Introduction
Intramuscular hematomas represent 10–25% of all
hemorrhagic complications in patients with hemophilia (1). Factor VIII (FVIII) replacement therapy
is crucial to the therapeutic and conservative treatment of
hemorrhagic complications. However, the emergence of FVIII
inhibitors is a major complication in haemophilia. Upon the
occurrence of a hemorrhagic event, subsequent events may become
unpredictable and their management becomes more demanding in
hemophiliac patients with factor VIII inhibitors.
The diagnosis of pelvic pain may also be challenging
in patients with hemophilia. Under such conditions, evaluation
should be based on three main pathological findings: hip
hemarthrosis, iliopsoas hematoma and acute digestive tract illness,
such as appendicitis or diverticulitis. However, rare diagnoses
must be considered. Obturator muscle hematomas are very rarely
encountered. Aouba et al reported two cases of spontaneous
obturator internus muscle hematoma in hemophilia, which is the only
publication regarding obturator muscle hematomas in the literature
(2). To the best of our knowledge,
cases of obturator externus muscle hematoma in the context of
hemophilia have not been published to date. We herein report a case
of spontaneous bleeding of the bilateral obturator externus
muscles, which occurred three times within a period of 9 months in
a hemophilia patient with factor VIII inhibitors. The most
frequently published cases involving the obturator muscles are
primary pyomyositis or intramuscular abscess (3–6). We also
underline the possibility of underdiagnosing obturator muscle
hematoma with ultrasonography, which requires more advanced imaging
modalities, such as magnetic resonance imaging (MRI) or computed
tomography (CT).
Case report
A 22-year-old male patient diagnosed with
haemophilia A (FVIII <1%) with high responding inhibitors (6.4
BU) for 2 years, was admitted to our emergency department with left
hip, groin and thigh pain, extending to the pubic area. At rest,
the patient maintained his hip in mild flexion, whereas movement
resulted in pain and muscular spasm. The psoas test was within
normal limits. The findings on examination of other joints,
cardiovascular and respiratory systems were normal. Routine
radiographs and ultrasonography of the pelvis and hips revealed no
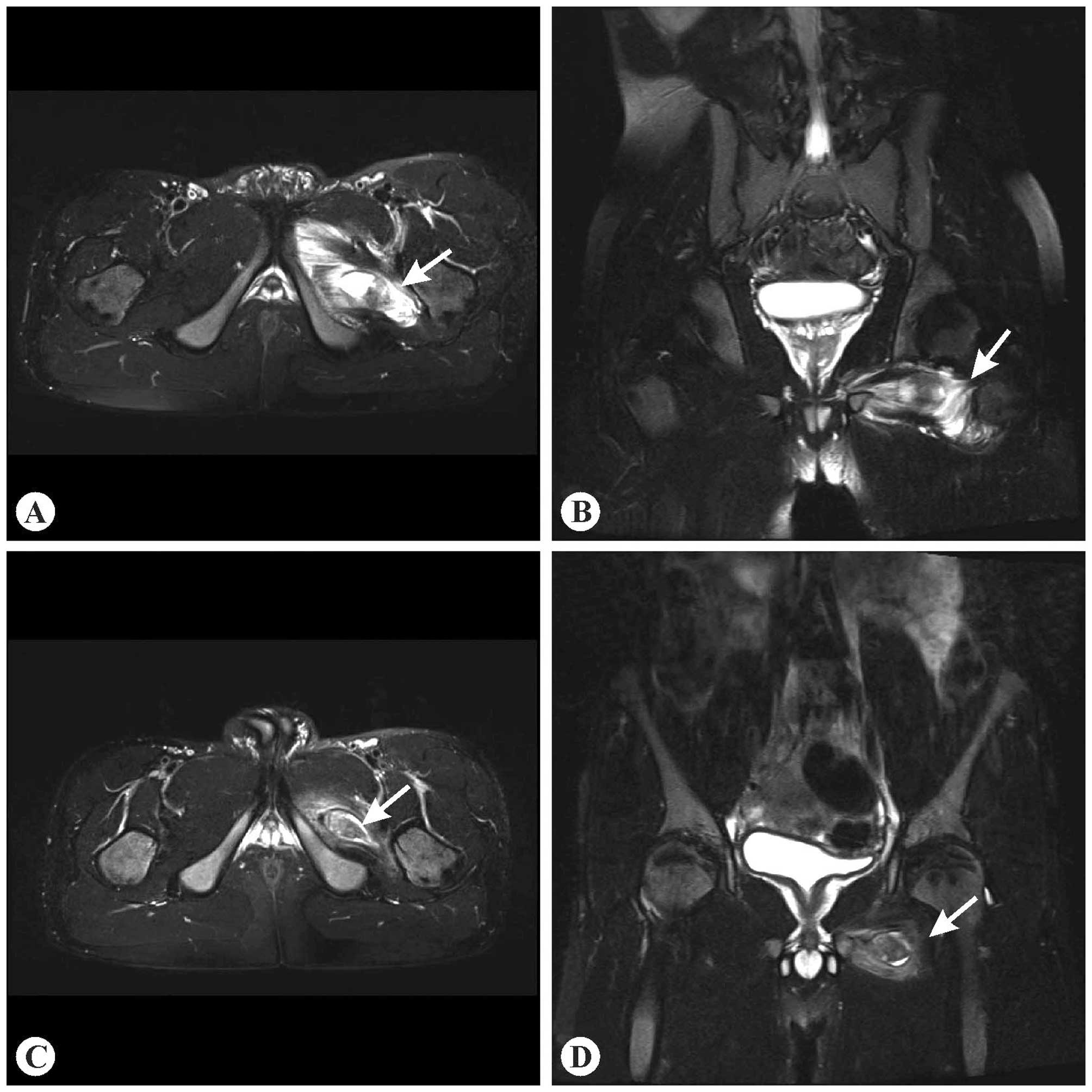
abnormalities. A pelvic MRI revealed extensive bleeding and edema
in the left obturator externus muscle (Fig. 1A and B). The clinical findings
subsided following initiation of treatment with recombinant
activated FVII (rFVIIa). The treatment included 90 mcg
kg−1 every 3 h for 3 days. The control MRI performed 3
weeks after the first hemorrhagic event revealed regression of the
intramuscular hematoma and edema (Fig. 1C
and D).
The patient was admitted to the emergency department
with right hip, groin and thigh pain 5 months after the first
event. The musculoskeletal findings were nearly identical to the
first presentation, when the patient was admitted to the hospital.
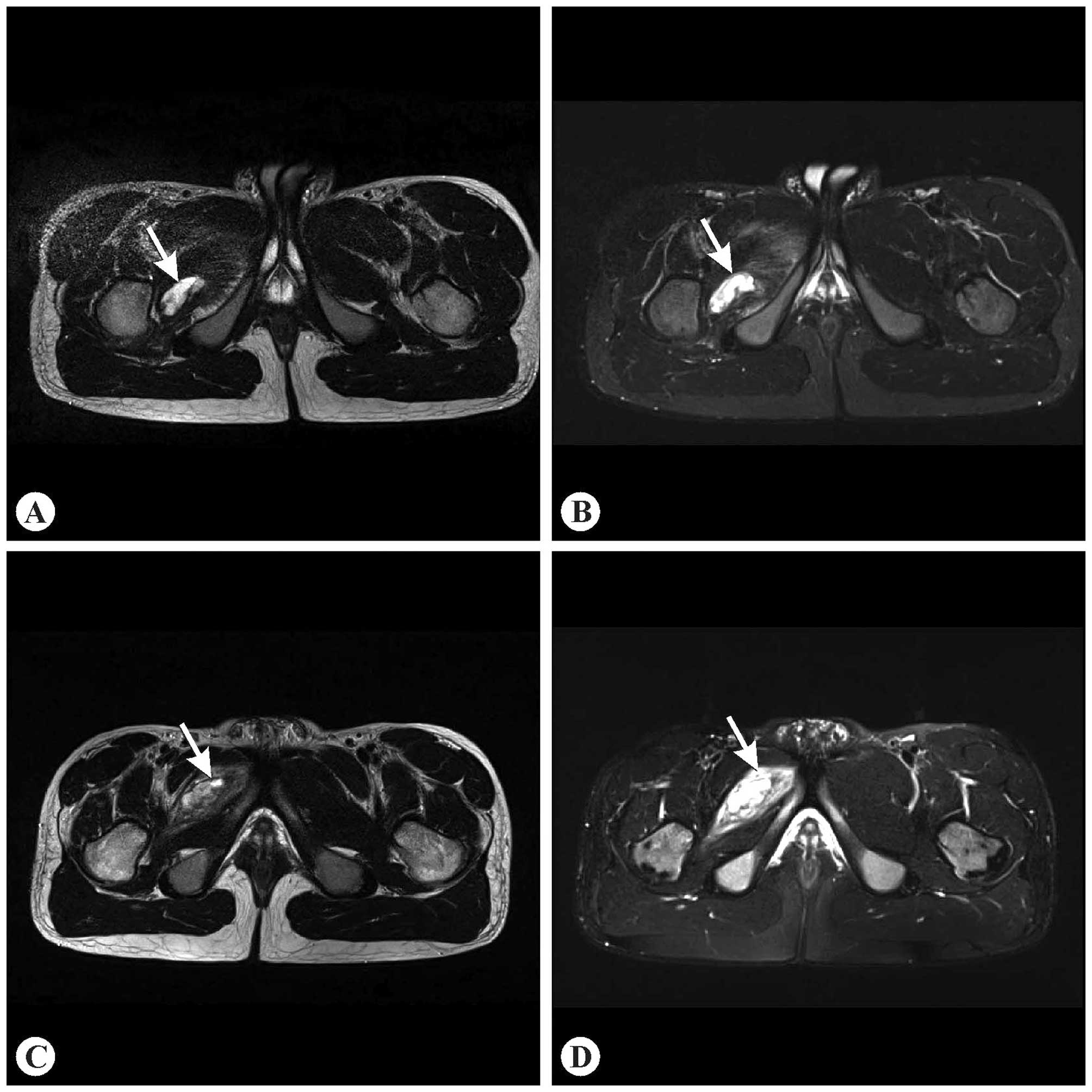
An MRI revealed a focal hematoma and mild peripheral edema in the
right obturator externus muscle (Fig.
2A–B). The symptoms were relieved following treatment with
rVIIa (90 mcg kg−1 every 3 h for 4 days).
The patient was again admitted to the emergency
department with right iliopelvic pain and identical musculoskeletal
findings 4 months after the second event. An MRI revealed a larger
hematoma and prominent edema in the right obturator externus muscle
(Fig. 2C and D). The clinical
findings were alleviated following treatment with rFVIIa (90 mcg
kg−1 every 3 h for 4 days).
Τhe patient provided written informed consent for
the publication of the details of this case.
Discussion
The majority of the hemorrhagic complications in
hemophiliac patients occur within the musculoskeletal system.
Following joint hemorrhages, intramuscular hemorrhages are the
second most prevalent bleeding pattern in haemophilia. Hemorrhaging
generally occurs following trauma, although it may also occur
spontaneously (7). The clinical
findings are based on the affected muscle, its dimensions and the
extent of the coagulation defect. Bleeding causes a soft swelling
in the muscle, quickly progressing into defensive spasm and leading
to flexion of the adjacent joint, with limitation of movement and
intense pain. A limited number of studies have been conducted on
the pathology of the mentioned muscle hematomas. It is considered
that muscle necrosis happens quickly due to ischemia of the fibres
as the developing hematoma damages the neurovascular bundles
(8).
A significant location of hematoma occurrence is the
iliopsoas muscle; this is a well-known complication of hemophilia
and is considered as a possibly life-threatening complication,
significantly associated with morbidity. Iliopsoas haematoma leads
to compression of the femoral nerve due to the developing lesion in
the muscle; there is generally no traumatic etiology and the first
occurrence is sudden, with intense lower abdominal or groin pain
(9).
The obturators are the pelvi-trochanteric muscles
originating from the posterior (obturator internus) and the
anterior (obtutrator externus) walls of the obturator foramen.
These two muscles attach to the greater trochanter of the femur and
they are involved in thigh external rotation and abduction, or
external rotation and adduction respectively. The differential
diagnosis of the obturator externus muscle hematoma should also
include primary pyomyositis or abscess. However, only two cases of
isolated obturator externus muscle abscess have been reported in
the literature to date (5–6). In intramuscular abscesses, fever and
elevation of the erythrocyte sedimentation rate or C-reactive
protein levels are likely to occur. An MRI with intravenous
gadolinium administration achieves a rapid diagnosis of muscle
inflammation and rim-enhancing abscess formation; it also enables
the detection of additional local pathologies (5).
Ultrasonography is generally of little value in the
diagnosis of obturator muscle hematomas, contrary to pelvic MRI, as
mentioned in the present case. The CT findings of the intramuscular
hematoma are non-spesific asymmetric muscular hypertrophy and
possible blood attenuation in the muscle (2). MRI demonstrates hemorrhagic signal
abnormality and edema in the affected muscle (10).
As a result, in addition to hip hemarthrosis,
iliopsoas hematomas and acute appendicitis, obturator muscle
hematoma must be considered as one of the diagnostic alternatives
for pelvic pain in patients with hemophilia.
References
|
1
|
Beyer R, Ingerslev J and Sørensen B:
Current practice in the management of muscle haematomas in patients
with severe haemophilia. Haemophilia. 16:926–931. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Aouba A, Breton S, Harroche A, Sy-Bah D,
Torchet MF, Frenzel L, Lasne D, Padovani JP, Odent T and Rothschild
C: Spontaneous obturator internus muscle haematoma: A new
unpublished cause of iliopelvic pain in haemophilia. Haemophilia.
19:157–160. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nikolopoulos DD, Apostolopoulos A,
Polyzois I, Liarokapis S and Michos I: Obturator internus
pyomyositis in a young adult: A case report and review of the
literature. Cases J. 2:85882009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
King RJ, Laugharne D, Kerslake RW and
Holdsworth BJ: Primary obturator pyomyositis: A diagnostic
challenge. J Bone Joint Surg Br. 85:895–898. 2003.PubMed/NCBI
|
|
5
|
Kumar A and Anderson D: Primary obturator
externus pyomyositis in a child presenting as hip pain: A case
report. Pediatr Emerg Care. 24:97–98. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fowler T and Strote J: Isolated obturator
externus muscle abscess presenting as hip pain. J Emerg Med.
30:137–139. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Duthie RB: Muscle bleeds and consequences.
The Management of Musculoskeletal Problems in the Hemophilias.
Duthie R, Rizza C, Giangrande P and Dodd C: (2nd). (Oxford). Oxford
University Press. 104–117. 1994.
|
|
8
|
Forbes CD: Clinical aspects of the genetic
disorders of coagulation. Disorders of Hemostasis. Ratnoff OD and
Forbes CD: (3rd). (Philadelphia). WB Saunders Company. 138–185.
1996.
|
|
9
|
Fernandez-Palazzi F, Hernandez SR, DeBosch
NB and De Saez AR: Hematomas within the iliopsoas muscles in
hemophilic patients: The Latin American experience. Clin Orthop
Relat Res. 19–24. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yuh WT, Schreiber AE, Montgomery WJ and
Ehara S: Magnetic resonance imaging of pyomyositis. Skeletal
Radiol. 17:190–193. 1988. View Article : Google Scholar : PubMed/NCBI
|