Introduction
Thymic tumors, consisting of thymoma and thymic
carcinoma, are rare neoplasms that arise in the anterior
mediastinum. Thymic carcinomas have malignant cytological features
with aggressive invasion of mediastinal organs, resulting in a poor
outcome, whereas thymomas are generally considered to be
cytologically benign (1,2).
Surgery is indicated as the initial treatment for
cases in which complete resection is considered feasible. For
patients who are not operable, radiation therapy and/or
chemotherapy may be indicated for symptom control and potentially
prolonged survival rates (3). Owing
to the rarity of thymic carcinoma, however, a standard chemotherapy
regimen remains to be established.
Nanoparticle albumin-bound paclitaxel (nab-PAC), an
albumin-bound, 130 nm particle form of paclitaxel, was developed to
avoid Cremophor/ethanol-associated toxicities for solvent-based
paclitaxel (sb-PAC), and to exploit albumin receptor-mediated
endothelial transport (4). Promising
activity was demonstrated in patients with non-small cell lung
cancer (NSCLC), breast cancer and gastric cancer (5–7). In the
present study, a case of lymphoepithelioma-like thymic carcinoma is
described, refractory to carboplatin plus sb-PAC (CP) treatment,
but which responded to subsequent treatment with carboplatin plus
nab-PAC.
Case report
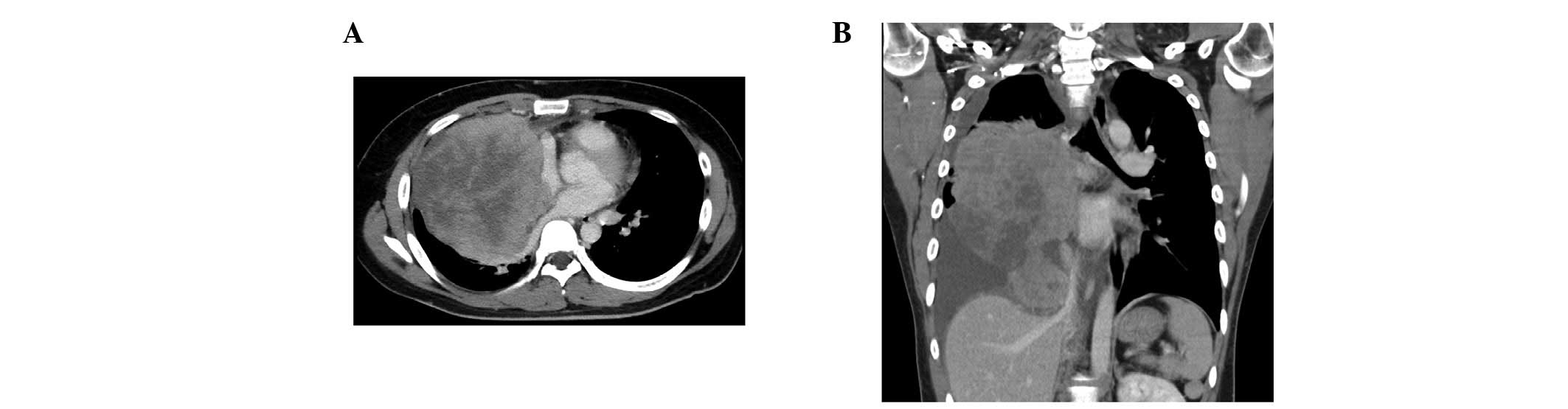
A 22-year-old man presented with progressive chest
pain, dyspnea and body weight loss. Contrast-enhanced computed
tomography (CT) using an Aquillion™ One CT scanner (Toshiba, Tokyo,
Japan) revealed a 20×10 cm irregular tumor in the right thorax with
pleural dissemination and invasion to the brachiocephalic trunk,
right pulmonary artery, trachea and epicardium (Fig. 1).
Fluorodeoxyglucose (FDG) positron-emission CT
(Discovery IQ; GE Healthcare, Buckinghamshire, UK) demonstrated
marked FDG accumulation in the tumor. CT-guided needle biopsy of
the tumor was performed. The tissue was fixed in 10%
neutral-buffered formalin, and embedded in paraffin. A 3 µm-thick
section of the paraffin block was stained with hematoxylin and
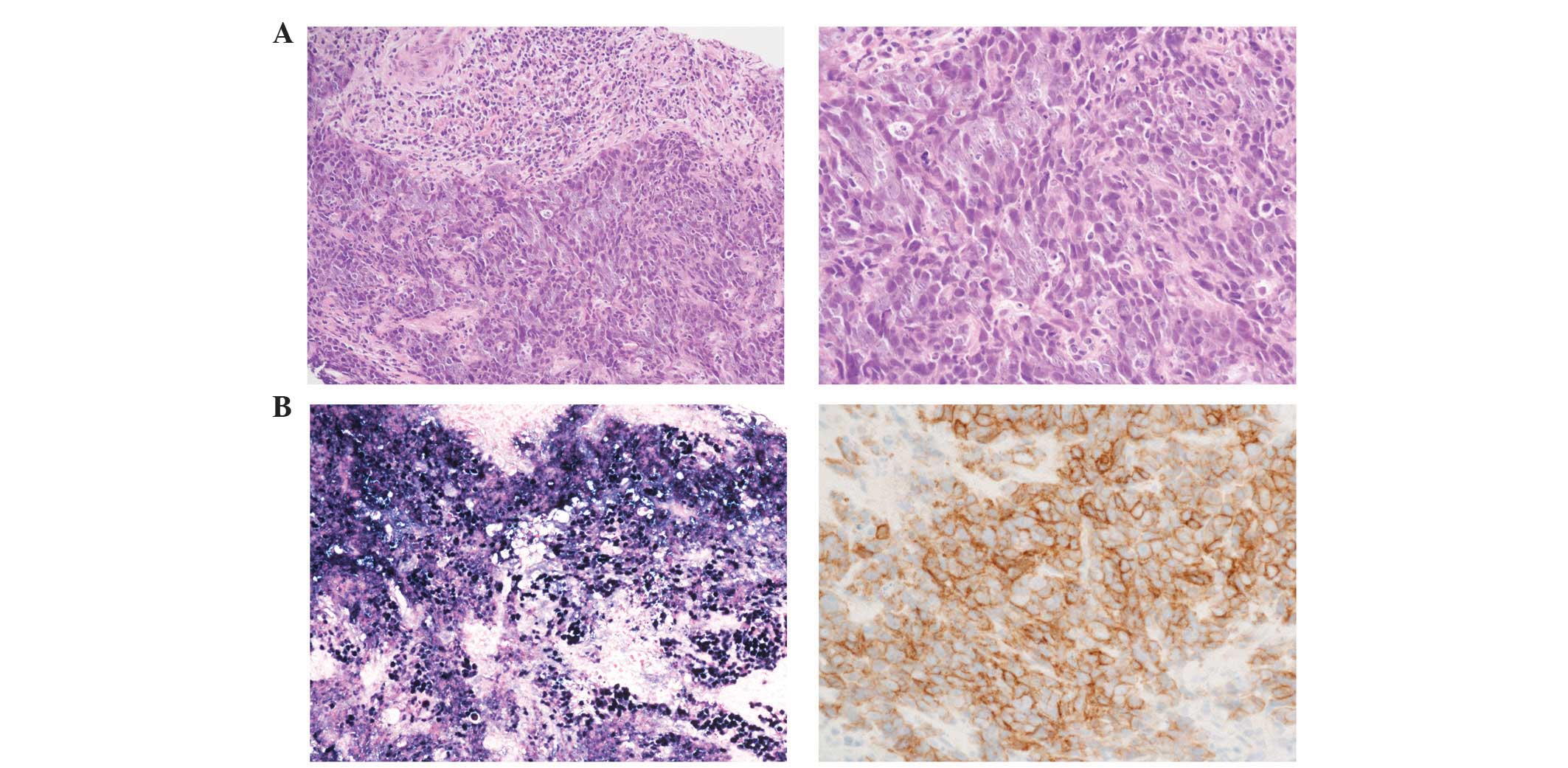
eosin, and used for immunohistochemistry. Histologically, the tumor
was composed of nests and sheets of malignant cells with the
infiltration of lymphocytes (Fig.
2A). The tumor cells exhibited a high nuclear/cytoplasmic ratio
and large vesicular nuclei with distinct nucleoli.
Immunohistochemical staining was performed on a Ventana BenchMark
URTLA instrument (Ventana Medical Systems, Inc., Tucson, AZ, USA).
CAM5.2 (clone cytokeratin 8, 1:500, B.D. 349205), cluster of
differentiation 5 (CD5; clone 4C7, 1:50, Leika NCL-CD5-4C7), CD117
(polyclonal, 1:200, Dako A4502) and EBER [Epstein-Barr virus
(EBV)-encoded small RNA] in situ hybridization (ISH; Roche
518-102524) were selected as diagnostic markers.
Immunohistochemical staining revealed that the tumor cells were
positive for cytokeratin CAM5.2, CD117 and the EBV-encoded small
RNA, but were negative for CD5 (Fig.
2B). On the basis of these findings, the patient was diagnosed
with lymphoepithelioma-like thymic carcinoma, stage IVa, in
accordance with the Masaoka-Koga staging system (8).
As the initial therapy, palliative radiotherapy (45
Gy) for the mediastinal area in combination with weekly carboplatin
[dose calculation: Area under curve (AUC) 2] plus sb-PAC (40
mg/m2) was started to palliate the airway obstruction
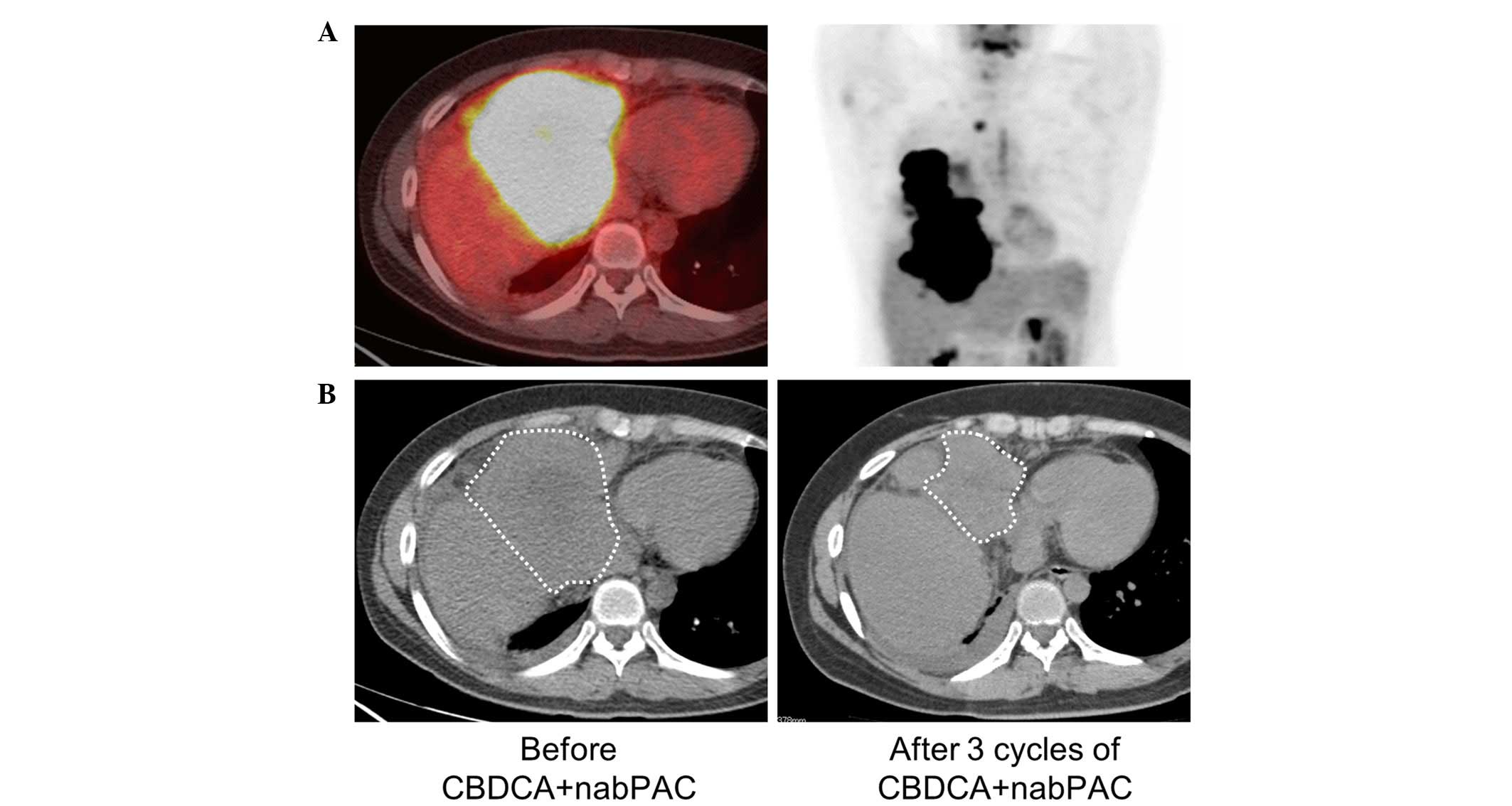
and dyspnea. When the palliative radiotherapy was completed,
despite the reduction in tumor size, liver invasion was
subsequently demonstrated using FDG positron emission CT (Fig. 3A). Subsequently, chemotherapy with
carboplatin (AUC 6, day 1) and nab-PAC (100 mg/m2, days
1, 8 and 15) every 3 weeks was started. Since only grade 3
neutropenia, but no other severe adverse effects, was observed, no
dose reduction was required. Objective tumor size reduction
(partial response) was obtained following three cycles of
chemotherapy (Fig. 3B).
Discussion
Thymic carcinoma is a rare neoplasm, with a poor
outcome due to its aggressive characteristics. For patients who are
not operable, radiation therapy and/or palliative chemotherapy are
indicated (1). Since a standard
chemotherapy regimen for thymic carcinoma remains to be
established, the present case report implies that carboplatin plus
nab-PAC is a promising therapy for patients with thymic
carcinoma.
In the National Comprehensive Cancer Network
guidelines for thymoma and thymic carcinoma, CP is recommended as
the first-line chemotherapy in patients with advanced-stage thymic
carcinoma (3). Two phase II studies
by Lemma et al (9) and Hirai
et al (10) revealed that
patients with advanced-stage thymic carcinoma had a favorable
response to CP (overall response rate of 22 and 36%, respectively)
compared with the response in other studies (11–18). There
have been no prospective large-scale trials addressing the optimal
chemotherapy regimen for patients with thymic carcinoma, due to the
rarity of this disease.
CP regimens occasionally cause severe sensory
neuropathy, resulting in dose reduction and/or treatment
termination. In the study of Lemma et al (9), grade 3 sensory neuropathy was observed
in 13.3% [and the rate of discontinuation of treatment for toxicity
was considerably higher (~21%)] of the patients with either thymoma
or thymic carcinoma receiving the CP regimen (9).
Nab-PAC, the 130 nm albumin-bound paclitaxel
formulation, is a promising novel agent with lower toxicity and
higher accumulation in tumors compared with sb-PAC. In a
preclinical in vivo study, increased antitumor activity of
nab-PAC was reported, with a 33% higher paclitaxel concentration in
tumors compared with sb-PAC (4). A
phase III trial for patients with advanced NSCLC revealed that the
administration of carboplatin plus nab-PAC as a first-line therapy
resulted in a significantly lower rate of sensory neuropathy, 26%
greater dose intensity, and a higher objective response rate (33
vs. 25%; P=0.005) compared with CP (5). In the current case study, weekly CP was
administered in combination with palliative radiotherapy due to the
safe profile of CP when administered with concurrent radiotherapy.
Notably, the tumor responded to subsequent chemotherapy with
carboplatin and nab-PAC, despite progression during the treatment
with weekly CP. A high accumulation of nab-PAC in the tumor and
high dose intensity may have contributed to the response.
According to the World Health Organization
classification, there are 13 subtypes of thymic carcinoma: 60–70%
of all thymic carcinomas are subtypes of squamous cell carcinoma
and lymphoepithelioma-like carcinoma. The lymphoepithelioma-like
carcinoma is a classically common, although now rare, subtype
(1.0–8.2%), with poor prognosis, being associated with Epstein-Barr
virus infection (19–25). A histological difference appears to be
associated with the response to nab-PAC: A subset analysis of a
phase III study in patients with NSCLC revealed that squamous cell
carcinoma responded markedly well to carboplatin plus nab-PAC
(5). In thymic carcinoma, two cases
receiving carboplatin plus nab-PAC and exhibiting a favorable
response were previously reported, and notably, the two cases were
presented as squamous cell carcinomas (26,27). The
current case study describes, to the best of our knowledge, the
first patient with thymic lymphoepithelioma-like subtype who
responded to carboplatin plus nab-PAC. A response to nab-PAC, in
association with the histological subtype, in thymic carcinoma
should be discussed in the future.
In conclusion, a case of thymic carcinoma with
lymphoepithelioma-like histology that responded to treatment with
carboplatin plus nab-PAC has been presented in the current study.
Considering that a standard treatment has yet to be established in
patients with thymic carcinoma, nab-PAC may merit further
investigation in this rare, but aggressive disease.
References
|
1
|
Falkson CB, Bezjak A, Darling G, Gregg R,
Malthaner R, Maziak DE, Yu E, Smith CA, McNair S, et al: The
management of thymoma: A systematic review and practice guideline.
J Thorac Oncol. 4:911–919. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Eng TY, Fuller CD, Jagirdar J, Bains Y and
Thomas CR Jr: Thymic carcinoma: State of the art review. Int J
Radiat Oncol Biol Phys. 59:654–664. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
NCCN guidelines on the treatment of
thymomas and thymic carsinomas. Version 1. 2014.http://www.nccn.org/professionals/physician_gls/pdf/thymic.pdfAccessed.
July 05–2015
|
|
4
|
Desai N, Trieu V, Yao Z, Louie L, Ci S,
Yang A, Tao C, De T, Beals B, Dykes D, et al: Increased antitumor
activity, intratumor paclitaxel concentrations and endothelial cell
transport of cremophor-free, albumin-bound paclitaxel, ABI-007,
compared with cremophor-based paclitaxel. Clin Cancer Res.
12:1317–1324. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Socinski MA, Bondarenko I, Karaseva NA,
Makhson AM, Vynnychenko I, Okamoto I, Hon JK, Hirsh V, Bhar P,
Zhang H, et al: Weekly nab-paclitaxel in combination with
carboplatin versus solvent-based paclitaxel plus carboplatin as
first-line therapy in patients with advanced non-small-cell lung
cancer: Final results of a phase III trial. J Clin Oncol.
30:2055–2062. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gradishar WJ, Tjulandin S, Davidson N,
Shaw H, Desai N, Bhar P, Hawkins M and O'Shaughnessy J: Phase III
trial of nanoparticle albumin-bound paclitaxel compared with
polyethylated castor oil-based paclitaxel in women with breast
cancer. J Clin Oncol. 23:7794–7803. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Koizumi W, Morita S and Sakata Y: A
randomized Phase III trial of weekly or 3-weekly doses of
nab-paclitaxel versus weekly doses of Cremophor-based paclitaxel in
patients with previously treated advanced gastric cancer (ABSOLUTE
Trial). Jpn J Clin Oncol. 45:303–306. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Masaoka A, Monden Y, Nakahara K and
Tanioka T: Follow-up study of thymomas with special reference to
their clinical stages. Cancer. 48:2485–2492. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lemma GL, Lee JW, Aisner SC, Langer CJ,
Tester WJ, Johnson DH and Loehrer PJ Sr: Phase II study of
carboplatin and paclitaxel in advanced thymoma and thymic
carcinoma. J Clin Oncol. 29:2060–2065. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hirai F, Yamanaka T, Taguchi K, Daga H,
Ono A, Tanaka K, Kogure Y, Shimizu J, Kimura T, Fukuoka J, et al: A
multicenter phase II study of carboplatin and paclitaxel for
advanced thymic carcinoma: WJOG4207L. Ann Oncol. 26:363–368. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Koizumi T, Takabayashi Y, Yamagishi S,
Tsushima K, Takamizawa A, Tsukadaira A, Yamamoto H, Yamazaki Y,
Yamaguchi S, Fujimoto K, et al: Chemotherapy for advanced thymic
carcinoma: Clinical response to cisplatin, doxorubicin, vincristine
and cyclophosphamide (ADOC chemotherapy). Am J Clin Oncol.
25:266–268. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kanda S, Koizumi T, Komatsu Y, Yoshikawa
S, Okada M, Hatayama O, Yasuo M, Tsushima K, Urushihata K, Kubo K,
et al: Second-line chemotherapy of platinum compound plus CPT-11
following ADOC chemotherapy in advanced thymic carcinoma: Analysis
of seven cases. Anticancer Res. 27:3005–3008. 2007.PubMed/NCBI
|
|
13
|
Komatsu Y, Koizumi T, Tanabe T, Hatayama
O, Yasuo M, Okada M, Yamamoto H, Kubo K, Sasabayashi M and Tsunoda
T: Salvage chemotherapy with carboplatin and paclitaxel for
cisplatin-resistant thymic carcinoma-three cases. Anticancer Res.
26:4851–4855. 2006.PubMed/NCBI
|
|
14
|
Weide LG, Ulbright TM, Loehrer PJ Sr and
Williams SD: Thymic carcinoma. A distinct clinical entity
responsive to chemotherapy. Cancer. 71:1219–1223. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yoh K, Goto K, Ishii G, Niho S, Ohmatsu H,
Kubota K, Kakinuma R, Nagai K, Suga M and Nishiwaki Y: Weekly
chemotherapy with cisplatin, vincristine, doxorubicin and etoposide
is an effective treatment for advanced thymic carcinoma. Cancer.
98:926–931. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lucchi M, Mussi A, Ambrogi M, Gunfiotti A,
Fontanini G, Basolo F and Angeletti CA: Thymic carcinoma: A report
of 13 cases. Eur J Surg Oncol. 27:636–640. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Igawa S, Murakami H, Takahashi T, Nakamura
Y, Tsuya A, Naito T, Kaira K, Ono A, Shukuya T, Tamiya A, et al:
Efficacy of chemotherapy with carboplatin and paclitaxel for
unresectable thymic carcinoma. Lung Cancer. 67:194–197. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Maruyama R, Suemitsu R, Okamoto T, Kojo M,
Aoki Y, Wataya H, Eguchi T, Nishiyama K, Seto T and Ichinose Y:
Persistent and aggressive treatment for thymic carcinoma. Results
of a single-institute experience with 25 patients. Oncology.
70:325–329. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Leyvraz S, Henle W, Chahinian AP, Perlmann
C, Klein G, Gordon RE, Rosenblum M and Holland JF: Association of
Epstein-Barr virus with thymic carcinoma. N Engl J Med.
312:1296–1299. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Schirosi L, Nannini N, Nicoli D, Cavazza
A, Valli R, Buti S, Garagnani L, Sartori G, Calabrese F, Marchetti
A, et al: Activating c-KIT mutations in a subset of thymic
carcinoma and response to different c-KIT inhibitors. Ann Oncol.
23:2409–2414. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kondo K and Monden Y: Therapy for thymic
epithelial tumors: A clinical study of 1,320 patients from Japan.
Ann Thorac Surg. 76:878–884; discussion 884–885. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Okuma Y, Hosomi Y, Takahashi S, Maeda Y,
Okamura T and Hishima T: Response to cytotoxic chemotherapy in
patients previously treated with palliative-intent chemotherapy for
advanced thymic carcinoma. Clin Lung Cancer. 16:221–227. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Li W, Miao Z, Liu X, Zhang Q, Sun L, Li P,
Liu W and Zhang L: Thymic carcinoma patients with myasthenia gravis
exhibit better prognoses. Int J Clin Oncol. 2015 Jul 3;[Epub ahead
of print].
|
|
24
|
Filosso PL, Guerrera F, Rendina AE, Bora
G, Ruffini E, Novero D, Ruco L, Vitolo D, Anile M, Ibrahim M, et
al: Outcome of surgically resected thymic carcinoma: A multicenter
experience. Lung Cancer. 83:205–210. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wang S, Wang Z, Liu X, Wang D and Liu F:
Prognostic factors of patients with thymic carcinoma after surgery:
A retrospective analysis of 58 cases. World J Surg. 38:2032–2038.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Makimoto G, Fujiwara K, Watanabe H,
Kameyama N, Matsushita M, Rai K, Sato K, Yonei T, Sato T and
Shibayama T: nab-Paclitaxel in combination with carboplatin for a
previously treated thymic carcinoma. Case Rep Oncol. 7:14–17. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhan P, Xie H and Yu LK: Response to
nab-paclitaxel and nedaplatin in a heavily-metastatic thymic
carcinoma: A case report. Oncol Lett. 9:1715–1718. 2015.PubMed/NCBI
|