Introduction
Hemorrhagic cystitis (HC) is a rare disease that can
occur following radiotherapy and chemotherapy, including
cyclophosphamide regimens. HC is characterized by diffuse bleeding
from the bladder mucosa. By contrast with infectious cystitis, HC
is a potentially deadly complication (1). Treatment for this difficult disease
requires a wide range of invasiveness. For example, intravenous,
endoscopic and instillation therapy (aluminium hydroxide, magnesium
hydroxide aminocaproic acid, alum, silver nitrate solution)
(2–5),
hyperbaric oxygen therapy and a vascular approach (selective
embolization of the internal iliac arteries) may be possible
conservative therapies (6,7). Total cystectomy may be a final option
for patients with refractory HC (8).
However, high risk of perioperative complications and mortality
associated with surgery should be taken into consideration.
Aplastic anemia (AA) is a rare blood disorder and patients commonly
present with pancytopenia, increasing the risk of bleeding
complications, which can be fatal if left untreated (9). The present study reported severe HC,
which was unable to be managed with several conservative therapies,
however, improved by treatment for underlying AA that was diagnosed
belatedly.
Case report
A 70-year-old male was diagnosed to exhibit prostate
cancer with cT3aN0M0, initial prostate specific antigen 19.3 ng/ml,
and a Gleason score 5+4. The patient was treated by high dose rate
brachytherapy (19 Gy), followed by external beam radiotherapy
(EBRT; 46 Gy) for the whole pelvis, with combined androgen blockade
(leuprolide acetate and bicalutamide). Following 3 years of
radiotherapy, urinary retention and macroscopic hematuria occurred.
Ultrasonography revealed bladder tamponade and left hydronephrosis.
Abdominal computed tomography and magnetic resonance imaging
revealed no specific findings of the cause. As many minor bleedings
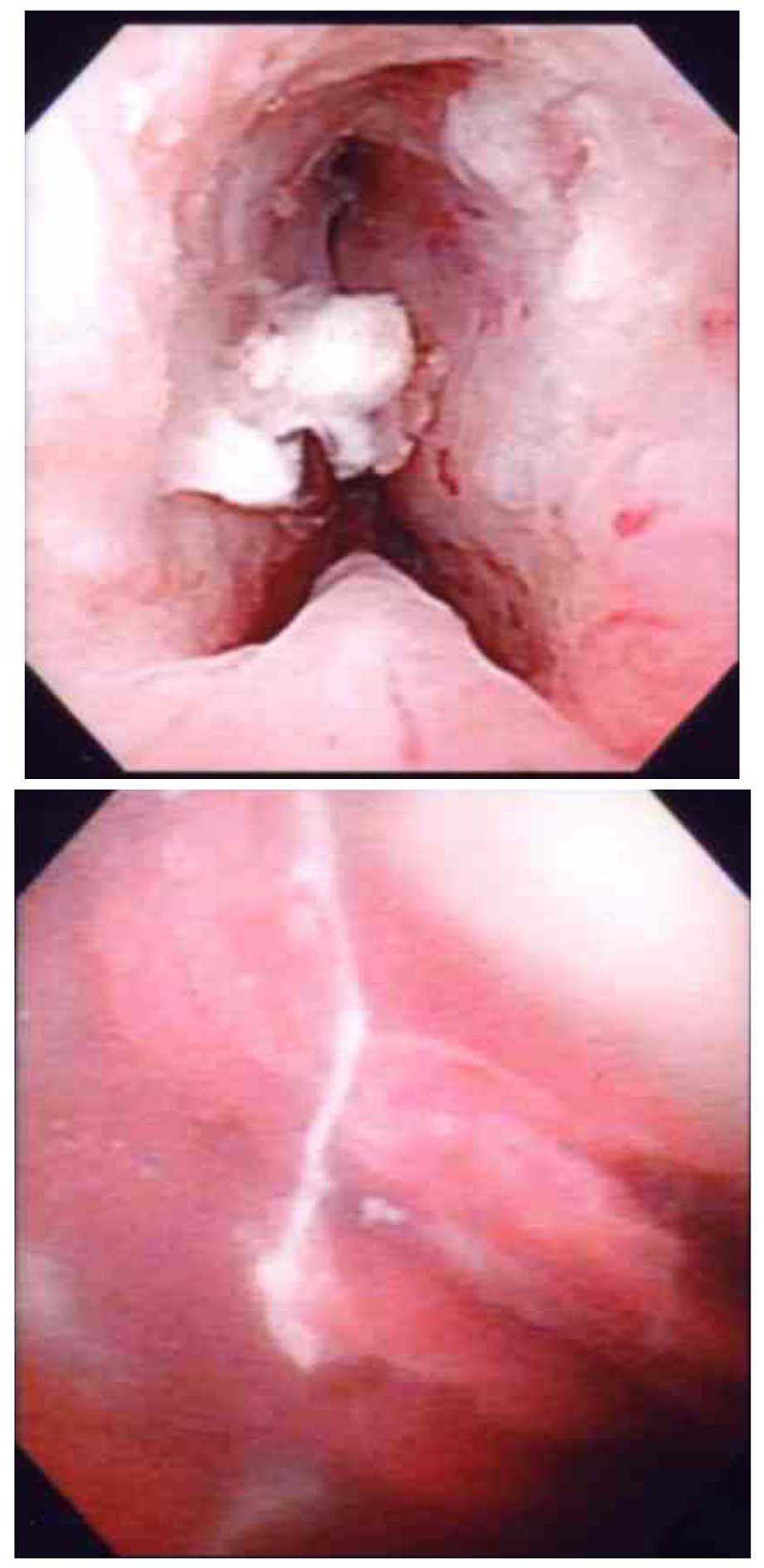
were observed in the bladder mucosa by cystoscopy, trans-urethral
coagulation was performed (Fig. 1).
The posterior wall and the urethral triangle in the bladder were
edematous, however, neither major bleeding or a cancerous lesion
were detected at this time. A long hematoma from the left ureteral
orifice was identified and retrograde pyelography revealed a
distorted lesion of the left lower ureter. However, urine cytology
from the left ureter revealed no malignancy. Biopsy of the bladder
mucosa and ureteroscopy to the left ureter revealed no evidence of
disease. Finally, radiation-induced HC was clinically diagnosed
with no clear evidence of other diseases. As the hematuria was very
severe and associated with frequent bladder tamponade and
deteriorating anemia, trans-urethral coagulations were performed
repeatedly during the next few months. Intravesical instillation of
the mixed compound of aluminium hydroxide and magnesium hydroxide
was administered, followed by hyperbaric oxygen therapy.
Nevertheless, no improvement of clinical symptom was observed.
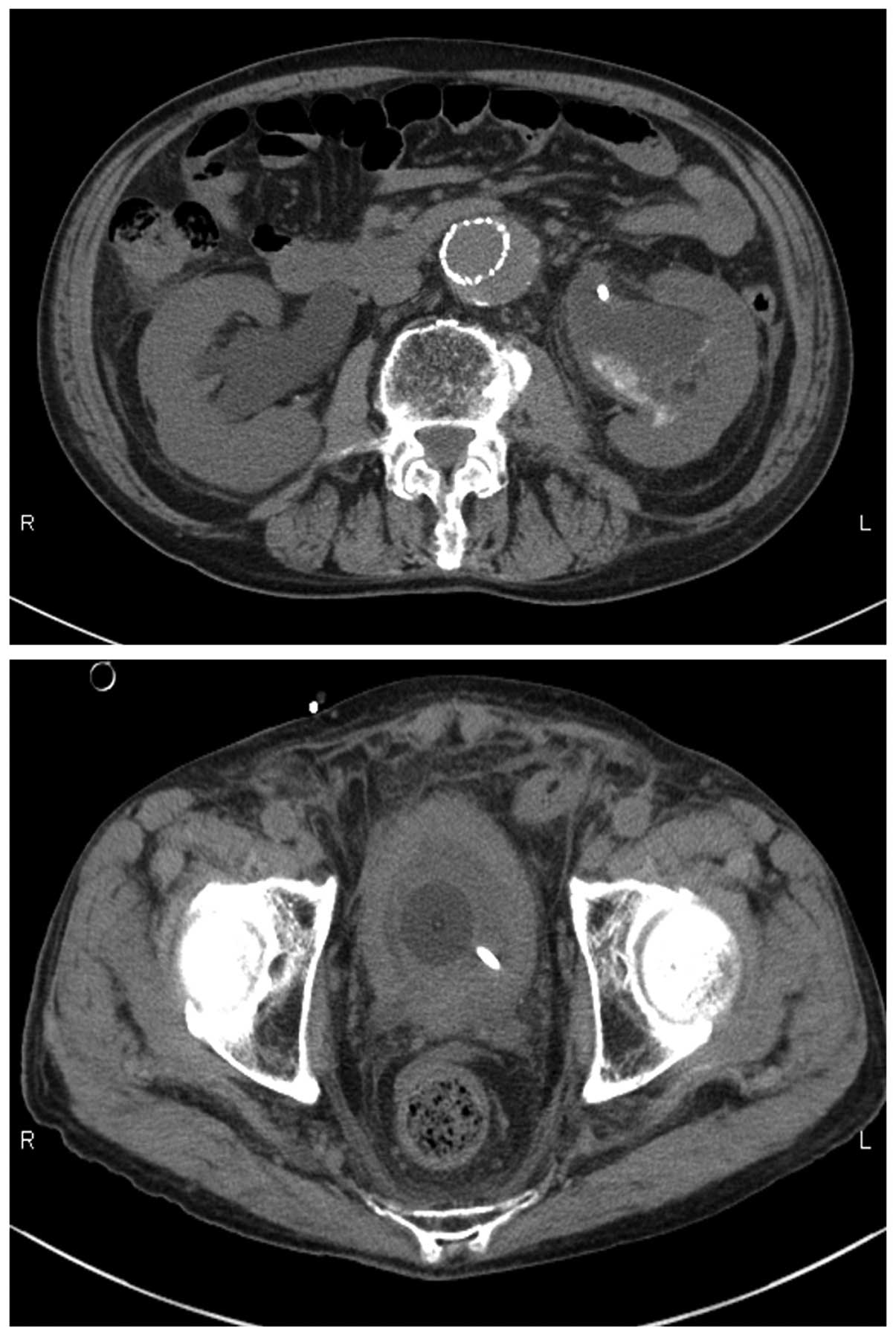
Subsequent bilateral hydronephroses and renal impairment with the
serum creatinine level of 8.72 mg/dl was developed and required the
induction of hemodialysis as well as bilateral percutaneous
nephrostomy (Fig. 2). A blood test
revealed pancytopenia and transfusions of red blood cells and
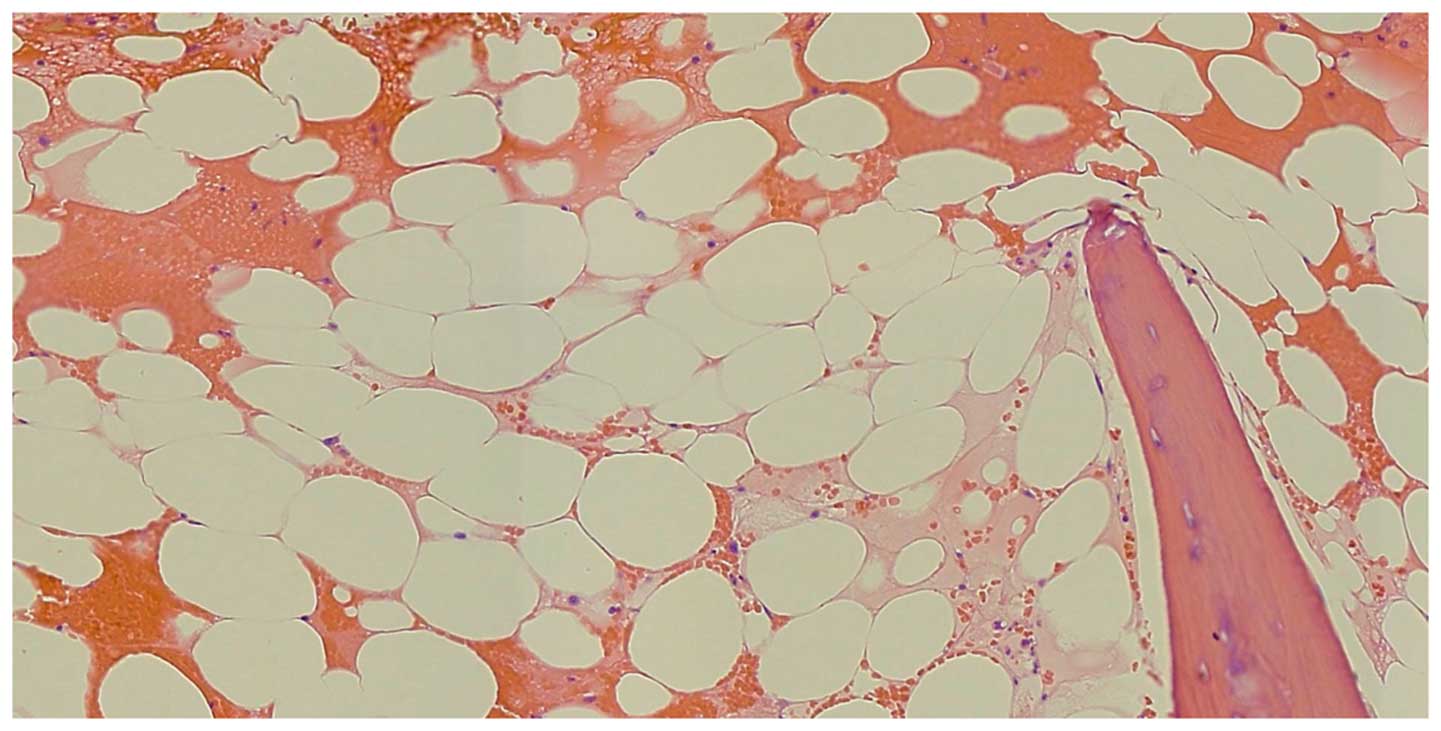
platelets were required every other day. When total cystectomy with
urinary diversion was considered for this difficult condition,
aplastic anemia (AA) was diagnosed by the bone marrow examination
(Fig. 3). Administration of
cyclosporine and anabolic steroid was initiated by hematologists,
and macroscopic hematuria was gradually improved. Subsequently,
renal impairment markedly improved to <1.0 mg/dl in the serum
creatinine level. The incidence of transfusions of red blood cells
and platelets was decreased to once a week thereafter.
Discussion
HC is defined as a diffuse inflammatory change of
the bladder characterized by sustained hematuria or lower urinary
tract symptom (10). HC may occur
following bone marrow transplantation, peripheral blood stem cell
transplantation, radiotherapy to the pelvic organ, chemotherapy
using cyclophosphamide, and specific viral infections (10). It is hypothesized that as a result of
mucosal edema and inflammation by radiotherapy, telangiectasia and
interstitial fibrosis occur, resulting in decreased bladder
capacity and compliance (11).
Finally, mucosal ischemia, ulceration and bleeding occur. HC can
occur generally between 6 months and 10 years after radiotherapy,
affecting ~6.5% of patients following pelvic radiation (11). Leapman et al (12) reported cystoscopy findings of 2,532
males treated with prostate brachytherapy with or without EBRT. Of
those, 13 individuals, (0.51%) were diagnosed with radiation
cystitis, and 8 received combined brachytherapy with EBRT, although
the total biological effective dose was similar among these groups
(208.6, compared with 200 Gy; P=0.092). Lawton et al
(13) reported that the risk of HC
increases with higher doses of radiation (>70 Gy) and a larger
treatment area (13). On the other
hand, Fuentes-Raspall et al (14) analyzed 257 patients treated with EBRT
for prostate cancer. They reported that late rectal toxicity was
associated with the volume irradiated, however, could not correlate
with the bladder volume (14).
Further studies are required to investigate whether irradiated
volume is a risk factor for HC. Treatment of HC can range from
simple bladder irrigation to invasive surgery. For refractory cases
to conservative therapy, urinary diversion can be considered.
However, cystectomy for radiation cystitis is often more difficult.
It was reported that the 90-day mortality rate in patients with HC
undergoing a cystectomy was 16% (15). Cystectomy with urinary diversion is
associated with a high rate of perioperative complications and
radiation-induced fistula (14). The
present study considered this challenging method, however, AA was
accidentally diagnosed in the background of HC. On multivariate
analysis, increased risk factors of HC were significantly
associated with previous pelvic radiation (10). Although it is unclear whether AA is a
risk factor for HC or not, treatment for AA improved symptoms
caused by HC, perhaps as a result of hematopoietic improvement.
Close examination in the background of HC is required in severe and
treatment-resistant HC.
References
|
1
|
Haldar S, Dru C and Bhowmick NA:
Mechanisms of hemorrhagic cystitis. Am J Clin Exp Urol. 2:199–208.
2014.PubMed/NCBI
|
|
2
|
Kawagoe K and Kawana T: Intravesical
instillation of maalox for the treatment of hemorrhagic cystitis.
Asia Oceania J Obstet Gynaecol. 15:107–108. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kawamura N, Kakuta Y, Fukuhara S, Imazu T,
Hara T and Yamaguchi S: Successful treatment of hemorrhagic
cystitis after radiation therapy with intravesical instillation of
aluminium hydroxide gel and magnesium hydroxide: Report of a case.
Hinyokika Kiyo. 54:239–241. 2008.PubMed/NCBI
|
|
4
|
Kanwar VS, Jenkins JJ III, Mandrell BN and
Furman WL: Aluminum toxicity following intravesical alum irrigation
for hemorrhagic cystitis. Med Pediatr Oncol. 27:64–67. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jerkins GR, Noe HN and Hill DE: An unusual
complication of silver nitrate treatment of hemorrhagic cystitis:
Case report. J Urol. 136:456–458. 1986.PubMed/NCBI
|
|
6
|
de Ribeiro Oliveira TM, Carmelo Romão AJ,
Gamito Guerreiro FM and Matos Lopes TM: Hyperbaric oxygen therapy
for refractory radiation-induced hemorrhagic cystitis. Int J Urol.
22:962–966. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Han Y, Wu D, Sun A, Xie Y, Xu J, Zhou J,
Zhu X, Wang Z and Ruan C: Selective embolization of the internal
iliac arteries for the treatment of severe hemorrhagic cystitis
following hematopoietic SCT. Bone Marrow Transplant. 41:881–886.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Linder BJ, Tarrell RF and Boorjian SA:
Cystectomy for refractory hemorrhagic cystitis: Contemporary
etiology, presentation and outcomes. J Urol. 192:1687–1692. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Willis L, Rexwinkle A, Bryan J and Kadia
TM: Recent developments in drug therapy for aplastic anemia. Ann
Pharmacother. 48:1469–1478. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Riachy E, Krauel L, Rich BS, McEvoy MP,
Honeyman JN, Boulad F, Wolden SL, Herr HW and La Quaglia MP: Risk
factors and predictors of severity score and complications of
pediatric hemorrhagic cystitis. J Urol. 191:186–192. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Alesawi AM, El-Hakim A, Zorn KC and Saad
F: Radiation-induced hemorrhagic cystitis. Curr Opin Support
Palliat Care. 8:235–240. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Leapman MS, Stock RG, Stone NN and Hall
SJ: Findings at cystoscopy performed for cause after prostate
brachytherapy. Urology. 83:1350–1355. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lawton CA, Won M, Pilepich MV, Asbell SO,
Shipley WU, Hanks GE, Cox JD, Perez CA, Sause WT, Doggett SR, et
al: Long-term treatment sequelae following external beam
irradiation for adenocarcinoma of the prostate: Analysis of RTOG
studies 7506 and 7706. Int J Radiat Oncol Biol Phys. 21:935–939.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fuentes-Raspall R, Inoriza JM,
Rosello-Serrano A, Auñón-Sanz C, Garcia-Martin P and Oliu-Isern G:
Late rectal and bladder toxicity following radiation therapy for
prostate cancer: Predictive factors and treatment results. Rep
Pract Oncol Radiother. 18:298–303. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Linder BJ, Boorjian SA, Hudolin T,
Cheville JC, Thapa P, Tarrell RF and Frank I: Late recurrence after
radical cystectomy: Patterns, risk factors and outcomes. J Urol.
191:1256–1261. 2014. View Article : Google Scholar : PubMed/NCBI
|