Introduction
Hepatocellular carcinoma (HCC) is the fifth most
common cancer worldwide, which is a serious risk to human health
(1,2).
However, the pathogenesis of HCC has not been fully elucidated.
Hepatitis B virus (HBV) chronic infection is considered one of the
major risk factors for the development of HCC (3–5).
The HBV genome is an incomplete double-stranded
circular structure, containing 4 open reading frames (ORF): S, C, P
and X (6,7). ORF region mutations could alter viral
replication and virulence force, which lead to a persistent virus
infection and severe liver cell damage, and eventually result in
the development of HCC (8,9). The precore region encodes the hepatitis
B e-antigen (HBeAg), which has been associated with an increased
risk of HCC statistically. Certain studies have shown that HBV X
gene point mutations can affect the expression of HBeAg and
increase the viral replication capacity (8,10,11). In recent years, the association
between HBV mutations and the incidence of HCC has focused on the X
gene region, the former C gene region and pre-S gene region, and
the X gene region is the most important.
Previously, certain studies have identified that the
X gene region T1653, V1753, T1762/A1764 and other point mutations
may be associated with persistent HBV infection and the development
of HCC (6,10–13).
However, there remains certain controversy and further research is
required. Therefore, the present meta-analysis was performed to
investigate the association between HBV X gene point mutations and
the development of HCC systematically and comprehensively.
Materials and methods
Search strategy
Two authors (Wang and Zeng) searched PubMed, EMBASE,
the Cochrane Library and Chinese National Knowledge Infrastructure
for the relevant studies. The key words included: ‘Hepatitis B
virus X gene’, ‘mutation’, ‘liver cancer or hepatocellular
carcinoma’. The searches were limited to human subjects. Language
restriction was not imposed on the search process. In addition, the
reference lists of the included studies were checked manually for
other potentially eligible studies. This process was repeated until
no additional associated studies could be identified.
Inclusion criteria
The inclusion criteria included: i) Study design for
the prevalence of case-control; ii) the diagnoses of chronic
hepatitis B, liver cirrhosis and HCC were according to the
guidelines of the American Association for the Study of Liver
Diseases (14); iii) all
HBsAg-positive patients were infected with HBV >2 years and the
HBV DNA level was in accordance with the test standard; and iv) the
reported outcomes of patients was HCC.
Exclusion criteria
The exclusion criteria included: i) Patients with
HCV, HDV or human immunodeficiency virus infection; ii) patients
with alcoholic liver disease, autoimmune disease or drug-induced
liver disease; iii) patients with antiviral treatment; iv) if
similar research was reported by the same author, only the recent
study or high-quality study was included in this analysis.
Data extraction and quality
evaluation
Data extraction and quality evaluation of studies
were conducted by 2 independent authors (Wang and Chen). The
extracted data included first author, publication year, country,
study design, quality score, cases of patients (number of events
and total patients), age, gender, alanine aminotransferase and HBV
DNA level, genotypes, mutation sites and detection method. The
evaluation standard was in accordance with the methods of the study
by Liu et al (15). Discussion
or a third investigator aided in solving any disagreements.
Statistical analysis
The odds ratios (ORs) with 95% confidence intervals
(CIs) of binary end points were analyzed. Heterogeneity was checked
using χ2 test, P-values and I2. The random
effects model was used when P<0.1; otherwise the fixed effects
model was used when P≥0.1. Sensitivity analysis was conducted by
eliminating one study in turn in the analysis. Potential
publication bias was evaluated by visual inspection of the Begg
funnel plots in which the log ORs were plotted against their
standard errors. All the data were calculated by RevMan 5.0
software (Copenhagen: The Nordic Cochrane Centre, The Cochrane
Collaboration).
Results
Study characteristics
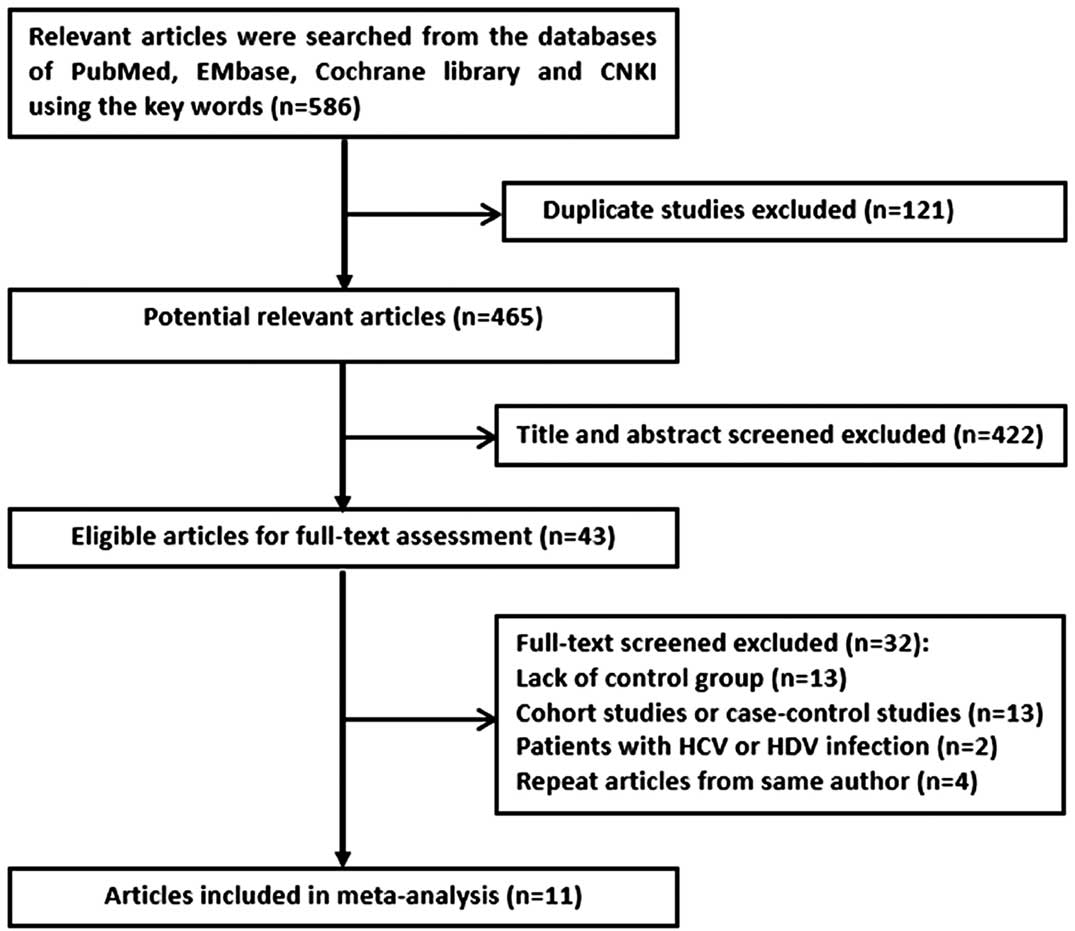
According to the inclusion and exclusion criteria of
the literature, 11 studies involving 2,502 patients were included
in this meta-analysis, of whom 2,801 had HCC. These studies
included 1 study in Chinese and 10 in English (6,11,13,16–23). A
detailed flow chart explaining the inclusion of studies is shown in
Fig. 1. The extracted information
from the studies included: i) The publication year of the studies
was between 1999 and 2013; ii) the study design were case-control
studies; iii) the countries of the studies included mainland China,
Hong Kong, South Korea and Thailand. A summary of the 11 included
studies is shown in Table I. The
details of the quality criteria based on factors are listed in
Table II.
 | Table I.Characteristics and clinical data of
the studies included in the meta-analysis. |
Table I.
Characteristics and clinical data of
the studies included in the meta-analysis.
| Authors (year) | Country | Design | Quality score | E/C | Age, years | Gender (m/f) | ALT level (U/l) | HBV DNA (log
copy/ml) | HBeAg (+) patients
(%) | Genotype | Mutation sites | Detection method | Refs. |
|---|
| Takahashi et
al (1999) | Japan | PCC | 6–10 |
58/271 | NA | NA | NA | NA | 108
(37.6) | C | T1653, V1753, T1762,
A1764, T1762/A1764 | Sequencing | (16) |
| Tanaka et al
(2006) | Japan/HK | PCC | ≥10 | 148/180 | 50.2±10.7 | 261/69 | 46 (8–773) | 5.4±1.4 | 109
(33.2) | C1, C2 | T1653, V1753,
T1762/A1764, V1765, A1896, A1899 | Sequencing | (17) |
| Shinkai et al
(2007) | Japan | PCC | ≥10 | 80/80 | 55±8 | 135/25 |
85±133 | 5.7±1.4 | 60
(37.5) | C2 | T1653, C1479, T1485,
H1499, A1613, V1753, T1762/A1764, A1896 | Sequencing | (13) |
| Wang et al
(2007) | China | PCC | ≤6 |
47/164 | 49.8±11.6 | 176/35 | 63.9±41.6 | NA | 112
(53.1) | Ba, C1, C2 | T1653, V1753,
T1762/A1764, T1856, T1858, A1896, A1898, A1899 | Sequencing | (18) |
| Kim et al
(2008) | Korea | PCC | 6–10 |
60/124 | 45.9±17.3 | 134/50 |
90.8±132.1 | NA | 115
(62.5) | C | T1653, V1753,
T1762/A1764 | Sequencing | (19) |
| Kim et al
(2009) | Korea | PCC | ≥10 | 135/135 | 44.3±7.9 | 224/46 | NA | 3.45±3.8 | 76
(28.1) | C2 | T1653, A1689,
V1753, T1762/A1764, T1846, A1850, C1858, A1896 | Sequencing |
(6) |
| Choi et al
(2009) | Korea | PCC | ≤6 | 42/46 | 57.3±9.3 | 57/31 |
89.8±110.5 | 6.2±1.5 | 39
(44.3) | C2 | M1385, A1485,
B1499, B1574, A1613, T1631, T1653, V1753, T1762/A1764 | Sequencing | (20) |
| Tangkijvanich et
al (2010) | Thailand | PCC | ≥10 | 60/60 | 55.7±9.8 | 104/16 | 161.1±116.9 | 5.9±1.4 | 32 (30) | B, C | A1613, T1653,
V1753, T1762/A1764, T1766/A1768, C1858C | Sequencing | (21) |
| Shi et al
(2013) | China | PCC | ≤6 | 43/55 | 58.0±9.58 | 63/32 | NA | 4.67±0.91 | 46
(47.9) | NA | A1440, C1467,
A1479, T1485, T1653, V1753, T1762/A1764 | Sequencing | (11) |
| Li et al
(2013) | China | PCC | 6–10 | 102/105 | NA | NA | NA | NA | NA | C2 | T1653, V1753,
T1762, A1764, T1766, A1768 | Sequencing | (22) |
| Lyu et al
(2013) | Korea | PCC | 6–10 | 318/234 | 55 (30–74) | 452/100 | 37 (9–774) | 4.09±2.39 | 271
(49.1) | C2 | T1653, V1753,
T1762/A1764, A1896 | Sequencing | (23) |
| Table II.Details of the quality criteria for
studies included in the meta-analysis. |
Table II.
Details of the quality criteria for
studies included in the meta-analysis.
|
| Score |
|---|
|
|
|
|---|
| Quality
parameter | 0 | 1 | 2 |
|---|
| Study design | Cohort or nested
case-control | Incidence
case-control | Prevalence
case-control |
| Sample size of
cases | <50 | 50–100 | ≥100 |
| Source of
samples | None | 1 hospital | ≥2 hospitals |
| Mutation detection
method | None | Others | DNA sequencing |
| Matching of cases
and controls |
|
|
|
|
(1) | None | Age or gender | Age and gender |
|
(2) | None | HBeAg or
genotype | HBeAg and
genotype |
Meta-analysis
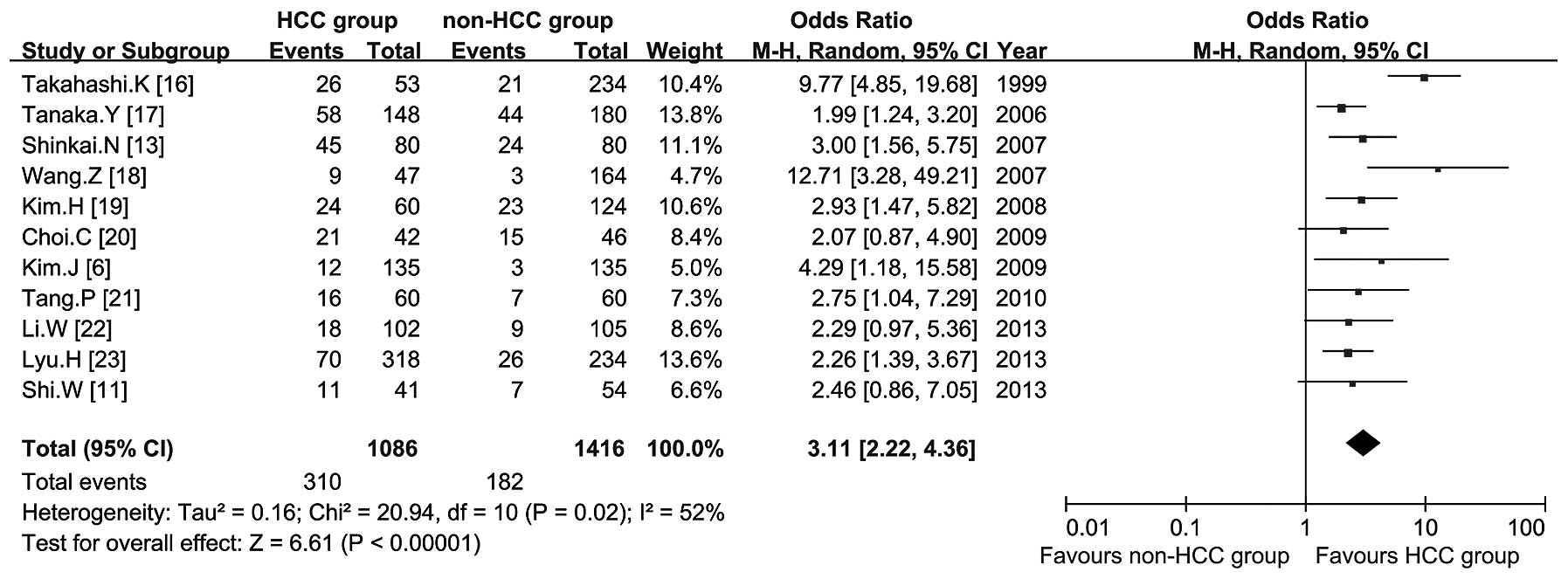
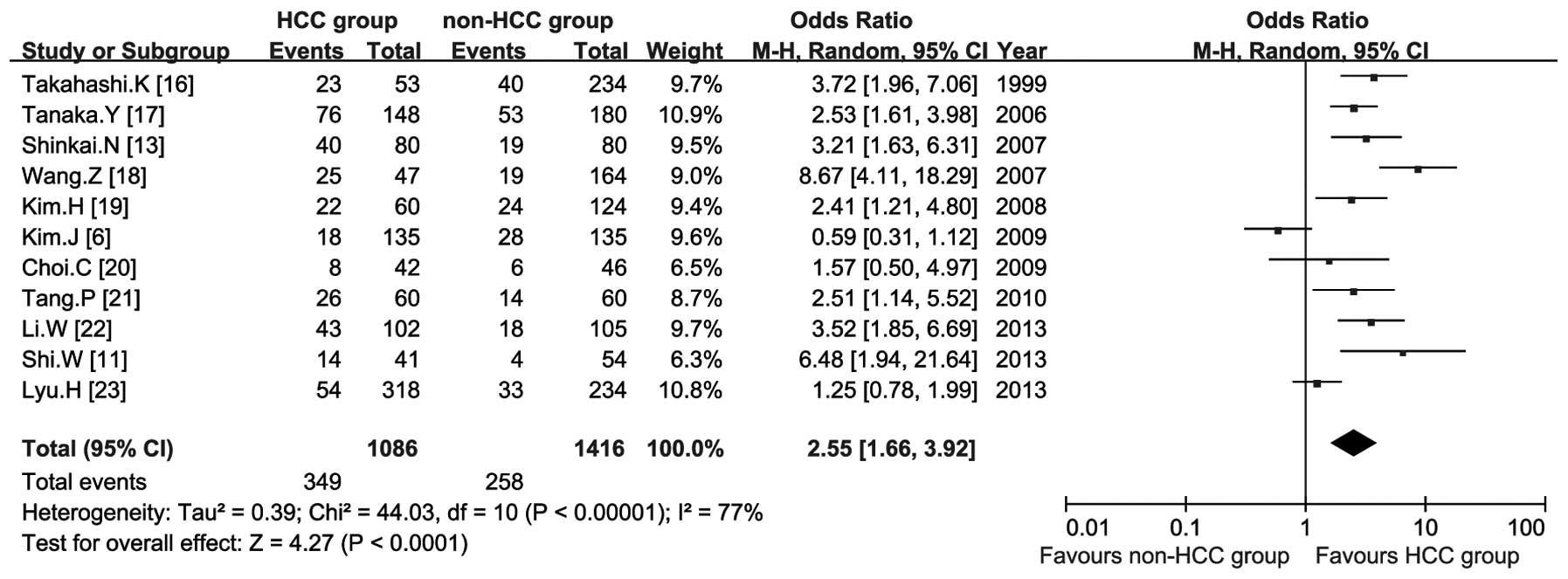
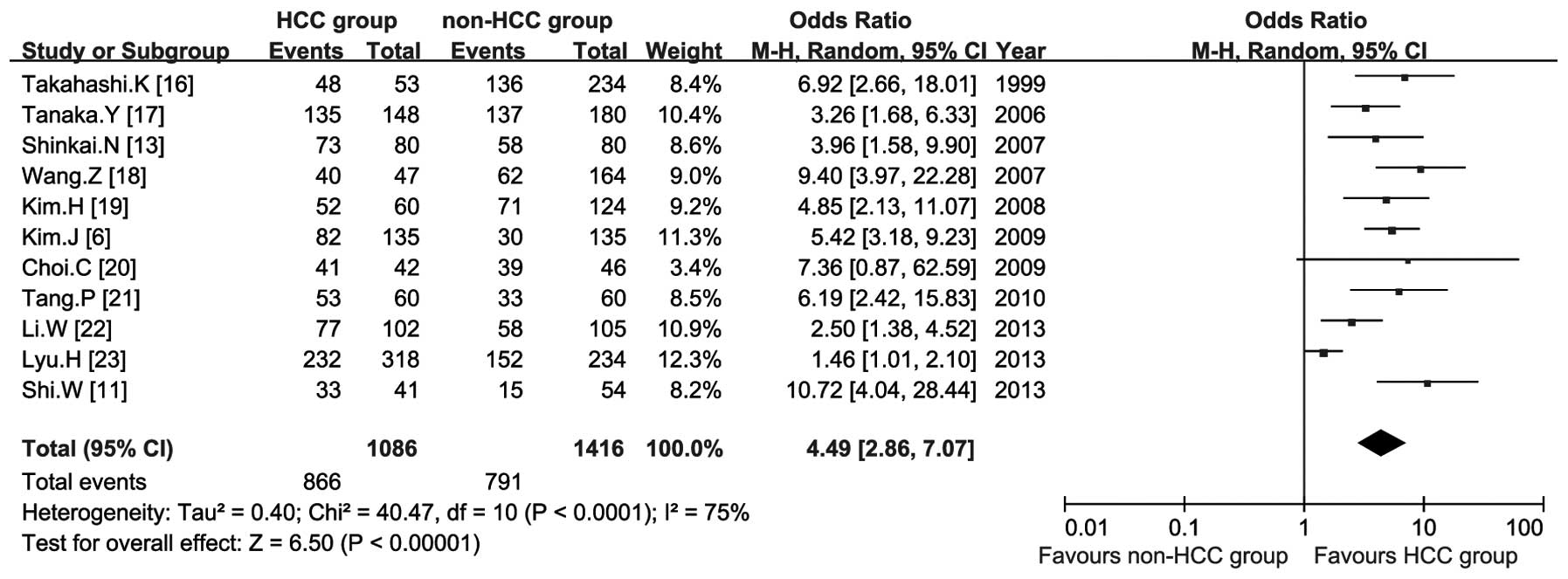
All 11 studies involving 2,502 patients reported
that the relevant outcome of the T1653, V1753 and T1762/A1764 point
mutations were associated with the risk of HCC. The results of the
meta-analysis showed that T1653 (OR, 3.11; 95% CI, 2.22–4.36)
(Fig. 2), V1753 (OR, 2.55; 95% CI,
1.66–3.92) (Fig. 3) and T1762/A1764
(OR, 4.49; 95% CI, 2.86–7.07) (Fig.
4) increase the risk of HCC.
Subgroup analysis
The summary ORs for HBV X gene mutations were
explored by HBeAg status, country and quality score. The summary OR
of the T1762/A1764 double mutations in HBeAg (+) group were lower
compared to the HBeAg (−) group, whereas the T1653 and V1753
mutations were higher. There is no significant difference in the
results between subgroup and overall analyses except for the V1753
point mutation for the risk of HCC in patients from Korea. The
result suggested that there was no statistically significant
associations between the V1753 mutation and the risk of HCC in
Korean patients (OR, 1.25; 95% CI, 0.69–2.26) (Table III). The summary ORs for T1653,
V1753 and T1762/A1764 increased with decreasing study quality score
(Table III).
| Table III.Subgroup analyses based on the main
characteristics of the included studies. |
Table III.
Subgroup analyses based on the main
characteristics of the included studies.
|
| T1653 | V1753 | T1762/A1764 |
|---|
|
|
|
|
|
|---|
|
Characteristics | T/P | OR (95% CI) | Model | T/P | OR (95% CI) | Model | T/P | OR (95% CI) | Model |
|---|
| HBeAg |
|
| + | 5/392 | 3.25
(1.87–5.66) | Fixed | 5/392 | 2.50
(1.52–4.12) | Fixed | 6/536 | 3.15
(2.03–4.89) | Fixed |
| − | 5/741 | 2.56
(1.78–3.68) | Fixed | 5/741 | 1.84
(1.32–2.58) | Fixed | 6/911 | 5.50
(2.64–11.46) | Fixed |
| Country |
|
|
China | 3/513 | 3.23
(1.80–5.79) | Fixed | 3/513 | 5.17
(3.28–8.13) | Fixed | 3/513 | 5.99
(2.17–16.53) | Random |
|
Japan | 3/775 | 3.78
(1.52–9.41) | Random | 3/775 | 2.93
(2.11–4.06) | Fixed | 3/775 | 4.27
(2.68–6.80) | Fixed |
|
Korea | 4/1,094 | 2.50
(1.77–3.54) | Fixed | 4/1,094 | 1.25
(0.69–2.26) | Random | 4/1,094 | 3.58
(1.46–8.79) | Random |
|
Thailand | 1/120 | 2.75
(1.04–7.29) | NA | 1/120 | 2.51
(1.14–5.52) | NA | 1/120 | 6.19
(2.42–15.83) | NA |
| Quality score |
|
|
>6 | 8/2,108 | 3.05
(2.10–4.42) | Random | 8/2,108 | 2.14
(1.39–3.28) | Random | 8/2,108 | 3.66
(2.30–5.81) | Random |
| ≤6 | 3/394 | 3.11
(1.74–5.59) | Fixed | 3/394 | 5.18
(2.98–9.02) | Fixed | 3/394 | 9.60
(5.14–17.93) | Fixed |
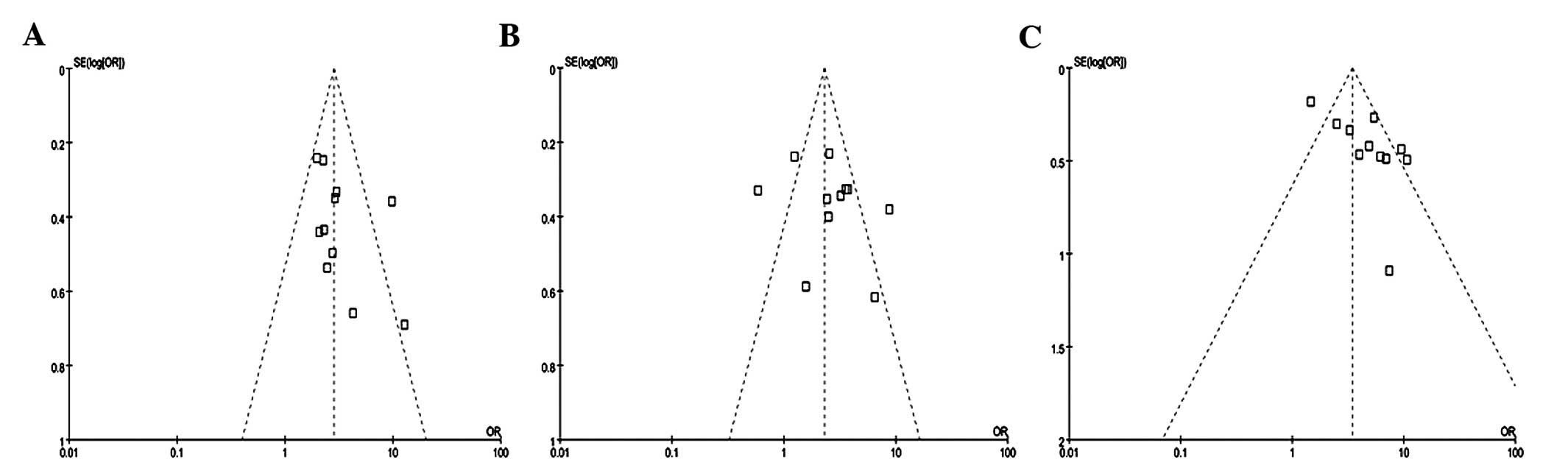
Sensitivity analysis and publication
bias
The effect of a single study on the overall pooled
analyses was investigated by sensitivity analysis to evaluate the
heterogeneity of each study. There were no significant influences
observed when one study was removed each turn. The funnel plot
showed an asymmetrical distribution of these studies, indicating
that publication bias existed in these results regarding an
association between T1653 (Fig. 5A),
V1753 (Fig. 5B) and T1762/A1764
(Fig. 5C) point mutations and the
risk of HCC.
Discussion
Meta-analysis is regarded as a qualitative and
quantitative tool to solve those problems that remain controversial
in clinical settings. The results of the meta-analysis were the
highest level of evidence. The debate on the association between
HBV gene mutations and development of HCC is ongoing. Recently, a
series of studies on this subject have been published. Therefore,
the present meta-analysis was performed and the results showed that
T1653, V1753 and T1762/A1764 mutations could significantly increase
the risk of HCC, particularly the T1762/A1764 double mutations.
HBV chronic infection is the most important risk
factor for the development of HCC (24). Lin et al (25) considered that the transactivation
function of the carboxyl terminus of the HBV X protein would
regulate HBV DNA replication and transcription of liver cell
proliferation and differentiation. As well as T1653, V1753 and
T1762/A1764 mutations are all located in the carboxyl terminus
region of the HBV X protein. Kim et al (19) suggested that T1653, V1753 and
T1762/A1764 mutations would change the sequence of HBV X protein
amino acids, further leading to the activation of proto-oncogenes
and inactivation of the tumor suppressor gene, eventually causing
the occurrence of HBV-related HCC. However, the mechanism of how
the point mutations of HBV X gene region affect the biological
function of HBV X protein remains to be elucidated in further
studies.
Liu et al (15)
considered that the HBeAg status would affect the point mutation
type of the HBV X gene and development of HCC. Previous studies
suggested that the expression of HBeAg is often significantly
correlated with immune evasion and acted as an indicator of active
viral replication (26,27). In the subgroup analysis, data on the
HBeAg status was extracted, which was a potential confounder, and
identified that T1762/A1764 double mutations could decrease HBeAg
expression. However, a large number of studies showed that
T1762/A1764 double mutations could enhance the virus replication.
The contradiction indicated that the decrease of HBeAg expression
did not equate to an improved development of HCC. Persistent
chronic HBV infection may be due to HBV immune escape, which
further aggravates the condition of patients and eventually results
in HCC (28,29). Li et al (22) reported that T1762/A1764 double
mutations could not predict the development of HCC. However, the
present study identified that double mutations were more closely
associated with the risk of HCC compared to T1653 or V1753 alone.
Therefore, the combined mutations could lead to a higher incidence
of liver cancer and improve the predictability of HCC.
The present findings showed that the summary ORs for
T1653, V1753 and T1762/A1764 were higher in the low-quality
compared to the high-quality studies. Potential confounders may
have an important role in evaluating HBV mutations and the risk of
HCC in low-quality studies. Yin et al (30) suggested that the average age of the
patients with chronic hepatitis B was 10 years younger than that of
the patients with HCC. Additionally, Yang et al (31) suggested that HBV mutations accumulated
with increasing age. Therefore, the association between the HBV X
gene point mutations and risk of HCC was more likely to be
overestimated in the confounder-unmatched, low-quality studies.
The main characteristics embodied in the present
study were: i) The association between HBV X gene mutations and
development of HCC among various studies examined systematically
and comprehensively, in order to have an improved understanding for
the effect of HBV X protein on development of HCC; ii) a series of
subgroup analyses were conducted to explore the effect of potential
confounding factors on the development of HCC; and iii) the results
suggested that these point mutations could be used as molecular
markers of the risk of HCC. The limitations of the study were: i)
The age, gender, genotype and other confounding factors could not
be matched fully and the existence of various offsets requires
further information and data to be confirmed; ii) only 3 HBV X gene
mutations were analyzed in the meta-analysis, and there may be
other gene mutations that affect the HBV X protein biological
function as well as V1674, T1766 and A1768 mutations; and iii) the
included studies were all observational case-control studies, as
experimental studies could not be conducted in humans.
In the future, the mechanism of the HBV X gene
region point mutations should focus on the biological function of
the HBV X protein and the association with the development of HCC.
In order to improve the prediction for HCC risk and reduce or even
avoid the development of HCC, quicker and easier methods should be
developed for the detection of HBV gene mutations.
Acknowledgements
The authors would like to thank Dr Longkun Li for
providing methods of data analysis.
References
|
1
|
Cazzagon N, Trevisani F, Maddalo G, et al:
Italian Liver Cancer (ITA.LI.CA) Group: Rise and fall of
HCV-related hepatocellular carcinoma in Italy: A long-term survey
from the ITA.LI.CA centres. Liver Int. 33:1420–1427. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fares N and Peron JM: Epidemiology,
natural history, and risk factors of hepatocellular carcinoma. Rev
Prat. 63:216–217, 220–212. 2013.(In French). PubMed/NCBI
|
|
3
|
Matsuda Y and Ichida T: Impact of
hepatitis B virus X protein on the DNA damage response during
hepatocarcinogenesis. Med Mol Morphol. 42:138–142. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rawat S, Clippinger AJ and Bouchard MJ:
Modulation of apoptotic signaling by the hepatitis B virus X
protein. Viruses. 4:2945–2972. 2012. View
Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bouchard MJ and Navas-Martin S: Hepatitis
B and C virus hepatocarcinogenesis: Lessons learned and future
challenges. Cancer Lett. 305:123–143. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kim JK, Chang HY, Lee JM, Baatarkhuu O,
Yoon YJ, Park JY, Kim Y, Han KH, Chon CY and Ahn SH: Specific
mutations in the enhancer II/core promoter/precore regions of
hepatitis B virus subgenotype C2 in Korean patients with
hepatocellular carcinoma. J Med Virol. 81:1002–1008. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Liu L, Li Y, Zhang S, Yu D and Zhu M:
Hepatitis B virus X protein mutant upregulates CENP-A expression in
hepatoma cells. Oncol Rep. 27:168–173. 2012.PubMed/NCBI
|
|
8
|
Tu H, Bonura C, Giannini C, Mouly H,
Soussan P, Kew M, Paterlini-Bréchot P, Bréchot C and Kremsdorf D:
Biological impact of natural COOH-terminal deletions of hepatitis B
virus X protein in hepatocellular carcinoma tissues. Cancer Res.
61:7803–7810. 2001.PubMed/NCBI
|
|
9
|
Yeh CT, Shen CH, Tai DI, Chu CM and Liaw
YF: Identification and characterization of a prevalent hepatitis B
virus X protein mutant in Taiwanese patients with hepatocellular
carcinoma. Oncogene. 19:5213–5220. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kaneko M, Uchida T, Moriyama M, Arakawa Y,
Shikata T, Gotoh K and Mima S: Probable implication of mutations of
the X open reading frame in the onset of fulminant hepatitis B. J
Med Virol. 47:204–208. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shi W, Wang Q, Zhao X and Zhao L: Study on
the relationship between the mutations of hepatitis B virus X gene
and precore gene, related factors and hepatocellular carcinoma.
Chinas Med. 8:1673–4777. 2013.(In Chinese).
|
|
12
|
Uchida T, Saitoh T and Shinzawa H:
Mutations of the X region of hepatitis B virus and their clinical
implications. Pathol Int. 47:183–193. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Shinkai N, Tanaka Y, Ito K, Mukaide M,
Hasegawa I, Asahina Y, Izumi N, Yatsuhashi H, Orito E, Joh T, et
al: Influence of hepatitis B virus X and core promoter mutations on
hepatocellular carcinoma among patients infected with subgenotype
C2. J Clin Microbiol. 45:3191–3197. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cabibbo G, Antonucci M and Genco C: Update
on new approaches in the management of hepatocellular carcinoma.
Hepat Med. 2:163–173. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Liu S, Zhang H, Gu C, Yin J, He Y, Xie J
and Cao G: Associations between hepatitis B virus mutations and the
risk of hepatocellular carcinoma: A meta-analysis. J Natl Cancer
Inst. 101:1066–1082. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Takahashi K, Ohta Y, Kanai K, Akahane Y,
Iwasa Y, Hino K, Ohno N, Yoshizawa H and Mishiro S: Clinical
implications of mutations C-to-T1653 and T-to-C/A/G1753 of
hepatitis B virus genotype C genome in chronic liver disease. Arch
Virol. 144:1299–1308. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tanaka Y, Mukaide M, Orito E, Yuen MF, Ito
K, Kurbanov F, Sugauchi F, Asahina Y, Izumi N, Kato M, et al:
Specific mutations in enhancer II/core promoter of hepatitis B
virus subgenotypes C1/C2 increase the risk of hepatocellular
carcinoma. J Hepatol. 45:646–653. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang Z, Tanaka Y, Huang Y, Kurbanov F,
Chen J, Zeng G, Zhou B, Mizokami M and Hou J: Clinical and
virological characteristics of hepatitis B virus subgenotypes Ba,
C1 and C2 in China. J Clin Microbiol. 45:1491–1496. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kim HJ, Park JH, Jee Y, Lee SA, Kim H,
Song BC, Yang S, Lee M, Yoon JH, Kim YJ, et al: Hepatitis B virus X
mutations occurring naturally associated with clinical severity of
liver disease among Korean patients with chronic genotype C
infection. J Med Virol. 80:1337–1343. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Choi CS, Cho EY, Park R, Kim SJ, Cho JH
and Kim HC: X gene mutations in hepatitis B patients with
cirrhosis, with and without hepatocellular carcinoma. J Med Virol.
81:1721–1725. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tangkijvanich P, Sa-Nguanmoo P, Mahachai
V, Theamboonlers A and Poovorawan Y: A case-control study on
sequence variations in the enhancer II/core promoter/precore and X
genes of hepatitis B virus in patients with hepatocellular
carcinoma. Hepatol Int. 4:577–584. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Li W, Chen G, Yu X, Shi Y, Peng M and Wei
J: Accumulation of the mutations in basal core promoter of
hepatitis B virus subgenotype C1 increase the risk of
hepatocellular carcinoma in Southern China. Int J Clin Exp Pathol.
6:1076–1085. 2013.PubMed/NCBI
|
|
23
|
Lyu H, Lee D, Chung YH, Kim JA, Lee JH,
Jin YJ, Park W, Mathews P, Jaffee E, Zheng L, et al: Synergistic
effects of A1896, T1653 and T1762/A1764 mutations in genotype c2
hepatitis B virus on development of hepatocellular carcinoma. J
Viral Hepat. 20:219–224. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Huang X and Hollinger FB: Occult hepatitis
B virus infection and hepatocellular carcinoma: A systematic
review. J Viral Hepat. 21:153–162. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lin CL, Chen JD, Liu CJ, Lee PH, Chen PJ,
Lai MY, Kao JH and Chen DS: Clinicopathological differences between
hepatitis B viral genotype B- and C-related resectable
hepatocellular carcinoma. J Viral Hepat. 14:64–69. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kay A and Zoulim F: Hepatitis B virus
genetic variability and evolution. Virus Res. 127:164–176. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yim HJ and Lok AS: Natural history of
chronic hepatitis B virus infection: What we knew in 1981 and what
we know in 2005. Hepatology. 43(Suppl 1): S173–S181. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Jammeh S, Tavner F, Watson R, Thomas HC
and Karayiannis P: Effect of basal core promoter and pre-core
mutations on hepatitis B virus replication. J Gen Virol.
89:901–909. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Buckwold VE, Xu Z, Chen M, Yen TS and Ou
JH: Effects of a naturally occurring mutation in the hepatitis B
virus basal core promoter on precore gene expression and viral
replication. J Virol. 70:5845–5851. 1996.PubMed/NCBI
|
|
30
|
Yin J, Zhang H, Li C, Gao C, He Y, Zhai Y,
Zhang P, Xu L, Tan X, Chen J, et al: Role of hepatitis B virus
genotype mixture, subgenotypes C2 and B2 on hepatocellular
carcinoma: Compared with chronic hepatitis B and asymptomatic
carrier state in the same area. Carcinogenesis. 29:1685–1691. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Yang HI, Yeh SH, Chen PJ, Iloeje UH, Jen
CL, Su J, Wang LY, Lu SN, You SL, Chen DS, et al: REVEAL-HBV Study
Group: Associations between hepatitis B virus genotype and mutants
and the risk of hepatocellular carcinoma. J Natl Cancer Inst.
100:1134–1143. 2008. View Article : Google Scholar : PubMed/NCBI
|