Introduction
Gallbladder perforation (GBP) represents a rare, but
potentially life-threatening, complication of acute cholecystitis,
with an incidence rate of 0.8–4.8% and a mortality rate of 9.5–16%
as reported in recent studies (1–4). The
proposed mechanism of GBP is gallbladder wall ischemia and necrosis
triggered by intense inflammatory reaction, and intracholecystic
hypertension caused by calculi impacted in the cystic duct
(5). Acute abdominal pain
accompanied by fever or nausea and vomiting portends the onset of
perforation. However, clinical discrimination from uncomplicated
acute cholecystitis is difficult due to overlapping signs and
symptoms, leading to a delay in diagnosis and poor results
(3,6). Radiological evaluations serve a vital
role in early identification and appropriate intervention. Although
focal disruption of the wall is the definitive imaging finding of
GBP, small perforations may escape detection, and preoperative
diagnosis therefore remains challenging (7).
Based on the clinicopathological findings of
Niemeier in 1934 (8), GBP is
subdivided into three categories: Type I presents an acute status
with generalized biliary peritonitis; type II is characterized as a
subacute stage with abscess formation and localized peritonitis;
and type III is a chronic procedure, with the development of
fistula between gallbladder and another viscus. Subacute
perforation is the most common type, followed by acute and chronic
perforations, whereas the development of biloma is extremely rare
(5,9).
In the present study, a case of a giant and
asymptomatic subphrenic biloma formation secondary to GBP without
visualized defects, and mimicking a biliary cystic tumor, is
reported.
Case report
In December 2015, a 40-year-old man with a 10-year
history of calculus cholecystitis was referred to The First
Affiliated Hospital of Nanjing Medical University (Nanjing, China)
for surgical treatment of an emerging massive subphrenic entity
without abdominal pain, fever, jaundice, nausea or omitting. The
patient had been admitted to the local hospital two months earlier
for conservative treatment of an acute attack of chronic
cholecystitis. An initial computed tomography (CT) scan was
unremarkable, apart from calculus cholecystitis. The patient's
medical history was negative for abdominal trauma and surgery.
An abdominal examination revealed a palpable hard
mass in the right upper quadrant (RUQ) without tenderness. Abnormal
laboratory findings included mild elevation of total and direct
bilirubins (1.7 and 0.8 mg/dl, respectively), alkaline phosphatase
(199.3 U/l) and γ-glutamyltransferase (98.6 U/l). Levels of
peripheral blood count (white blood cell count,
5.42×109/l; neutrophils, 57%; hemoglobin, 144 g/l;
platelet count, 187×109/l), liver enzymes (aspartate
transaminase, 31.3 U/l; alanine transaminase, 34.5 U/l) and tumor
markers (carcinoembryonic antigen, 1.1 ng/ml; α-fetoprotein, 4.0
ng/ml; carbohydrate antigen 19–9, 0.7 U/ml) were all within normal
limits.
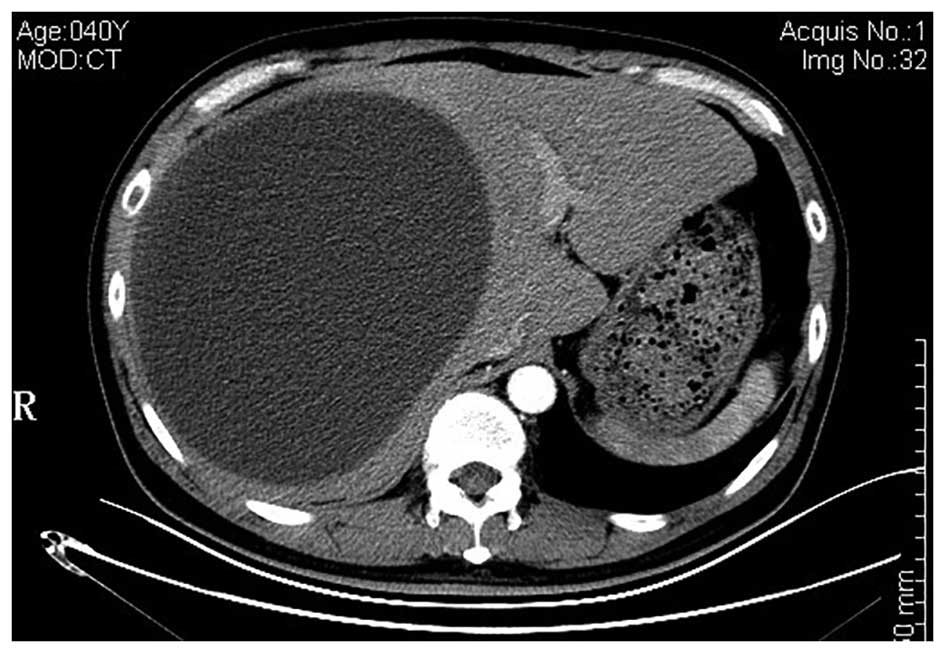
A repeat CT scan revealed a well-circumscribed,
hepatic cystic lesion, measuring approximately 20.4×15.4 cm,
without enhancement (Fig. 1).
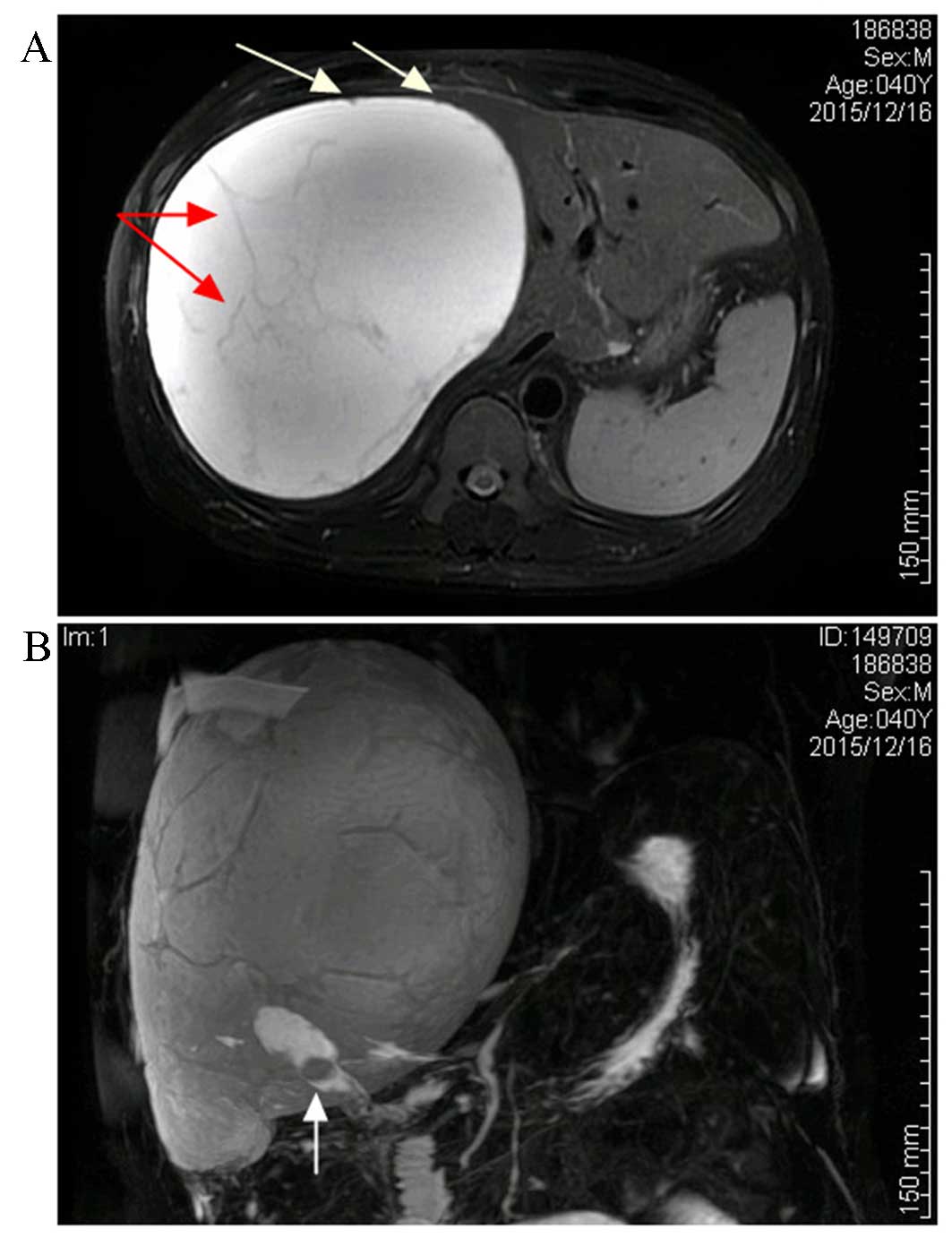
Magnetic resonance imaging (MRI) revealed a hepatic mass that was
revealed by a homogenously iso-intensity signal on a T1-weighted
image, with hyper-intensity and also several iso-intensity
septations and small mural nodules on a T2-weighted image (Fig. 2A). Magnetic resonance
cholangiopancreatography (MRCP) demonstrated the gallstones and
subphrenic collection, without any visible communication with the
biliary system (Fig. 2B).
A biliary cystic tumor (BCT), particularly
cystadenocarcinoma, was highly suspected, based on the intracystic
septations and mural nodules that were demonstrated on the MR
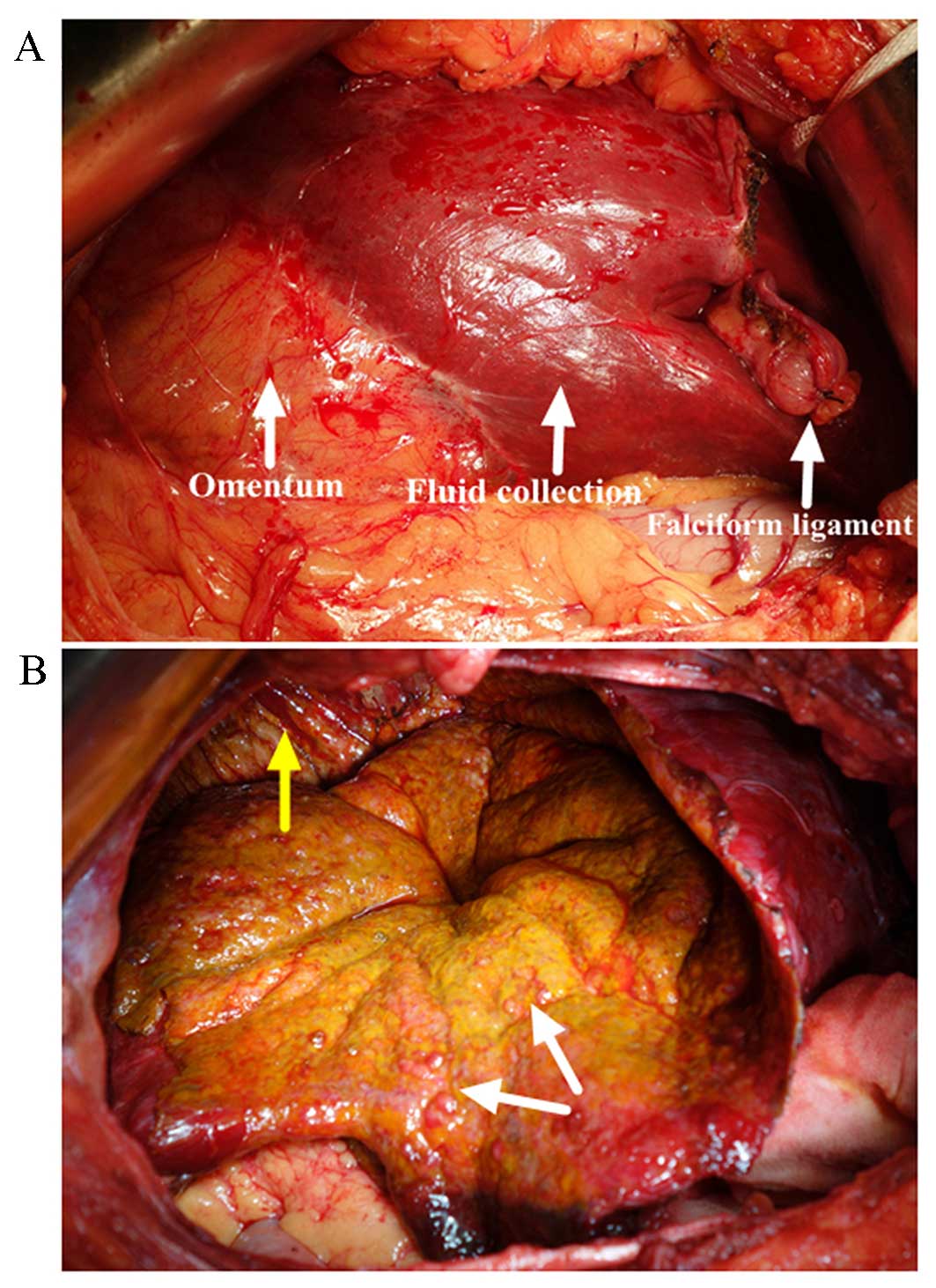
images. Therefore, a laparotomy was performed, and an
intraoperative examination revealed that the greater omentum had
adhered to the undersurface of the entity and gallbladder densely
(Fig. 3A). Approximately 4,000 ml
dark-yellow fluid was aspirated, and the lumen was scattered with
papillae (Fig. 3B). Given the
suspected BCT and its malignant potential, a frozen section
examination was performed at the time of performing the
fenestration, which illustrated a simple hepatic cyst. The cyst
wall was peeled off from the hepatic capsule and the right
diaphragm with ease following cholecystectomy. Histopathology of
the gallbladder illustrated an ulcerative episode of a
chronic-recurring calculus cholecystitis with focal granulation
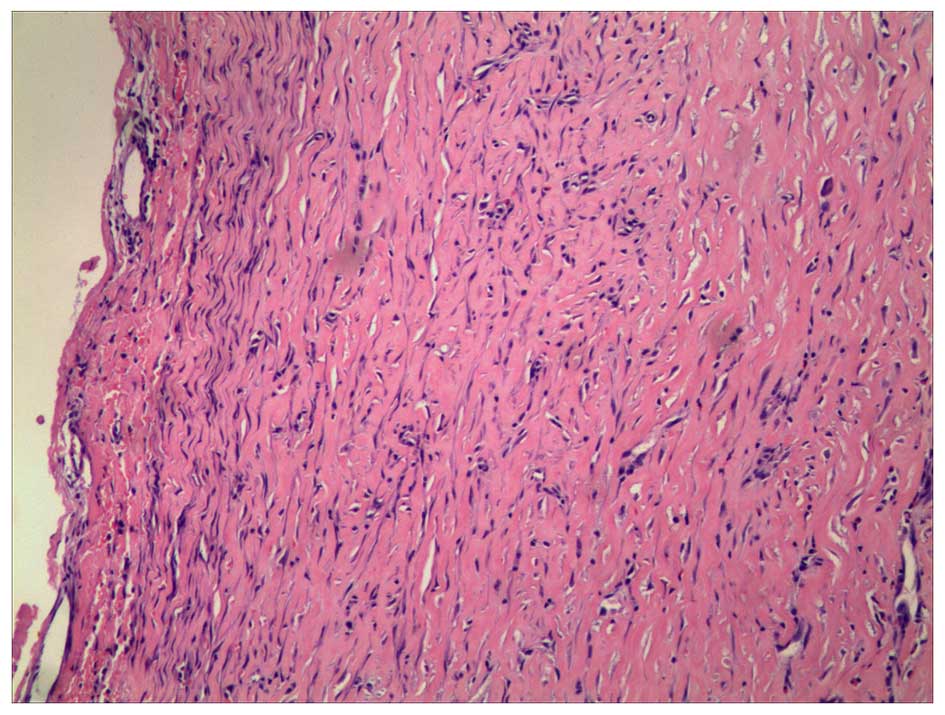
tissue formation. Microscopically, the wall was made up of fibrous
tissue without epithelial lining, which indicated that the fluid
collection produced encapsulation by inducing a mild inflammatory
response and fibrosis (Fig. 4). The
aspiration fluid contained bile (total bilirubin, 8.3 mg/dl), and
was negative on culture, further substantiating the diagnosis of
biloma. The patient had an uneventful postoperative course and was
discharged 7 days after the operation. There was no recollection,
or any other associated complaint after follow-up for 6 months.
Written informed consent was obtained from the
patient for publication of this case report and accompanying
images, and the study was approved by the ethics committee of The
First Affiliated Hospital of Nanjing Medical University (Nanjing,
China).
Discussion
Biloma was first coined by Gould and Patel (10), but was redefined as intra- or
extra-hepatic bile collection outside the biliary tree with
well-demarcated capsule in 1983 by Kuligowska et al
(11). Iatrogenic biliary injury,
particularly cholecystectomy, is the predominant causative factor,
followed by blunt abdominal injury (12,13). In
certain cases, spontaneous biloma formation may occur, and this is
usually associated with bile duct disruption, but rarely with GBP
(13–16). Acute perforation of the gallbladder
generally presents as generalized peritonitis followed by sepsis
syndrome, ascribed to the abrupt release of concentrated bile into
the peritoneal cavity. However, in certain instances, a low-grade
and chronic bile leakage from the gallbladder becomes encapsulated
to form a biloma.
Abdominal discomfort or pain (predominantly in the
RUQ), accompanied by fever, is the most common clinical
presentation of bilomas. Jaundice, nausea and vomiting are often
present as a result of extrinsic compression of the biliary or
digestive system, whereas certain patients may be asymptomatic.
Laboratory findings consist of leukocytosis with neutrophilia and
liver dysfunction, although the values obtained may be
non-specific, and a few patients have no abnormalities at the time
of diagnosis (12).
Abdominal ultrasonography (US) is usually the
initial modality to detect fluid collections, and the underlying
pathology for its non-radiation and accessibility. On US images,
bilomas present as well-circumscribed, anechoic and encapsulated
masses with or without internal debris and septa (7,12).
However, a variety of intraperitoneal cystic lesions have
overlapping features, including hematoma, hepatic cyst, abscess and
pseudocyst. An enhanced CT scan is a sensitive modality to confirm
the collection, as well as for the identification of the
distribution and adjacent anatomy (17), whereas the MRI technique is superior
in delineating the fluid homogeneity and differential diagnosis.
Low-signal intensity within the collection on T2-weighted sequences
indicates the presence of components. MRCP sequences are of value
to depict the course of the biliary system, and the communication
between cystic lesions and bile ducts. CT cholangiography and
cholescintigraphy are non-invasive and effective means of
demonstrating the presence and site of biliary excretion,
complementing the MRCP in selected cases and avoiding the
requirement for endoscopic retrograde cholangiopancreatography or
percutaneous transhepatic cholangiography (18,19). In
exceedingly rare cases, however, a pinhole-sized perforation may
escape detection on medical imaging, even when intraoperative
cholangiography is performed (20).
Multiple imaging modalities and the clinical history
are warranted for the diagnosis of biloma, but the diagnosis is
confirmed by demonstrating a communication with the biliary system
or the biochemical analysis of the fluid collection. Although rare,
BCTs should be suspected for a cystic neoplasm of liver,
particularly with septum-like structures and suspicious intracystic
components, as in our case study (21). However, hematological analysis and
tumor markers are non-specific for distinguishing BCTs from other
hepatic cystic masses (21,22). Given the suspected BCT, image-guided
needle aspiration cytology or biopsy is not implemented, due to
high false negative results and the risk of peritoneal
dissemination (23). Furthermore, an
elevated bilirubin concentration in the aspiration fluid cannot be
considered as a conclusive parameter to discriminate bilomas from
BCTs with bile duct communication (24,25). In
the present case study, intraoperative detection of scattered
papillomas highlighted our suspicion of BCT. Under such
circumstances, a frozen section examination is mandatory to
differentiate benign from malignant lesions, and the definitive
diagnosis should be based on histological examination (26). As such, suspected BCTs should be
treated with surgical resection when feasible.
As for biloma, without timely intervention, the
collection may progress to an infected abscess, and become fatal.
Management of individual patients depends on the etiologies,
symptoms, tumor-associated factors and the medical condition of the
patient. Typically small and asymptomatic bilomas can be monitored
periodically whereas, in cases with large-sized and infected
lesions, or where the patient is medically unfit for surgery,
percutaneous drainage is the appropriate approach, and may suffice
for the evacuation of bilomas. Adjunct therapies, including
percutaneous transhepatic biliary drainage (PTBD) and an endoscopic
technique, are mandatory to facilitate healing of the defect in
persistent cases, and these yield satisfactory results (15,27,28). As
a general rule, endoscopic intervention is responsive for
perforations located distally to the confluence of the left and
right hepatic duct, whereas PTBD is responsive for perforations
located proximally to the confluence. Surgical treatment may be
warranted in cases refractory to minimally invasive management, or
in dealing with the etiology.
There are few reports on biloma formation due to
GBP, but all cases have featured radiological discontinuity of the
gallbladder wall (13,15,16).
Tiny extravasation of unconcentrated bile from the gallbladder and
relatively large subphrenic space should have been responsible for
the insidious symptoms, normal laboratory tests and undetected
perforation site in our patient, and preoperative diagnosis
represented a challenge. To the best of our knowledge, this is the
first report of a giant and asymptomatic subphrenic biloma
formation after calculus cholecystitis without visualized defects
and mimicking a biliary cystic tumor.
In conclusion, GBP is subdivided into three
categories, whereas the formation of biloma is rare, and should be
classified as type IV (13). A
pinhole-sized perforation with extravasation of unconcentrated bile
from the gallbladder may result in insidious clinical presentation
and an undetected leak site. Preoperative differentiation of
bilomas with intracystic septations and mural nodules from BCTs is
difficult, and the definitive diagnosis should be based on
histological analysis of the resected specimen. Laparotomy with a
frozen section examination may be the optimal approach for
discriminating benign from malignant lesions in cases of patients
who are fit for surgery.
Acknowledgements
The present study was supported by the China
Postdoctoral Science Foundation (no. 2015M581837).
Glossary
Abbreviations
Abbreviations:
|
GBP
|
gallbladder perforation
|
|
BCT
|
biliary cystic tumor
|
|
CT
|
computed tomography
|
|
RUQ
|
right upper quadrant
|
|
MRI
|
magnetic resonance imaging
|
|
MRCP
|
magnetic resonance
cholangiopancreatography
|
|
US
|
ultrasonography
|
|
PTBD
|
percutaneous transhepatic biliary
drainage
|
References
|
1
|
Kannan U, Parshad R and Regmi SK: An
unusual presentation of biloma five years following
cholecystectomy: A case report. Cases J. 2:80482009.PubMed/NCBI
|
|
2
|
Göbel T, Kubitz R, Blondin D and
Häussinger D: Intrahepatic type II gall bladder perforation by a
gall stone in a CAPD patient. Eur J Med Res. 16:213–216. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Derici H, Kara C, Bozdag AD, Nazli O,
Tansug T and Akca E: Diagnosis and treatment of gallbladder
perforation. World J Gastroenterol. 12:7832–7836. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ausania F, Suarez S Guzman, Garcia H
Alvarez, Senra del, Rio P and Nuñez E Casal: Gallbladder
perforation: Morbidity, mortality and preoperative risk prediction.
Surg Endosc. 29:955–960. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Seyal AR, Parekh K, Gonzalez-Guindalini
FD, Nikolaidis P, Miller FH and Yaghmai V: Cross-sectional imaging
of perforated gallbladder. Abdom Imaging. 39:853–874. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gunasekaran G, Naik D, Gupta A, Bhandari
V, Kuppusamy M, Kumar G and Chishi NS: Gallbladder perforation: A
single center experience of 32 cases. Korean J Hepatobiliary
Pancreat Surg. 19:6–10. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ohtake T, Kimura M, Yoshii S, Ikegaya N,
Takayanagi S, Hishida A and Kaneko E: Biloma during steroid therapy
for minimal change nephrotic syndrome. Intern Med. 32:543–546.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Niemeier OW: Acute free perforation of the
gall-bladder. Ann Surg. 99:922–924. 1934. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Date RS, Thrumurthy SG, Whiteside S, Umer
MA, Pursnani KG, Ward JB and Mughal MM: Gallbladder perforation:
Case series and systematic review. Int J Surg. 10:63–68. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gould L and Patel A: Ultrasound detection
of extrahepatic encapsulated bile: ‘Biloma’. AJR Am J Roentgenol.
132:1014–1015. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kuligowska E, Schlesinger A, Miller KB,
Lee VW and Grosso D: Bilomas: A new approach to the diagnosis and
treatment. Gastrointest Radio. 8:237–243. 1983. View Article : Google Scholar
|
|
12
|
Copelan A, Bahoura L, Tardy F, Kirsch M,
Sokhandon F and Kapoor B: Etiology, diagnosis, and management of
bilomas: A current update. Tech Vasc Interv Radiol. 18:236–243.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kalfadis S, Ioannidis O, Botsios D and
Lazaridis C: Subcapsular liver biloma due to gallbladder
perforation after acute cholecystitis. J Dig Dis. 12:412–414. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Akhtar MA, Bandyopadhyay D, Montgomery HD
and Mahomed A: Spontaneous idiopathic subcapsular biloma. J
Hepatobiliary Pancreat Surg. 14:579–581. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tsai MC, Chen TH, Chang MH, Chen TY and
Lin CC: Gallbladder perforation with formation of hepatic
subcapsular biloma, treated with endoscopic nasobiliary drainage.
Endoscopy. 42:(Suppl 2). E206–E207. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ferrusquía-Acosta JA, Álvarez-Navascués C
and Rodríguez-García M: Giant biloma as a result of a blunt
abdominal trauma: A case report. Rev Esp Enferm Dig. 107:768–769.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lee CM, Stewart L and Way LW:
Postcholecystectomy abdominal bile collections. Arch Surg.
135:538–544. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ziessman HA: Hepatobiliary scintigraphy in
2014. J Nucl Med. 55:967–975. 2014.PubMed/NCBI
|
|
19
|
Mbarushimana S, Morris-Stiff G and Hassn
A: CT diagnosis of an iatrogenic bile duct injury. BMJ Case Rep.
2014:bcr20142049182014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ishii K, Matsuo K, Seki H, Yasui N, Sakata
M, Shimada A and Matsumoto H: Retroperitoneal Biloma due to
Spontaneous Perforation of the Left Hepatic Duct. Am J Case Rep.
17:264–267. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Doussot A, Gluskin J, Groot-Koerkamp B,
Allen PJ, De Matteo RP, Shia J, Kingham TP, Jarnagin WR, Gerst SR
and D'Angelica MI: The accuracy of pre-operative imaging in the
management of hepatic cysts. HPB (Oxford). 17:889–895. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lee CW, Tsai HI, Lin YS, Wu TH, Yu MC and
Chen MF: Intrahepatic biliary mucinous cystic neoplasms:
Clinicoradiological characteristics and surgical results. BMC
Gastroenterol. 15:672015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Soares KC, Arnaoutakis DJ, Kamel I, Anders
R, Adams RB, Bauer TW and Pawlik TM: Cystic neoplasms of the liver:
Biliary cystadenoma and cystadenocarcinoma. J Am Coll Surg.
218:119–128. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kakisaka T, Kamiyama T, Yokoo H, Nakanishi
K, Wakayama K, Tsuruga Y, Kamachi H, Mitsuhashi T and Taketomi A:
An intraductal papillary neoplasm of the bile duct mimicking a
hemorrhagic hepatic cyst: A case report. World J Surg Oncol.
11:1112013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kishida N, Shinoda M, Masugi Y, Itano O,
Fujii-Nishimura Y, Ueno A, Kitago M, Hibi T, Abe Y, Yagi H, et al:
Cystic tumor of the liver without ovarian-like stroma or bile duct
communication: Two case reports and a review of the literature.
World J Surg Oncol. 12:2292014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Arnaoutakis DJ, Kim Y, Pulitano C,
Zaydfudim V, Squires MH, Kooby D, Groeschl R, Alexandrescu S, Bauer
TW, Bloomston M, et al: Management of biliary cystic tumors: A
multi-institutional analysis of a rare liver tumor. Ann Surg.
261:361–367. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Attasaranya S, Netinasunton N,
Jongboonyanuparp T, Sottisuporn J, Witeerungrot T, Pirathvisuth T
and Ovartlarnporn B: The Spectrum of Endoscopic Ultrasound
Intervention in Biliary Diseases: A Single Center's Experience in
31 Cases. Gastroenterol Res Pract. 2012:6807532012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
de Jong EA, Moelker A, Leertouwer T,
Spronk S, Van Dijk M and van Eijck CH: Percutaneous transhepatic
biliary drainage in patients with postsurgical bile leakage and
nondilated intrahepatic bile ducts. Dig Surg. 30:444–450. 2013.
View Article : Google Scholar : PubMed/NCBI
|