Introduction
Multiple primary cancers are defined as ≥2 separate
original cancers, simultaneously or successively occurring in the
same or different organs. Double primary cancer is the most common
type of multiple primary cancer and it is classified as synchronous
carcinoma (SC) and metachronous carcinoma (MC). SC is used to
describe the second primary tumor when it is diagnosed
simultaneously or within 6 months of the diagnosis of the first
primary tumor. MC is is used to describe the second cancer when it
is diagnosed >6 months after the first primary cancer (1). The first double primary cancer was
reported in 1889 by Billroth (2),
whose standard of the diagnosis was that each tumor should have a
different localization and independent histological appearance. In
1932, Warren and Gates established new criteria, which are still
applied today: i) both cancers must be definitively malignant
according to the histopathological examination; ii) the cancers
must be histologically different; and iii) it must be established
that the second cancer is not a metastatic lesion of the first
(3). the incidence of multiple
primary cancers appears to have increased significantly.
Approximately 10% of cancer patients develop another primary cancer
within 10 years of the first surgery (4). However, double primary cancer of the
lung and nasal vestibule is uncommon. We herein describe an
extremely rare case of synchronous double primary cancer involving
the left nasal vestibule and the left lung, with a review of the
literature.
Case report
A 55-year-old man presented to the Qianfoshan
Hospital on April 8, 2015, where he was diagnosed with a neoplasm
of the left lung. The patient had noticed bloodstained sputum 5
years prior, which later disappeared. However, the symptom recurred
2 weeks prior to admission, with accompanying intermittent pain in
the left hemithorax. The patient also reported loss of appetite and
weight loss of 3 kg over the last 2 months. The patient had been a
chronic smoker (40 cigarettes/day) and consumed alcohol (500
gr/day) for 20 years. On physical examination, there was no
peripheral lymph node enlargement. The laboratory tests revealed a
squamous cell carcinoma (SCC) antigen level of 2.1 ng/ml (normal
value: <1.5 ng/ml); the other blood tests were all within the
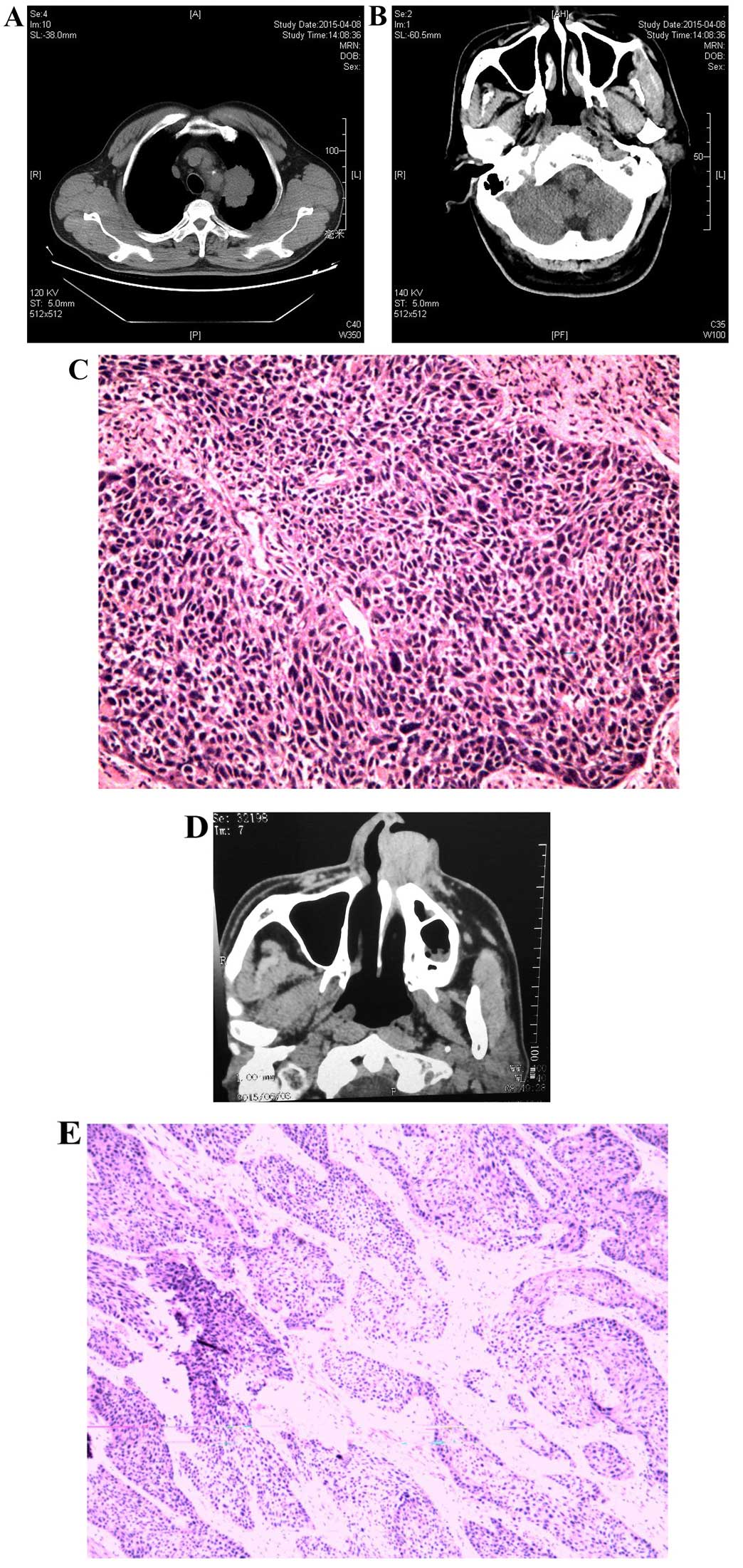
normal range. Contrast-enhanced computed tomography (CECT)
examination of the thorax revealed a mass sized ~5.3x3.7
cm in the upper lobe of the left lung (Fig. 1A). Other radiological examinations,
including whole-body emission CT, did not reveal any evidence of
distant metastasis, and a CT scan of the brain was unremarkable
(Fig. 1B). The patient was treated
with left upper lobectomy and mediastinal lymph node sampling.
Following histopathological examination, the lesion was diagnosed
as poorly differentiated SCC (pT3N0M0, IIb) (Fig. 1C). No lymph nodes were infiltrated.
Three weeks later, the patient received one cycle of adjuvant
chemotherapy with regular doses of nedaplatin (120 mg/day) and
gemcitabine (1,600 mg/day).
On a regular visit after chemotherapy week 1, the
patient presented with a small amount of purulent and bloody
discharge from the left nostril, which was first diagnosed as an
upper jaw cyst, and was treated with cefathiamidine antibiotics for
two days (2g, twice per day). Three weeks later, the patient was
re-admitted with bloody discharge from the left nostril, a mass in
the nose and nasal congestion. The CT examination revealed a mass
over the left nasal vestibule (Fig.
1D). Tru-Cut biopsies from the nasal area were performed and
histopathological examination revealed a moderately differentiated
SCC (pT2N0M0) (Fig. 1E). According to
the history, the patient was finally diagnosed with double primary
cancer of the lung and nasal vestibule. Following systemic
evaluation, external-beam radiation treatment was recommended and
the nasal tumor was significantly reduced after one cycle of
radiotherapy.
Discussion
Lung cancer is one of the most commonly diagnosed
types of cancer affected by population aging and changes in
lifestyle, such as smoking and physical inactivity (5). Non-small-cell lung cancer is the leading
cause of cancer-related mortality worldwide (5). The number of new cases of lung cancer
diagnosed annually worldwide is ~1.5 million (6). Surgery, radiotherapy, chemotherapy and
immunotherapy are the four most widely employed cancer treatments
(7). However, Han et al
reported that the 5-year survival rate remains very poor (8). Nasal vestibular carcinomas are uncommon
and are typically sccs. They display a natural history similar to
that of skin cancers and their prognosis is more favorable compared
with other cancers of the nasal cavity (9). Nasal vestibular carcinomas are often
located in the nasal floor, the nasal dome, the medial crus of the
lower lateral cartilage and the inner lining of the alar wing
(lateral crus), and account for <3.8% of all nasal mucosal
tumors and 1% of all malignant tumors of the head and neck
(10–12). Human papillomavirus infection and
smoking are considered to be risk factors (12). However, their prognosis remains better
compared with that of other sinonasal malignant tumors, such as
maxillary sinus and frontal sinus malignant tumor (13,14). The
5-year recurrence-free survival rates range widely between 20 and
92% (15–17).
To the best of our knowledge, cases of double
primary cancer of the nasal vestibule and lung are extremely rare.
Thus, a number of patients may be misdiagnosed or remain
undiagnosed in the first visit, resulting in a delay in treatment.
The patient in the present study was originally misdiagnosed with
an upper jaw cyst. Taking into consideration the clinical symptoms,
signs and the correlation of the examinations with the opinions of
experts, including a thoracic surgeon, otolaryngologist and
pathologist, the patient was finally diagnosed with double primary
cancer of the lung and nasal vestibule: i) we were able to
determine that the cancer of lung occurred earlier compared with
that of the nasal vestibule and the possibility of pulmonary
metastatic tumor was ruled out, as the patient had first presented
with bloodstained sputum 5 years prior and the CECT examination of
the thorax revealed a large mass, whereas the CT scan of the brain
was unremarkable. ii) head and neck metastasis from lung cancer is
an unusual event, particularly to the nasal vestibule. The larynx
is a terminally located organ in regard to vascular and lymphatic
circulation (18). Primary pulmonary
cancer metastasis to the larynx is very rare through the vascular
or lymphatic route, and metastasis to the nasal vestibule is even
rarer. In addition, on preoperative clinical examination there was
no cervical lymph node enlargement and the test results revealed no
evidence of distant metastasis. iii) Although the histopathological
diagnosis of both tumors was SCC, the degree of pathological
differentiation (the level of malignancy) was different. Thus,
metastatic carcinoma was deemed unlikely.
However, identification of the primary or metastatic
nature of the nasal vestibular SCC is difficult. As there is no
definitive evidence, it may be argued that a history of malignancy
does not necessarily suggest that a nasal vestibular lesion is
primary in nature. It is well-known among pathologists that there
are currently no immunohistochemical markers for the determination
of the likely site of origin of SCC, although this is feasible for
adenocarcinomas in the majority of cases (19). Some related and heuristic studies have
been performed in recent years. For example, Huang et al
performed immunohistochemical staining to compare the expression
profile of the epithelial-mesenchymal transition markers between a
metastatic lesion of the duodenum and primary SCC of the
hypopharynx (20). Therefore, the
differentiation between primary and metastatic nasal vestibular SCC
currently depends mainly on clinical and histological examination.
The clinical and histological evidence confirmed that the second
tumor of the nasal vestibule was primary in this case. Based on
these results, the patient was diagnosed with double primary cancer
of the lung and nasal vestibule.
The incidence of second cancers has increased
(21–23). A study on data from the European
cancer registry reported an overall incidence of double primary
cancer of 6.3% (range, 0.4–12.9%) (24); Utada et al reported that the
proportion of patients with a second primary tumor during the
follow-up period was 8.1% (median, 1.8 years; mean, 4.3 years)
(25). Filali et al reported
variable proportions of double primary cancer, ranging between 6.1
and 10.5% (26). Furthermore, the
risk of second primary cancer among cancer patient was higher
compared with the risk of cancer in the general population
(21–22,27–28). For
example, among second primary cancers, 19.0% were diagnosed within
3 months after the diagnosis of the first primary cancer (25). Another study reported that cancer
patients in Connecticut had a 31% higher risk of developing a
subsequent cancer (28). The
increased incidence is not only due to the population aging, but it
may also be attributed to the advances in medical technology,
particularly diagnostic techniques and cancer treatment modalities
(29). The mechanism underlying the
development of multiple primary cancers has not been fully
elucidated; it may be related to the late effects of treatment for
the first primary cancer, or risk factors common to the first and
subsequent primary cancer, such as environmental and lifestyle
factors, prolonged exposure to carcinogens, radiotherapy and
chemotherapy, cellular and humoral immunity deficit and individual
genetic susceptibility (30–33).
Our patient underwent major invasive surgery for
lung cancer. In addition, he received one cycle of adjuvant
chemotherapy, which weakened the body's immune system, increasing
the risk of cancer. Other important factors were the 20-year
history of heavy smoking and alcohol consumption. A study reported
that the major risk factor shared between first and second primary
cancers is smoking; a synergetic effect between smoking and
drinking may also contribute to the development of multiple primary
cancers (34–36). However, a definitive causative factor
of double primary cancer has not been clearly determined; further
detailed investigation on protective and risk factors is
required.
For SCC of the lung, platinum-based regimens are
considered as the mainstay of treatment (37). However, in our patient, although
nedaplatin and gemcitabine are effective in the treatment of SCC of
lung cancer, they confer no therapeutic benefit for SCC of the
nasal vestibule. Wray et al (9) evaluated the University of Florida
treatment of nasal vestibular carcinoma over a period of >40
years and reported excellent disease control with radiotherapy
alone in patients with T1-T2 and favorable T3-T4. Radiotherapy and
surgery result in improved likelihood of cure for patients with
advanced T4 lesions. Vital et al (38) reported that radiotherapy is a valuable
alternative treatment option avoiding potential cosmetic
disadvantages. Thus, we recommend treatment with radiotherapy
rather than chemotherapy for patients with SCC of the nasal
vestibule. Planning to receive treatment at a local hospital, the
patient was discharged. After 2 months of follow-up, the volume of
the nose tumor was significantly reduced through radiotherapy and
immunity-enhancing treatment.
A study in Japan reported that the esophagus, ovary,
larynx, pharynx and mouth were the most frequent sites for
developing a second primary cancer (21). In Queensland, Australia, from 1997 to
2001, second primary cancers of the head and neck were frequent,
whereas those of the esophagus and ovary were not as common
(22). However, the most common sites
for occurrence second primary cancer may not be as important; all
clinicians should bear in mind that, when a cancer patient is
experiencing discomfort in these sites, the possibility of double
or multiple primary cancers must be considered and the frequency of
medical examinations and complementary tests must be increased,
with the aim to improve the diagnostic rate of such patients and
avoid misdiagnosis and treatment delay. Although multiple primary
cancers have rarely been reported in China, their incidence is
considered to be on the increase. Early detection is crucial to
provide optimal treatment and improve the survival rate of cancer
patients.
In conclusion, cancer patients are at a higher risk
of a second primary cancers than the general population. The
esophagus, ovary, and head and neck were the most frequent sites
for developing a second primary cancer. Therefore, cancer patients
should be under close scrutiny, particularly shortly after the
diagnosis of their first primary cancer. early detection of a
silent tumor is meaningful in selecting the optimal treatment
option available. Platinum-based chemotherapy is the mainstay of
treatment in SCC of the lung; however, for SCC of the head and
neck, treatment with radiotherapy is recommended.
Written informed consent was obtained from the
patient for publication of this case report and any accompanying
images.
References
|
1
|
Moertel CG, Dockerty MB and Baggenstoss
AH: Multiple primary malignant neoplasms. II. Tumors of different
tissues or organs. Cancer. 14:231–237. 1961. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Billroth T: General surgical pathology and
therapeutics in 51 Vorlesungen: A textbook for students and
physicians in fifty-one lectures (14th). Berlin, DE: G. Rerimer.
1889.
|
|
3
|
Warren S and Gates O: Multiple primary
malignant tumors: Surgery of literature and statistical study. Am J
Cancer. 16:1358–1414. 1932.
|
|
4
|
Tsukuma H, Fujimoto I, Hanai A, Hiyama T,
Kitagawa T and Kinoshita N: Incidence of second primary cancers in
Osaka residents, Japan, with special reference to cumulative and
relative risks. Jpn J Cancer Res. 85:339–345. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jemal A, Bray F, Center M, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rossi A, Chiodini P, Sun JM, O'Brien ME,
von Plessen C, Barata F, Park K, Popat S, Bergman B, Parente B, et
al: Six versus fewer planned cycles of first-line platinum-based
chemotherapy for non-small-cell lung cancer: A systematic review
and meta-analysis of individual patient data. Lancet Oncol.
15:1254–1262. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Thanendrarajan S, Nowak M, Abken H and
Schmidt-Wolf IG: Combining cytokine-induced killer cells with
vaccination in cancer immunotherapy: More than one plus one. Leuk
Res. 35:1136–1142. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Han RX, Liu X, Pan P, Jia YJ and Yu JC:
Effectiveness and safety of chemotherapy combined with dendritic
cells co-cultured with cytokine-induced killer cells in the
treatment of advanced non-small-cell lung cancer: A systematic
review and meta-analysis. PLoS One. 9:e1089582014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wray J, Morris CG, Kirwan JM, Amdur RJ,
Werning JW, Dziegielewski PT and Mendenhall WM: Radiation therapy
for nasal vestibule squamous cell carcinoma: A 40-year experience.
Eur Arch Otorhinolaryngol. 2015 Mar 13;(Epub ahead of print).
PubMed/NCBI
|
|
10
|
Jeannon JP, Riddle PJ, Irish J, O'sullivan
B, Brown DH and Gullane P: Prognostic indicators in carcinoma of
the nasal vestibule. Clin Otolaryngol. 32:19–23. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kummer E, Rasch CR, Keus RB, Tan IB and
Balm AJ: T stage as prognostic factor in irradiated localized
squamous cell carcinoma of the nasal vestibule. Head Neck.
24:268–273. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Agger A, von Buchwald C, Madsen AR, Yde J,
Lesnikova I, Christensen CB, Foghsgaard S, Christensen TB, Hansen
HS, Larsen S, et al: Squamous cell carcinoma of the nasal vestibule
1993–2002: A nationwide retrospective study from DAHANCA. Head
Neck. 31:1593–1599. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wong CS, Cummings BJ, Elhakim T and Briant
TD: External irradiation for squamous cell carcinoma of the nasal
vestibule. Int J Radiat Oncol Biol Phys. 12:1943–1946. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Patel P, Tiwari R, Karim AB, Nauta JJ and
Snow GB: Squamous cell carcinoma of the nasal vestibule. J Laryngol
Otol. 106:332–336. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Fornelli RA, Fedok FG, Wilson EP and
Rodman SM: Squamous cell carcinoma of the anterior nasal cavity: A
dual institution review. Otolaryngol Head Neck Surg. 123:207–210.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Samaha M, Yoskovitch A, Hier MP and Black
MJ: Squamous cell carcinoma of the nasal vestibule. J Otolaryngol.
29:98–101. 2000.PubMed/NCBI
|
|
17
|
Dowley A, Hoskison E, Allibone R and Jones
NS: Squamous cell carcinoma of the nasal vestibule: A 20-year case
series and literature review. J Laryngol Otol. 122:1019–1023. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Quinn FB Jr and Mccabe BF: Laryngeal
metastases from malignant tumors in distant organs. Ann Otol Rhinol
Laryngol. 66:139–143. 1957.PubMed/NCBI
|
|
19
|
Oien KA: Pathologic evaluation of unknown
primary cancer. Semin Oncol. 36:8–37. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Huang YC, Chang PM, Lee IC, Yang CF, Tzeng
CH and Yang MH: Duodenal squamous cell carcinoma derived from the
hypopharynx: Immunohistochemical assessment of metastatic
mechanisms. Gastrointest Endosc. 72:460–463. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tabuchi T, Ito Y, Ioka A, Miyashiro I and
Tsukuma H: Incidence of metachronous second primary cancers in
Osaka, Japan: Update of analyses using population-based cancer
registry data. Cancer Sci. 103:1111–1120. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Youlden DR and Baade PD: The relative risk
of second primary cancers in Queensland, Australia: A retrospective
cohort study. BMC Cancer. 11:832011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Freeman HJ: Triple metachronous colon
cancer. World J Gastroenterol. 19:4443–4444. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rosso S, De Angelis R, Ciccolallo L,
Carrani E, Soerjomataram I, Grande E, Zigon G and Brenner H:
EUROCARE Working Group: Multiple tumours in survival estimates. Eur
J Cancer. 45:1080–1094. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Utada M, Ohno Y, Hori M and Soda M:
Incidence of multiple primary cancers and interval between first
and second primary cancers. Cancer Sci. 105:890–896. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Filali K, Hédelin G, Schaffer P, Estève J,
Arveux P, Bouchardy C, Exbrayat C, Faivre J, Lévi F, Macé-Lesech J,
et al: Multiple primary cancers and estimation of the incidence
rates and trends. Eur J Cancer. 32A:683–690. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Crocetti E, Buiatti E and Falini P:
Italian Multiple Primary Cancer Working Group: Multiple primary
cancer incidence in Italy. Eur J Cancer. 37:2449–2456. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Curtis RE, Boice JD Jr, Kleinerman RA,
Flannery JT and Fraumeni JF Jr: Summary: Multiple primary cancers
in Connecticut 1935–82. Natl Cancer Inst Monogr. 68:219–242.
1985.PubMed/NCBI
|
|
29
|
Ikeda Y, Tsukuda M, Ishitoya J, Arai Y,
Matsuda H, Katori H, Taguchi T, Yoshida T, Ono M, Sakuma Y, et al:
Four cases of simultaneous triple primary cancers of the
hypopharynx, esophagus and stomach. Otolaryngol Head Neck Surg.
132:788–793. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Travis LB, Rabkin CS, Brown LM, Allan JM,
Alter BP, Ambrosone CB, Begg CB, Caporaso N, Chanock S, DeMichele
A, et al: Cancer survivorship - genetic susceptibility and second
primary cancers: Research strategies and recommendations. J Natl
Cancer Inst. 98:15–25. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Travis LB: The epidemiology of second
primary cancers. Cancer Epidemiol Biomarkers Prev. 15:2020–2067.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kuligina E, Reiner A, Imyanitov EN and
Begg CB: Evaluating cancer epidemiologic risk factors using
multiple primary malignancies. Epidemiology. 21:366–372. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Jiao F, Hu H and Wang LW: Quadruple
primary malignancy patient with survival time more than 20 years.
World J Gastroenterol. 19:1498–1501. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Adami HO, Hunter D and Trichopoulos D:
Textbook of cancer epidemiology (2nd). Oxford University Press. New
York: 2002.
|
|
35
|
Hiyama T, Sato T, Yoshino K, Tsukuma H,
Hanai A and Fujimoto I: Second primary cancer following laryngeal
cancer with special reference to smoking habits. Jpn J Cancer Res.
83:334–339. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Botteri E, Iodice S, Bagnardi V, Raimondi
S, Lowenfels AB and Maisonneuve P: Smoking and colorectal cancer: A
meta-analysis. JAMA. 300:2765–2778. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
DeVita VT Jr and Rosenberg SA: Two hundred
years of cancer research. N Engl J Med. 366:2207–2214. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Vital D, Morand G, Huber GF, Studer G and
Holzmann D: Outcome in squamous cell carcinoma of the nasal
vestibule: A single center experience. Head Neck. 37:46–51. 2015.
View Article : Google Scholar : PubMed/NCBI
|