Introduction
As gastroesophageal reflux disease is highly
prevalent among the elderly (1) and
peptic ulcer and diffuse erosive gastritis are not uncommon among
cancer patients who are under severe mental stress (2), acid suppressant (AS) therapy with a
histamine type-2 receptor antagonist (H2RA) and/or a proton pump
inhibitor (PPI) are usually prescribed in these patients. Although
not common, dyspepsia and abdominal discomfort are two of the
possible adverse effects of epidermal growth factor receptor
tyrosine kinase inhibitors (EGFR-TKIs) (3). Therefore, drug interactions between AS
and TKIs are a clinical issue in the management of patients treated
with TKIs. During preclinical evaluation, one of the TKIs,
erlotinib, was found to exhibit pH-dependent solubility, with a
dissociation constant of 5.4 (3).
This pH-dependent solubility was reflected in a study that compared
its plasma concentrations in healthy subjects who were or were not
receiving AS therapy (4). In
addition, the H2RA ranitidine decreased the median area under the
curve (AUC) of erlotinib by 33% (3).
Recently, two clinical evaluations of the interaction between AS
therapy and erlotinib have been reported, and they reported
opposing findings, namely that AS therapy was associated with
decreased erlotinib efficacy (5) and
that there was no such an association (6). These studies included patients with
unknown EGFR mutation status and only evaluated the efficacy of
erlotinib therapy (5,6). On the other hand, however, Ter Heine
et al reported lower than expected erlotinib trough
concentrations in a patient who received pantoprazole, an
intravenous PPI, but this discrepancy was not observed when oral
pantoprazole was prescribed (7). The
EGFR mutation status was not described in that case report.
In the present study, we investigated whether oral
AS therapy is truly associated with decreased efficacy of gefitinib
and erlotinib, particularly in patients with mutated EGFR.
Patients and methods
Patients
A total of 46 consecutive patients with
pathologically confirmed non-small-cell lung cancer (NSCLC), who
were treated with TKIs at the Ryugasaki Saiseikai General Hospital
and the Mito Medical Center between September, 2005 and May, 2013,
were retrospectively analyzed. The histopathological diagnoses were
performed according to the World Health Organization classification
system (8) and the patients were
staged according to the Union for International Cancer Control
tumor-node-metastasis staging system (9).
The patient characteristics and the treatment
efficacy and safety were evaluated using patient data extracted
from the database of each participating institution. Tumor response
was classified as complete response, partial response, stable
disease, progressive disease or not evaluable, according to the
Response Evaluation Criteria in Solid Tumors, version 1.1 (10).
We next evaluated the TKI dose prescribed and
patient survival, taking body surface area (BSA) into
consideration. Briefly, we defined relative dose of TKI as the
prescribed dose divided by the full dose (gefitinib, 250 mg;
erlotinib, 150 mg). In addition, we divided the relative dose of
TKI by BSA and evaluated the association between relative dose of
TKI/BSA and survival of patients with or without AS treatment.
The present retrospective study conformed to the
Ethical Guidelines for Clinical Studies issued by the Ministry of
Health, Labor and Welfare of Japan. Ethical approval of this study
was obtained from the Institutional Review Board of the Ryugasaki
Saiseikai Hospital (Ryugasaki, Japan).
Statistical analysis
Statistical significance was determined using the
Mann-Whitney U test and the Chi-square test. Survival time was
calculated from the day of TKI initiation to death or last
follow-up. The survival rate was analyzed with the Kaplan-Meier
method and comparisons were performed using the log-rank test.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Patient characteristics
During the study period, a total of 46 patients were
treated with TKIs (29 with gefitinib and 17 with erlotinib). Of the
46 patients, 11 received AS treatment and 35 did not. The
characteristics of EGFR-mutated NSCLC patients with or without AS
treatment are summarized in Table I.
As regards age, gender, smoking history, performance status, cancer
histology, clinical stage, BSA and type of EGFR mutation, there
were no statistically differences between the two groups.
 | Table I.Characteristics of EGFR-mutated NSCLC
patients with or without acid suppressant (AS) treatment. |
Table I.
Characteristics of EGFR-mutated NSCLC
patients with or without acid suppressant (AS) treatment.
| Characteristics | With AS (n=11) | Without AS
(n=35) | P-value |
|---|
| Age, years [median
(range)] | 74 (52–88) | 77 (52–89) | 0.708 |
| Gender |
|
| 1.000 |
| Male | 2 | 9 |
|
|
Female | 9 | 26 |
|
| Smoking history |
|
| 0.559 |
| Never
smokers | 11 | 31 |
|
|
Current/former smoker | 0 | 4 |
|
| ECOG performance
status |
|
| 0.433 |
| 0–1 | 10 | 31 |
|
| 2–4 | 1 | 4 |
|
| Histology |
|
| 0.138 |
|
Adenocarcinoma | 9 | 34 |
|
|
Others | 2 | 1 |
|
| Stage |
|
| 1.000 |
| IIIA | 2 | 8 |
|
| IV | 9 | 27 |
|
| Body surface area,
m2 [median (range)] | 1.42 (1.11–1.86) | 1.41 (1.17–1.83) | 0.588 |
| EGFR mutation |
|
| 0.133 |
| Exon 19
deletion | 9 | 15 |
|
| Exon21
L858R | 2 | 18 |
|
|
Others | 0 | 2 |
|
TKI therapy
The characteristics of TKI therapy are shown in
Table II. There were no
statistically significant differences in terms of TKI prescribed,
dose reduction, prior therapy and relative dose of TKI/BSA between
patients with and those without AS treatment.
| Table II.Prescribed TKIs, dose reduction, prior
therapy and % of initial dose/BSA in patients with or without AS
treatment. |
Table II.
Prescribed TKIs, dose reduction, prior
therapy and % of initial dose/BSA in patients with or without AS
treatment.
| Variables | With AS | Without AS | P-value |
|---|
| Prescribed TKI
(patient no.) |
|
| 0.501 |
|
Gefitinib | 8 | 21 |
|
|
Erlotinib | 3 | 14 |
|
| TKI dose
reduction |
|
| 0.2419 |
|
Present | 2 | 13 |
|
|
Absent | 9 | 22 |
|
| Prior therapy |
|
| 0.282 |
|
Present | 4 | 14 |
|
|
Absent | 7 | 21 |
|
| % of initial dose/BSA
(%/m2) |
|
| 0.471 |
| Median
(range) | 70.4 (48.9–90.1) | 70.9 (47.5–85.5) |
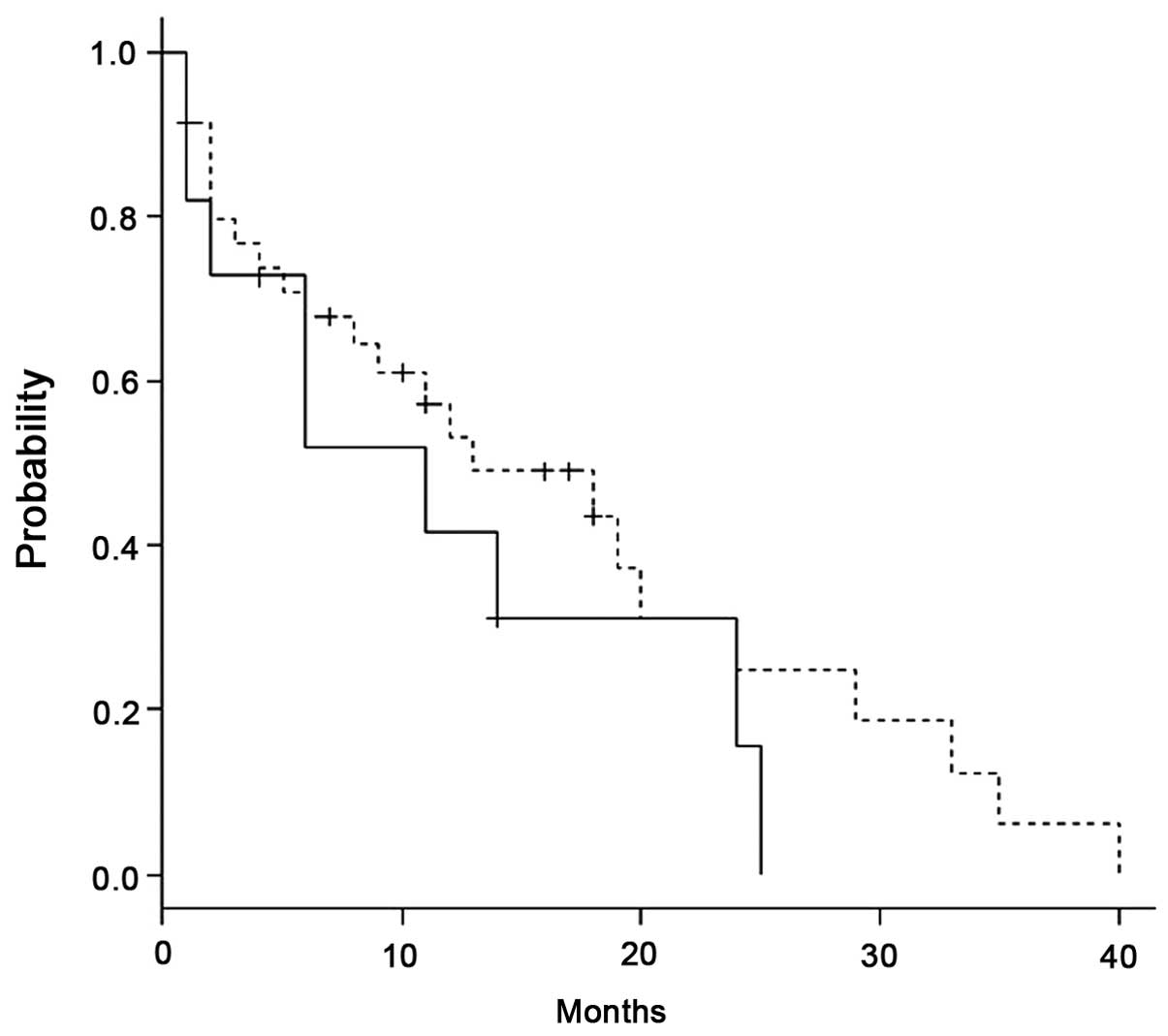
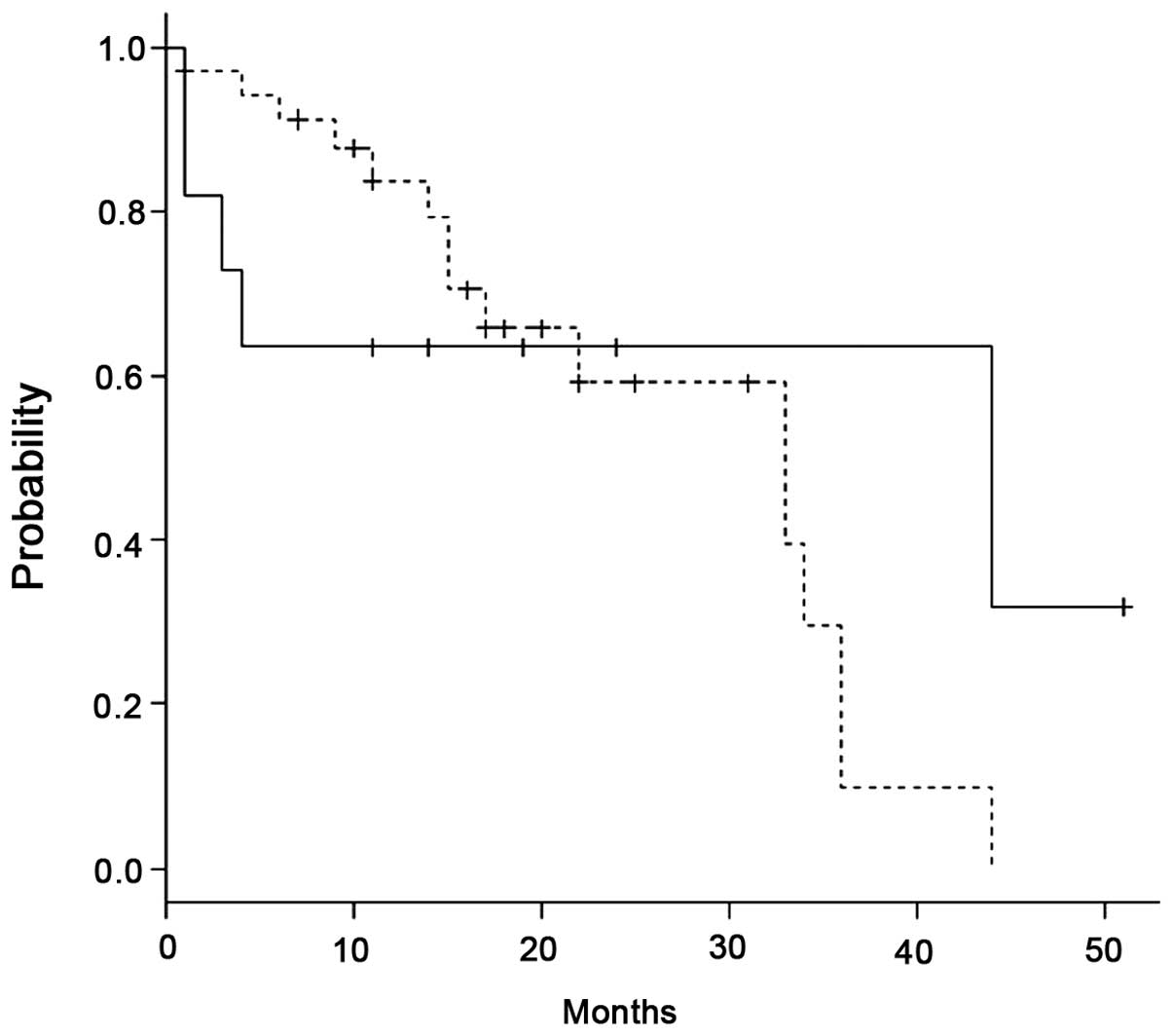
Survival analysis
There were no statistically significant differences
in PFS between the 11 patients with AS and the 35 patients without
AS treatment (Fig. 1) (P=0.296). OS
also did not differ significantly between the two groups (Fig. 2) (P=0.613).
Association between relative dose of
TKI/BSA and survival
We next evaluated the association between the
relative dose of TKI/BSA and survival in NSCLC patients with or
without AS treatment. The median of the relative dose of TKI/BSA in
patients with AS and those without AS was 70.4 and 70.9
%/m2, respectively (Table
II); therefore, we performed the analysis in patients with a
relative dose of TKI/BSA of ≥70 and in those with a relative dose
of TKI/BSA of <70 %/m2. There were no statistically
significant differences in PFS and OS between the two groups of
patients (Table III).
| Table III.Relative dose of TKI/BSA and survival
in patients with or without AS treatment. |
Table III.
Relative dose of TKI/BSA and survival
in patients with or without AS treatment.
|
| Survival |
|
|---|
|
|
|
|
|---|
| Relative dose of
TKIa/BSA | With AS | Without AS | P-value |
|---|
| ≥70
(%/m2) |
|
|
|
| Number of
patients | 5 | 17 |
|
| PFS,
months (range) | 24 (1-NA) | 18 (2-NA) | 0.959 |
| OS,
months (range) | 44 (1-NA) | 34 (17-NA) | 0.342 |
| <70
(%/m2) |
|
|
|
| Number of
patients | 6 | 18 |
|
| PFS,
months (range) | 6 (1-NA) | 13 (2–29) | 0.959 |
| OS,
months (range) | 4 (1-NA) | 22 (11-NA) | 0.361 |
Discussion
In the present study, we evaluated whether oral AS
therapy is truly associated with decreased efficacy of gefitinib
and erlotinib, particularly in patients with mutated EGFR. Our
results demonstrated that oral AS therapy is not associated with
decreased efficacy of gefitinib and erlotinib in patients with
mutated EGFR, which was inconsistent (5) or consistent (6) with previous studies. Chu et al
(5) reported that gastric acid
suppression was associated with decreased erlotinib efficacy in
NSCLC patients. That retrospective study included 507 patients with
advanced NSCLC, but there were 487 patients with unknown EGFR
mutation status. By contrast, Hilton et al (6) reported that the co-administration of AS
treatment with erlotinib did not appear to exert a significant
effect on the median plasma drug levels or the outcome. The study
evaluated pharmacokinetics and survival in the patients of a phase
III clinical trial (BR.21), but there was no information regarding
the association among AS treatment, EGFR mutation status and
patient survival (6). Although it is
clear that AS administration may affect the absorption of erlotinib
in an experimental setting, it is uncertain whether the decreased
erlotinib efficacy associated with AS in the study by Chu et
al (5) can be generalized when AS
agents are prescribed for oral use, or when other TKIs, such as
gefitinib, are prescribed in patients with mutated EGFR. This
inconsistence in the results may be attributed to a number of
possible reasons, such as the difference in EGFR mutation status,
difference in BSA of the patients, difference in the AS agent
prescribed, and different ethnicities. All our patients had mutated
EGFR, the median BSA of the patients was 1.41–1.42 m2,
all the patients had received oral AS treatment, and all our
patients were Asians and Caucasians similar to the study by Chu
et al (5).
It is well known that the association between the
maximum tolerated dose (MTD) and recommended dose (RD) in erlotinib
and gefitinib treatment may be associated with this inconsistency.
The RD of gefitinib (250 mg/day) for NSCLC is only one-third of its
MTD, whereas the RD used for erlotinib (150 mg/day) is its MTD
(11,12). Cigarette smoking is a well-known
factor that may alter erlotinib plasma levels (13). In our study, there was no difference
in smoking status between patients with and those without AS
treatment. In addition, no patients were smoking during the TKI
administration. Another explanation for the inconsistency may be
that it reflects the presence of comorbidities where AS use was
indicated, such as aspirin for cardiovascular disease,
dexamethasone for symptomatic NSCLC, gastroesophageal reflux or
treatment for duodenal or gastric ulcers. Taking this evidence into
consideration, we hypothesized that, in patients with mutated EGFR,
decreased AUC by AS therapy may exert a relatively smaller effect
on TKI efficacy compared with that in patients with wild-type EGFR,
i.e., prevalence of an EGFR mutation may allow a significantly
lower than standard TKI dose to be effective, thereby circumventing
the reduced TKI absorption caused by AS therapy, as suggested by
Yeo et al in a study on erlotinib therapy (14).
The main limitation of our study is due to its
retrospective design and the small sample size. In addition, there
were no data on pharmacokinetics and its effect on treatment
efficacy. In addition, no data are available on whether AS
treatment decreases TKI serum levels in Japanese patients. If so,
it is not known whether the serum level is decreased below what
would be clinically efficient. However, despite these limitations,
the difference in our outcomes compared with those of previous
studies on erlotinib therapy may be of clinical value when
administering TKIs and AS therapy in NSCLC patients with mutated
EGFR.
In conclusion, our study suggests that AS treatment
may not compromise TKI efficacy in patients with mutated EGFR.
Prospective studies and large-scale confirmation studies
investigating the effect of AS and TKI co-administration in NSCLC
patients with mutated EGFR may be meaningful in clinical
practice.
References
|
1
|
Achem SR and DeVault KR: Gastroesophageal
reflux disease and the elderly. Gastroenterol Clin North Am.
43:147–160. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Keynes WM: Medical response to mental
stress. J R Soc Med. 87:536–539. 1994.PubMed/NCBI
|
|
3
|
US Food and Drug Administration: Center
for Drug Evaluation and Research. Tarceva NDA 21–743/S000 clinical
pharmacology and biopharmaceutics review. November
18–2004.http://www.accessdata.fda.gov/drugsatfda_docs/nda/2004/21-743_Tarceva_biopharmr.PDFAccessed.
May 01–2014
|
|
4
|
Budha NR, Frymoyer A, Smelick GS, Jin JY,
Yago MR, Dresser MJ, Holden SN, Benet LZ and Ware JA: Drug
absorption interactions between oral targeted anticancer agents and
PPIs: Is pH-dependent solubility the Achilles heel of targeted
therapy? Clin Pharmacol Ther. 92:203–213. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chu MP, Ghosh S, Chambers CR, Basappa N,
Butts CA, Chu Q, Fenton D, Joy AA, Sangha R, Smylie M and Sawyer
MB: Gastric acid suppression is associated with decreased erlotinib
efficacy in non-small-cell lung cancer. Clin Lung Cancer. 16:33–39.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hilton JF, Tu D, Seymour L, Shepherd FA
and Bradbury PA: An evaluation of the possible interaction of
gastric acid suppressing medication and the EGFR tyrosine kinase
inhibitor erlotinib. Lung Cancer. 82:136–142. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ter Heine R, Fanggiday JC, Lankheet NA,
Beijnen JH, Van Der Westerlaken MM, Staaks GH and Malingré MM:
Erlotinib and pantoprazole: A relevant interaction or not? Br J
Clin Pharmacol. 70:908–911. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Travis WD, Brambilla E, Muller-Hermelink
HK and Harris CC: Pathology and genetics: Tumours of the Lung,
Pleura, Thymus and Heart. IARC Press. Lyon: 9–122. 2004.
|
|
9
|
Vallières E, Shepherd FA, Crowley J, et
al: International Association for the Study of Lung Cancer
International Staging Committee and Participating Institutions: The
IASLC Lung Cancer Staging Project: Proposals regarding the
relevance of TNM in the pathologic staging of small cell lung
cancer in the forthcoming (seventh) edition of the TNM
classification for lung cancer. J Thorac Oncol. 4:1049–1059. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Costa DB, Nguyen KS, Cho BC, Sequist LV,
Jackman DM, Riely GJ, Yeap BY, Halmos B, Kim JH, Jänne PA, et al:
Effects of erlotinib in EGFR mutated non-small cell lung cancers
with resistance to gefitinib. Clin Cancer Res. 14:7060–7077. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rukazenkov Y, Speake G, Marshall G,
Anderton J, Davies BR, Wilkinson RW, Hickinson Mark D and Swaisland
A: Epidermal growth factor receptor tyrosine kinase inhibitors:
Similar but different? Anticancer Drugs. 20:856–866. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
O'Malley M, King AN, Conte M, Ellingrod VL
and Ramnath N: Effects of cigarette smoking on metabolism and
effectiveness of systemic therapy for lung cancer. J Thorac Oncol.
9:917–926. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yeo WL, Riely GJ, Yeap BY, Lau MW, Warner
JL, Bodio K, Huberman MS, Kris MG, Tenen DG, Pao W, et al:
Erlotinib at a dose of 25 mg daily for non-small-cell lung cancers
with EGFR mutations. J Thorac Oncol. 5:1048–1053. 2010. View Article : Google Scholar : PubMed/NCBI
|