Introduction
Strategies for the treatment of lateral pelvic lymph
node (LPLN) metastasis in patients with lower rectal cancer has
been controversial. In Western countries (1,2), LPLN
dissection (LPLD) is rarely used since LPLN metastasis is viewed as
a systemic disease. By contrast, in Japan, LPLN is categorized
according to the regional lymph node and LPLN metastasis is treated
as a localized lesion (3). Notably, a
previous Japanese nationwide multi-institutional study (4) demonstrated that the survival rate of
patients with internal iliac lymph node metastasis was comparable
to that of cases with a tumor, node, metastasis (TNM)
classification of N2a, and that the survival rate of patients with
LPLN metastasis, which is more distant than the internal iliac
lymph node, was comparable to that in cases with a classification
of N2b. These previous findings suggested that LPLN metastasis can
be recognized as local disease. The 5 year overall and
cancer-specific survival rates of patients with LPLN metastasis
were better compared with those of stage IV patients following
curative resection (4). Total
mesorectal excision (TME) with LPLD is the established method for
advanced lower rectal cancer, and LPLD in Japan was effective in
reducing the intrapelvic recurrence by 50% and improving the 5 year
survival rate by 8–9% (5).
The diagnostic utility of diffusion-weighted imaging
(DWI) in magnetic resonance imaging (MRI) for patients with
colorectal cancer has previously been reported (6,7). DWI
detects the random movement of water molecules in tissue. This
diffusion is inhibited in densely proliferating cells, including
fibrosis, edema and tumors, and this is visualized as an abnormally
high intensity signal (8).
Furthermore, diffusion capacity decreases in malignant tumors
compared with that in benign tumors as a result of the higher cell
density, and therefore, DWI can differentiate between malignant and
benign tumor types (8,9). The signal intensities of primary lesions
and lymph node metastases on DWI are also higher compared with that
of the surrounding area, and this high contrast facilitates the
detection of lesions.
In a multicenter cooperative study of 1,427 patients
with lower rectal cancer in Japan, the incidences of LPLN
metastasis was 16.7% in cases treated with LPLD and 9.8% in all
patients including without LPLD, respectively (10). By depth of tumor invasion, the
incidences were 0.9, 5.4, 13.5 and 28.8% in T1, T2, T3 and T4
cases, respectively (10).
A patient with T1 lower rectal cancer with LPLN
metastasis, which is relatively uncommon, in whom diagnosis by DWI
MRI was useful was presented. The present study reported the case
and discussed the current status of diagnosis of LPLN metastasis of
lower rectal cancer and the indication for LPLD. The patient
provided written informed consent.
Case report
The present patient was a 35-year-old female who
visited a physician for close examination of fecal occult blood
detected at a medical check-up. The patient was diagnosed with
rectal cancer following colonoscopy, and was referred and admitted
to Tokyo Women's Medical University (Tokyo, Japan). No particular
familial or past medical history was known, and no abnormality was
detected in blood tests and tumor markers were within the normal
ranges (carcinoembryonic antigen, 0.8 ng/ml; cancer antigen 19-9, 6
U/ml).
Colonoscopy revealed a superficial elevated-type
tumor with a central depression in the lower rectum. This tumor was
diagnosed as T1 deep invasive cancer due to a
Vnon-structural pit pattern being observed at high
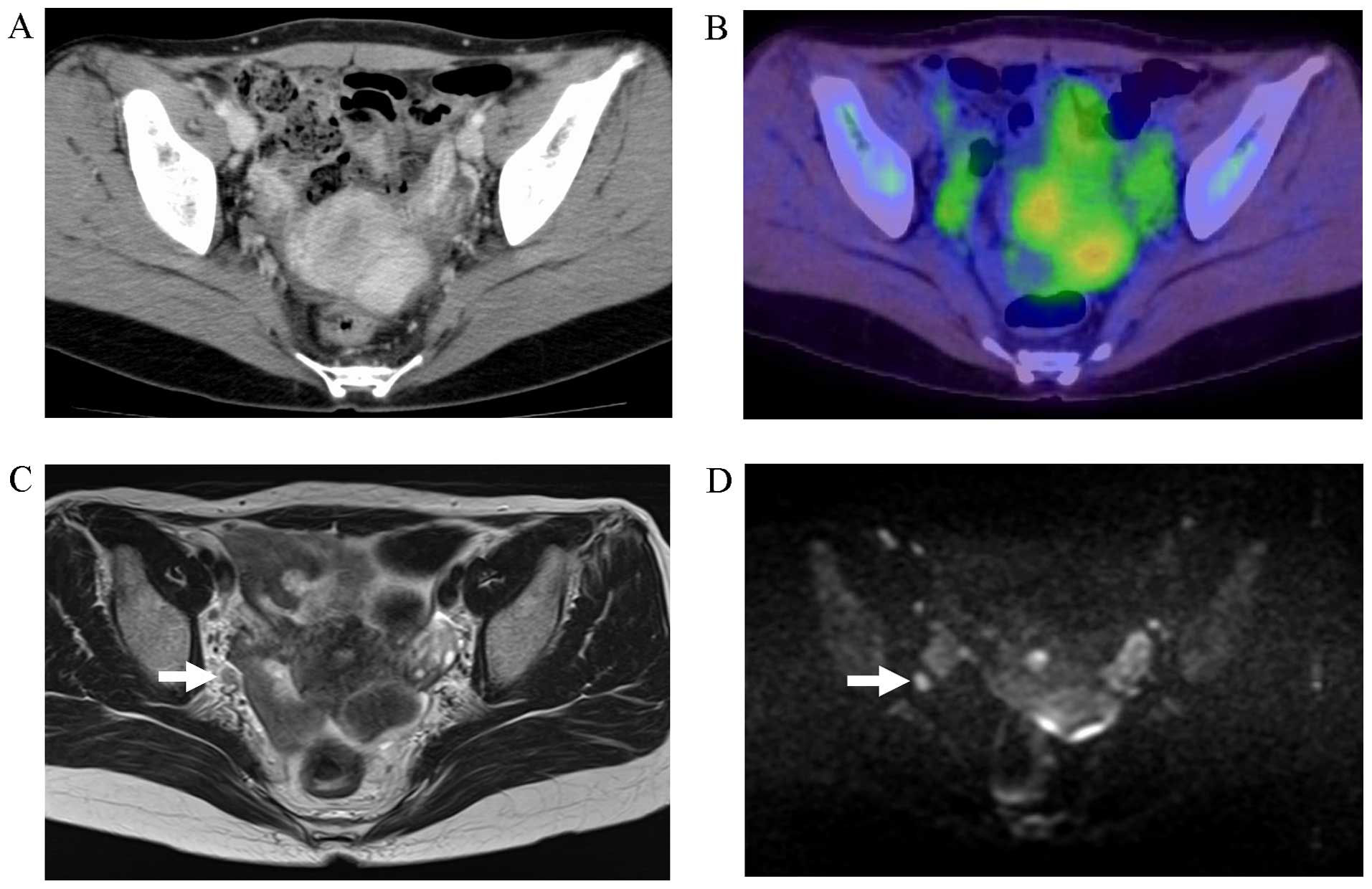
magnification. No features indicating swollen lymph nodes or
distant metastasis were present on computed tomography (CT) or
[18F]-fluorodeoxyglucose positron emission tomography
(18F-FDG PET) with CT. However, a swollen lymph node
with a short axis of 4 mm was visualized in the right lateral
region on MRI, and this lymph node exhibited a high intensity on
DWI, suggesting lymph node metastasis (Fig. 1).
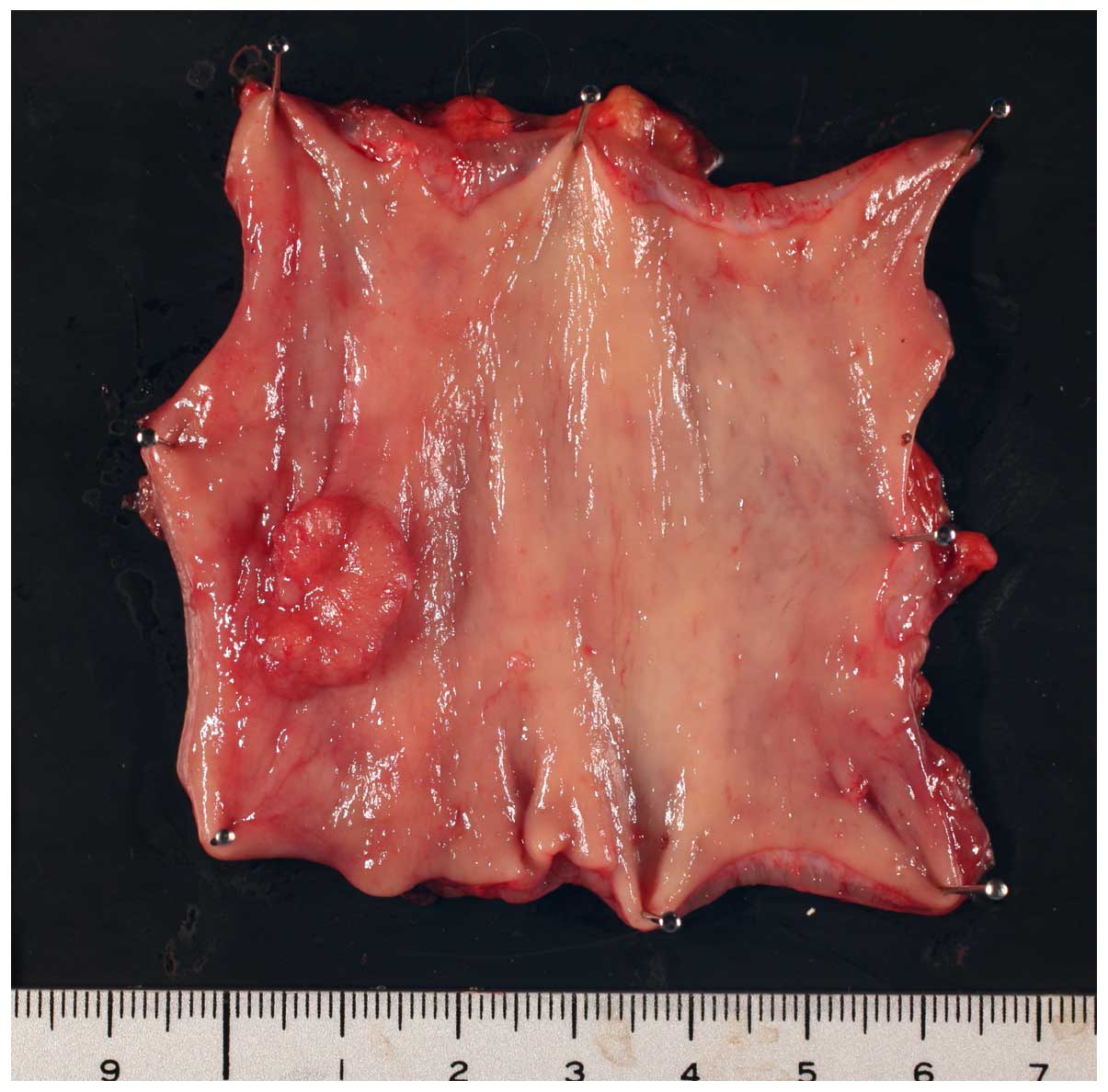
In surgery, low anterior resection and dissection of
the regional lymph node and right LPLN were performed. The tumor
measured 16×12 mm (Fig. 2), the
histopathological grade was 1, the classification was pT1 and the
vertical depth of invasion from the lamina muscularis mucosae was
3,000 µm (L1, V0). These findings indicated right LPLN metastasis,
as suspected based on the high intensity signal on DWI. No
postoperative complications occurred and the patient was discharged
10 days after surgery. Post-operative adjuvant chemotherapy with
Tegafur-uracil + leucovorin was performed. The patient remains
alive and has been recurrence-free 4 years after surgery.
Discussion
Diagnosis of lymph node metastasis from rectal
cancer is usually made using imaging studies, including endoscopic
ultrasound, CT and MRI, which have accuracies of 61–80, 56–79 and
57–85%, respectively (11). The
European Society for Medical Oncology guidelines specify MRI as the
first-line imaging test as it allows wide evaluation inside and
outside the mesorectum (12). MRI has
superior contrast resolution in soft tissue and is an excellent
method with multiplanar imaging capacity that is generally used for
pre-treatment N staging of rectal cancer (9). The sensitivity and specificity of MRI
for diagnosis of lymph node metastasis were revealed to be 77 and
71%, respectively, in a recent meta-analysis (13). However, this meta-analysis also
revealed a low diagnostic odds ratio with MRI for rectal cancer
lymph node metastasis, indicating that MRI cannot be used to
evaluate lymph nodes accurately and is insufficient for complete
diagnosis (13).
One of the problems associated with MRI diagnosis of
lymph node metastasis is a lack of valid diagnostic criteria. The
widely accepted criterion has been the size of lymph nodes on MRI
images (14). This is based on the
observation that metastasis-positive lymph nodes were larger
compared with metastasis-negative nodes. The size criteria,
however, has limited value in its performance since small lymph
nodes are also often positive and the maximum diameters of positive
and negative nodes overlapped to a certain extent on a histogram
(14). Morphological imaging
criteria, including signal heterogeneity and an irregular border,
have also been proposed (14),
however, they are not applicable to small lymph nodes sized ≤4 mm
(15). Therefore, MRI diagnosis of
lymph node metastasis of rectal cancer remains difficult using
current techniques.
The utility of DWI for diagnosis of malignant tumors
has recently been suggested. When lymph nodes with high signal
intensity are detected on DWI, which does not depend on the size,
they are considered to be metastasis-positive. For diagnosis of
lymph node metastasis of colorectal cancer, Mizukami et al
(16) found that the accuracy of DWI
of 86.8% compared favorably with that of 76.0% for CT. Similarly,
Ono et al (6) found an
accuracy of DWI of 78.3%, which was more favorable compared with
that of 69.6% for 18F-FDG-PET. DWI also has a higher
sensitivity and negative predictive value compared with CT and
18F-FDG-PET, indicating that fewer cases of lymph node
metastasis are diagnosed as false negatives by DWI-MRI. When lymph
nodes with high signal intensity are not detected on DWI, these
cases are more likely to be negative for lymph node metastasis.
However, differentiation of metastasis-positive and
metastasis-negative lymph nodes on DWI is limited since
non-metastatic lymph nodes can give high intensity signals in
certain cases (9,17). In advanced colorectal cancer,
inflammation-induced (reactive) swelling of the lymph nodes is
common and may lead to false-positive results (18). By contrast, in early cancer, reactive
swelling of lymph nodes does not occur frequently. Choi et
al (18) suggested that a high
intensity DWI signal for a lymph node in the case of early cancer
is more likely to be due to metastasis compared with reactive
swelling.
According to the current Japanese guidelines
(10), LPLD is recommended for a
patient whose tumor has its lower border distal to the peritoneal
reflection and the clinical grade of ≥T3, irrespective of
preoperative diagnosis of LPLN metastasis. The recommendation is
based on the study in which risk factors for LPLN metastasis were
identified to be female gender, tumor location in the lower rectum,
histological type of non-well-differentiated adenocarcinoma,
maximum tumor diameter ≥4 cm and depth of tumor invasion T3 or T4,
according to the analysis of 1,977 cases accumulated from high
volume centers in Japan (5). Analysis
of the pre-operative risk factors, the odds ratios for a location
in the lower rectum and the depth of tumor invasion T3 and T4 were
high, based on which the indication in the current guidelines was
established (5). The cohort in the
multi-center study, however, was relatively old (1991–1998) and
imaging diagnosis of LPLN metastasis was not taken into
consideration. The present case was judged to be cT1, which is not
included in the indication for LPLD in the current guidelines.
Additionally, if the case had been evaluated by CT and
18F-FDG-PET/CT only, without MRI, the pre-operative LPLN
status would have been judged to be metastasis-negative, and it is
unlikely that LPLD would have been performed.
Fujita et al (19) found that CT diagnosis was the most
powerful predictor of LPLN metastasis compared with any other
independent factors, including pathological status of regional
lymph nodes, tumor location and tumor differentiation, suggesting
that evaluation of LPLN metastasis by imaging studies is important
in determining the treatment strategy for rectal cancer.
In T1 cases, reactive swelling of lymph nodes is
less likely to occur and the incidence of LPLN metastasis is low
(0.9%) (10). Therefore, as with the
present case, an LPLN that provides a high signal intensity on DWI
in a case of T1 lower rectal cancer is likely to be a
metastasis-positive lymph node. DWI appears to be useful for
diagnosing or ruling out LPLN metastasis of T1 lower rectal cancer.
A prospective study that examines the role of DWI-MRI on LPLN in
planning the treatment strategy for rectal cancer is warranted.
Acknowledgements
The authors would like to thank Palabra (www.palabra.co.jp) for the English language
review.
References
|
1
|
Georgiou P, Tan E, Gouvas N, Antoniou A,
Brown G, Nicholls RJ and Tekkis P: Extended lymphadenectomy versus
conventional surgery for rectal cancer: A meta-analysis. Lancet
Oncol. 10:1053–1062. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Quadros CA, Falcão MF, Carvalho ME, Ladeia
PA and Lopes A: Metastases to retroperitoneal or lateral pelvic
lymph nodes indicated unfavorable survival and high pelvic
recurrence rates in a cohort of 102 patients with low rectal
adenocarcinoma. J Surg Oncol. 106:653–658. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Japanese Society for Cancer of the Colon
and Rectum: Japanese classification of colorectal carcinoma (2nd).
Tokyo: Kanehara: 2009.
|
|
4
|
Akiyoshi T, Watanabe T, Miyata S, Kotake
K, Muto T and Sugihara K: Japanese society for cancer of the colon
and rectum: Results of a Japanese nationwide multi-institutional
study on lateral pelvic lymph node metastasis in low rectal cancer:
Is it regional or distant disease? Ann Surg. 255:1129–1134. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sugihara K, Kobayashi H, Kato T, Mori T,
Mochizuki H, Kameoka S, Shirouzu K and Muto T: Indication and
benefit of pelvic sidewall dissection for rectal cancer. Dis Colon
Rectum. 49:1663–1672. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ono K, Ochiai R, Yoshida T, Kitagawa M,
Omagari J, Kobayashi H and Yamashita Y: Comparison of
diffusion-weighted MRI and 2-[fluorine-18]-fluoro-2-deoxy-D-glucose
positron emission tomography (FDG-PET) for detecting primary
colorectal cancer and regional lymph node metastases. J Magn Reson
Imaging. 29:336–340. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhao Q, Liu L, Wang Q, Liang Z and Shi G:
Preoperative diagnosis and staging of rectal cancer using
diffusion-weighted and water imaging combined with dynamic
contrast-enhanced scanning. Oncol Lett. 8:2734–2740.
2014.PubMed/NCBI
|
|
8
|
Kwee TC, Takahara T, Ochiai R, Koh DM,
Ohno Y, Nakanishi K, Niwa T, Chenevert TL, Luijten PR and Alavi A:
Complementary roles of whole-body diffusion-weighted MRI and
18F-FDG PET: The state of the art and potential applications. J
Nucl Med. 51:1549–1558. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Torkzad MR, Påhlman L and Glimelius B:
Magnetic resonance imaging (MRI) in rectal cancer: A comprehensive
review. Insights Imaging. 1:245–267. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Watanabe T, Itabashi M, Shimada Y, Tanaka
S, Ito Y, Ajioka Y, Hamaguchi T, Hyodo I, Igarashi M, Ishida H, et
al: Japanese society for cancer of the colon and rectum (JSCCR)
guidelines 2014 for treatment of colorectal cancer. Int J Clin
Oncol. 20:207–239. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Klessen C, Rogalla P and Taupitz M: Local
staging of rectal cancer: The current role of MRI. Eur Radiol.
17:379–389. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schmoll HJ, Van Cutsem E, Stein A,
Valentini V, Glimelius B, Haustermans K, Nordlinger B, van de Velde
CJ, Balmana J, Regula J, et al: ESMO consensus guidelines for
management of patients with colon and rectal cancer. A personalized
approach to clinical decision making. Ann Oncol. 23:2479–2516.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Al-Sukhni E, Milot L, Fruitman M, Beyene
J, Victor JC, Schmocker S, Brown G, McLeod R and Kennedy E:
Diagnostic accuracy of MRI for assessment of T category, lymph node
metastases and circumferential resection margin involvement in
patients with rectal cancer: A systematic review and meta-analysis.
Ann Surg Oncol. 19:2212–2223. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Brown G, Richards CJ, Bourne MW, Newcombe
RG, Radcliffe AG, Dallimore NS and Williams GT: Morphologic
predictors of lymph node status in rectal cancer with use of
high-spatial-resolution MR imaging with histopathologic comparison.
Radiology. 227:371–377. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Akasu T, Iinuma G, Takawa M, Yamamoto S,
Muramatsu Y and Moriyama N: Accuracy of high-resolution magnetic
resonance imaging in preoperative staging of rectal cancer. Ann
Surg Oncol. 16:2787–2794. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mizukami Y, Ueda S, Mizumoto A, Sasada T,
Okumura R, Kohno S and Takabayashi A: Diffusion-weighted magnetic
resonance imaging for detecting lymph node metastasis of rectal
cancer. World J Surg. 35:895–899. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Heijnen LA, Lambregts DM, Mondal D,
Martens MH, Riedl RG, Beets GL and Beets-Tan RG: Diffusion-weighted
MR imaging in primary rectal cancer staging demonstrates but does
not characterise lymph nodes. Eur Radiol. 23:3354–3360. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Choi J, Oh SN, Yeo DM, Kang WK, Jung CK,
Kim SW and Park MY: Computed tomography and magnetic resonance
imaging evaluation of lymph node metastasis in early colorectal
cancer. World J Gastroenterol. 21:556–562. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fujita S, Yamamoto S, Akasu T and Moriya
Y: Risk factors of lateral pelvic lymph node metastasis in advanced
rectal cancer. Int J Colorectal Dis. 24:1085–1090. 2009. View Article : Google Scholar : PubMed/NCBI
|