical
features included pelvic mass, irregular uterus enlargement and
bleeding in the vagina, menstruation variation, abdominal
distension, and pelvic cavity compression. Before the tumor
spreading via the inferior vena cava, all clinical symptoms were
hidden and led to misdiagnosis by physicians. However, when the
tumor extended to the right atrium, this caused palpitation, chest
pain, discontinuous syncope, sudden mortality and even pulmonary
transfer (3).
IVL is a rare disease and the CT features of IVL
were unique, particularly in cases of mass with heart extension. At
an early stage, contrast-enhanced CT and CT vein (CTV) imaging can
distinguish IVL. In non-contrast-enhanced CT images, a mass
consisting of an isodense lesion was revealed in the vein and heart
lumen; and an off-centered filling-defect was revealed in the vein
and heart lumen. The mass was dissociated in the lumen with low
density and medium heterogeneous enhancement in the
contrast-enhanced CT image. The involved the thickening and
extension of the vein system in the lumen (4,5). CTV
imaging revealed the mass, which performed vascular reconstruction
more accurately and directly. The CTV image confirmed the
correlation between the tumor and other viscera vessels, collateral
vessels, which was significant for pre-operation evaluation and
operation strategy.
For IVL with right atrium extension, differential
diagnosis includes vascular thrombus, as well as primary and
metastatic tumor types. Vascular thrombus was always without
enhancement in the contrasted CT scanning. Metastatic differential
diagnosis includes metastasis with IVC invasion (e.g. renal cell
carcinoma, adrenal cortical carcinoma, hepatocellular carcinoma and
lymphoma), atrial myxoma, right-sided heart thrombus or embolus,
and leiomyosarcoma. Atrial myxoma is usually the initial diagnosis
in these patients given that it is the most common primary heart
tumor. However, 60–75% of atrial myxomas are located in the left
atrium attached to atrial septum, usually at the fossa ovalis, and
no IVC extension exists unless it arises from the IVC proper (in
extremely rare cases) (6,7). Another diagnosis to consider is benign
metastasizing leiomyomas (BML). This disease is characterized by
uterine leiomyoma in young adulthood, with pulmonary metastasis
occurring in the pre-menopausal period (8).
Treatment of IVL is almost always surgical (9–11), which
includes excision of the extra-uterine tumor and myomectomy, or
total hysterectomy, as necessary. The tumor usually spreads via the
veins. Therefore, once intravenous leiomyomatosis was suspected,
the vein system must be assessed completely and the tumor was
excised as completely as possible. As for patients where resection
is not possible or where the tumor remains, anti-estrogen treatment
was a good choice. Anti-estrogen existed in uterine vascular
leiomyoma. The level of estrogen in the uterine vascular leiomyoma
was 10-times higher compared with healthy tissue. Kokawa et
al (12) suggested that higher
estrogen and estrogen receptor levels may influence the growth and
invasion of the tumor.
In the present study, IVL, a rare diagnosis that
merits consideration in young pre-menopausal or old post-menopausal
female patients with cardiac symptoms associated with a right
atrial mass. From the two-presented cases, it was clear that
radiologists serve a vital role in the diagnosis and follow-up of
patients with the diagnosis of IVL. Once patients present with a
uterine or periuterine mass, and deep vein thrombus at the same
time, IVL must be considered. Early detection and correct diagnosis
is imperative for appropriate treatment and surgical planning.
References
|
1
|
Birch-Hirschfeld FV: Lehrbuch der
Pathologischen Anatomie. 5th. F.C.W. Vogel; Leipzig: pp. 2261896,
(In German).
|
|
2
|
Durck H: Ueber ien kontinvierlich durch
die entere holhlvene in das herz vorwachsendes: Fibromyom des
uterus. Munch Med Wochenschr. 54:11541907.(In German).
|
|
3
|
Lam PM, Lo KW, Yu MY, Wong WS, Lau JY,
Arifi AA and Cheung TH: Intravenous leiomyomatosis: Two cases with
different routes of tumor extension. J Vasc Surg. 39:465–469. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Oliveira L and Ramos S: Anesthetic
approach for a clinical case of intravenous leiomyomatosis: Case
report. Braz J Anesthesiol. 63:504–507. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Demirkiran F, Sal V, Kaya U, Alhan C and
Tokgozoqlu N: Intravenous leiomyoma with extension to the heart: A
case report and review of the literature. Case Rep Obstet Gynecol.
2013:6024072013.PubMed/NCBI
|
|
6
|
Grebenc ML, Rosado-de-Christenson ML,
Green CE, Burke AP and Galvin JR: Cardiac myxoma: Imaging features
in 83 patients. Radiographics. 22:673–689. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Buckley O, Madan R, Kwong R, Rybicki FJ
and Hunsaker A: Cardiac masses, part 2: Key imaging features for
diagnosis and surgical planning. AJR Am J Roentgenol.
197:W842–W851. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Awonuga AO, Rotas M, Imudia AN, Choi C and
Khulpateea N: Recurrent benign metastasizing leiomyoma after
hysterectomy and bilateral salpingo-oophorectomy. Arch Gynecol
Obstet. 278:373–376. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sogabe M, Kawahito K, Aizawa K, Sato H and
Misawa Y: Uterine intravenous leiomyomatosis with right ventricular
extension. Ann Thorac Cardiovasc Surg. 20:(Suppl). S933–S936. 2014.
View Article : Google Scholar
|
|
10
|
Kang LQ, Zhang B, Liu BG and Liu FH:
Diagnosis of intravenous leiomyomatosis extending to heart with
emphasis on magnetic resonance imaging. Chin Med J (Engl).
125:33–37. 2012.PubMed/NCBI
|
|
11
|
Clay TD, Dimitriou J, McNally OM, Russell
PA, Newcomb AE and Wilson AM: Intravenous leiomyomatosis with
intracardiac extension-a review of diagnosis and management with an
illustrative case. Surg Oncol. 22:e44–e52. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kokawa K, Yamoto M, Yata C, Mabuchi Y and
Umesaki N: Postmenopausal intravenous leiomyomatosis with high
levels of estradiol and estrogen receptor. Obstet Gynecol.
100:1124–1126. 2002. View Article : Google Scholar : PubMed/NCBI
|