Introduction
Nodular goiter is the most common pathology of the
thyroid gland. The prevalence of goitre nodules may depend on
several factors, such as genes and low iodine intake (1). The majority of focal thyroid lesions are
of a benign nature and the incidence of occult malignancy within a
multinodular goiter ranged between 10 and 35% in the previous
surgical series. The majority of nodular goiter present as an
asymptomatic enlargement of the thyroid gland, or increasing
symptoms of compression (2). As the
thyroid enlarges, it normally extends into the mediastinum as a
result of its anatomical location under the investing layer of the
deep cervical fascia. The present study reported a case of a goiter
with papillary thyroid microcarcinoma, which presented as a
subcutaneous partially cystic with solid areas lesion in the neck
extending over the chest.
Case report
A 76-year-old man of Hui ethnicity presented with
swelling in the front of the neck, which had been present since the
age of 42. The swelling began in the right lobe of the thyroid
region and was initially small in size, however, gradually
increased to the present size. Upon examination, partially cystic
with solid areas swellings extended from the right side of the neck
to the chest wall. The swellings were immobile and failed to move
with deglutition. The cervical lymph nodes were not enlarged
(Fig. 1).
Neck and chest X-rays revealed a markedly increased
soft tissue density in the neck region extending to the upper
sternal region and indenting the trachea (data not shown). An
ultrasound of the neck revealed a disappearance of the normal right
lobe of the thyroid and identified multiple hypoechoic masses with
anechoic areas extending from the level of the carotid to the
mid-sternum (data not shown). Inhomogeneous interior echoes were
observed in the mass (data not shown). The mass on the chest wall
appeared as a low echo mass with a clear margin. The lesion of the
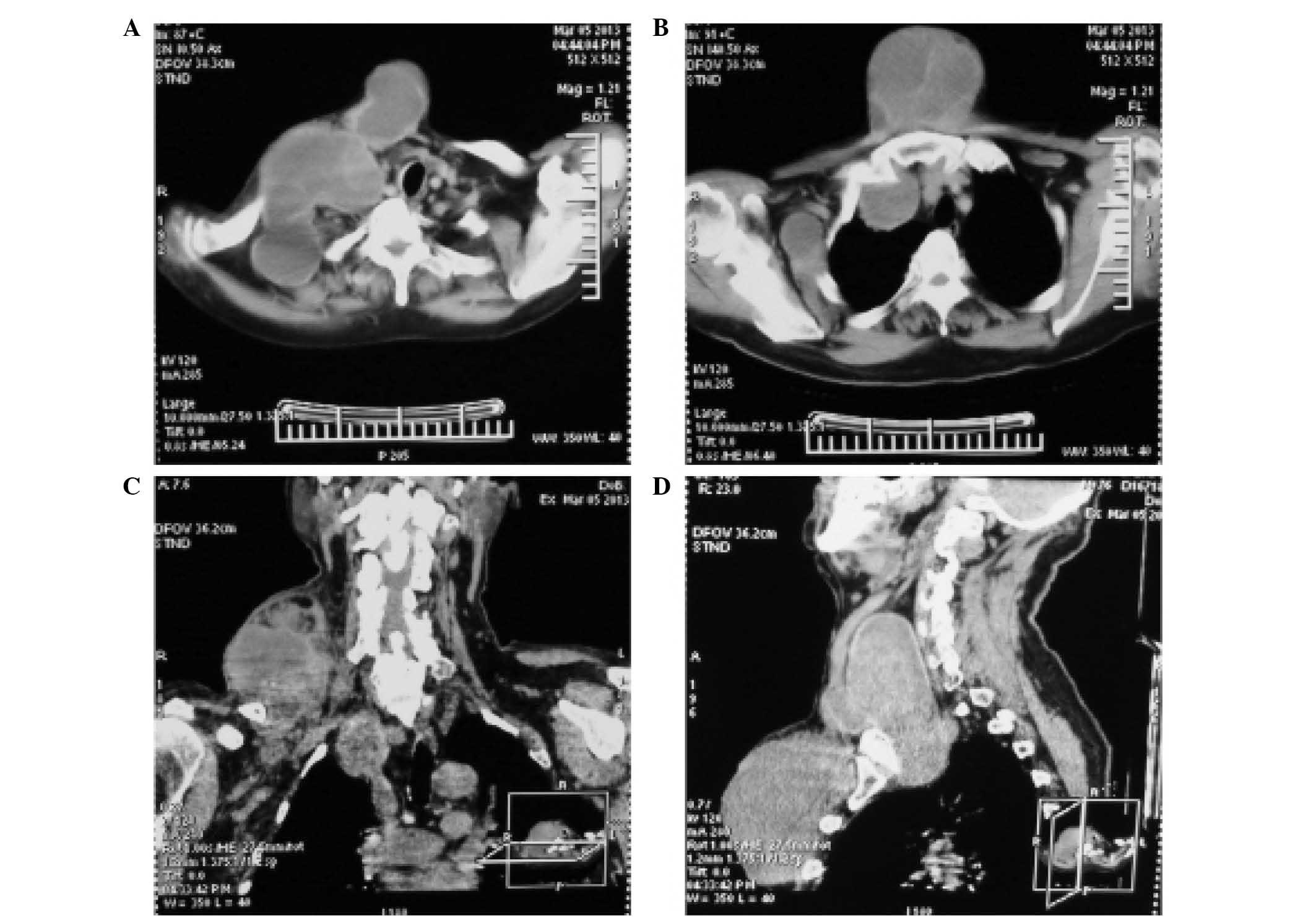
chest wall appeared to arise from thyroid tissue. Computed
tomography revealed multiple coalescing cystic lesions with fluid
attenuation in the subcutaneous plane of the neck and chest wall,
and below the thoracic inlet. The cystic lesions appeared to be
interlinked with the right thyroid lobe and only part of the left
thyroid lobe was visible (Fig.
2).
The patient underwent surgery and under general
anesthesia, an extended Kocher's horizontal fusiform incision was
made over the neck swelling, and the middle part of the incision
was extended vertically downward over the chest wall swelling. The
fluid in the cyst was brown in color. The mass in the right neck
was 15×12 cm in size, ranging up to the jaw, outside to the front
edge of the trapezius, down over the clavicle, and connecting with
the sternum and chest wall mass. On the right side, the mass was
adhered to the internal jugular vein, requiring ligation of the
internal jugular vein. The mass in the chest wall was 17×13 cm and
the substernal goiter descended into the anterior mediastinum. The
maximum length of the part of the mass, which had descended into
the chest was 10 cm. Upon histopathological examination, a
papillary thyroid microcarcinoma with a diameter of 0.2 cm was
identified. The predominant mass was characterized as a
multinodular goiter with hemorrhage, necrosis and cystic change.
The patient recovered completely within 2 weeks following
surgery.
Discussion
The most common benign cervical and chest wall cysts
are lymphangiomas, dermoid cysts, teratomas and inflammatory cysts.
Multinodular goiter progresses from a diffuse enlargement of the
thyroid to a multinodular structure with advancing age. It is very
commonly observed that the long-standing goiter descends into the
upper mediastinum space causing compression of the trachea and
other cervical structures (3). A
paucity of literature addressing thyroid carcinomas, which present
as a chest wall mass, exist (4,5). In
addition, it is extremely rare for a benign multinodular goiter to
present in this way. The present case report suggested that
multinodular goiters may invade adjacent structures and manifest as
malignancies.
Acknowledgements
The present study was supported by a grant from the
Health and family planning commission of Ningxia Hui Autonomous
Region (no. 2013104).
References
|
1
|
Carle A, Krejbjerg A and Laurberg P:
Epidemiology of nodular goitre. Influence of iodine intake. Best
Pract Res Clin Endocrinol Metab. 28:465–479. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nixon IJ and Simo R: The neoplastic
goitre. Curr Opin Otolaryngol Head Neck Surg. 21:143–149. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Silva MN, Rubio IG, Romão R, Gebrin EM,
Buchpiguel C, Tomimori E, Camargo R, Cardia MS and Medeiros-Neto G:
Administration of a single dose of recombinant human thyrotrophin
enhances the efficacy of radioiodine treatment of large compressive
multinodular goitres. Clin Endocrinol (Oxf). 60:300–308. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gertz R, Sarda R and Lloyd R: Follicular
thyroid carcinoma presenting as a massive chest wall tumor. Endocr
Pathol. 24:20–24. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Patil VS, Vijayakumar A and Natikar N:
Unusual presentation of cystic papillary thyroid carcinoma. Case
Rep Endocrinol. 2012:7327152012.PubMed/NCBI
|