Introduction
Ovarian thecoma is a rare benign tumor of stromal
cell origin, and represents <1% of all ovarian tumors (1). It occurs most often in perimenopausal
and postmenopausal women. Elevated serum cancer antigen (CA)125
levels in postmenopausal women with solid adnexal masses, ascites
and pleural effusion are highly suggestive for malignant ovarian
tumors. However, surgery and histological confirmation of the
preoperative diagnosis are mandatory, since a minority of patients
with these findings have a benign condition, commonly known as
Meigs' syndrome. This condition disappears following the removal of
the pelvic tumor. The present study reported a case of massive
pleural effusions caused by right ovarian thecoma with elevated
serum CA125 levels in a postmenopausal woman. This patient was
clinically interpreted to harbor a malignant ovarian tumor, which
was eventually revealed to be benign ovarian thecoma.
Case report
A 58-year-old, para 2 women visited the Respiratory
Medical Clinic at The First Affiliated Hospital of Xi'an Jiaotong
University (Shaanxi, China) in December 2014 due to a 1-week-long
cough and shortness of breath for 4 days. The patient went through
the menopause at the age of 50. Chest examination revealed dullness
to the percussion and diminished breath sounds on the right lung.
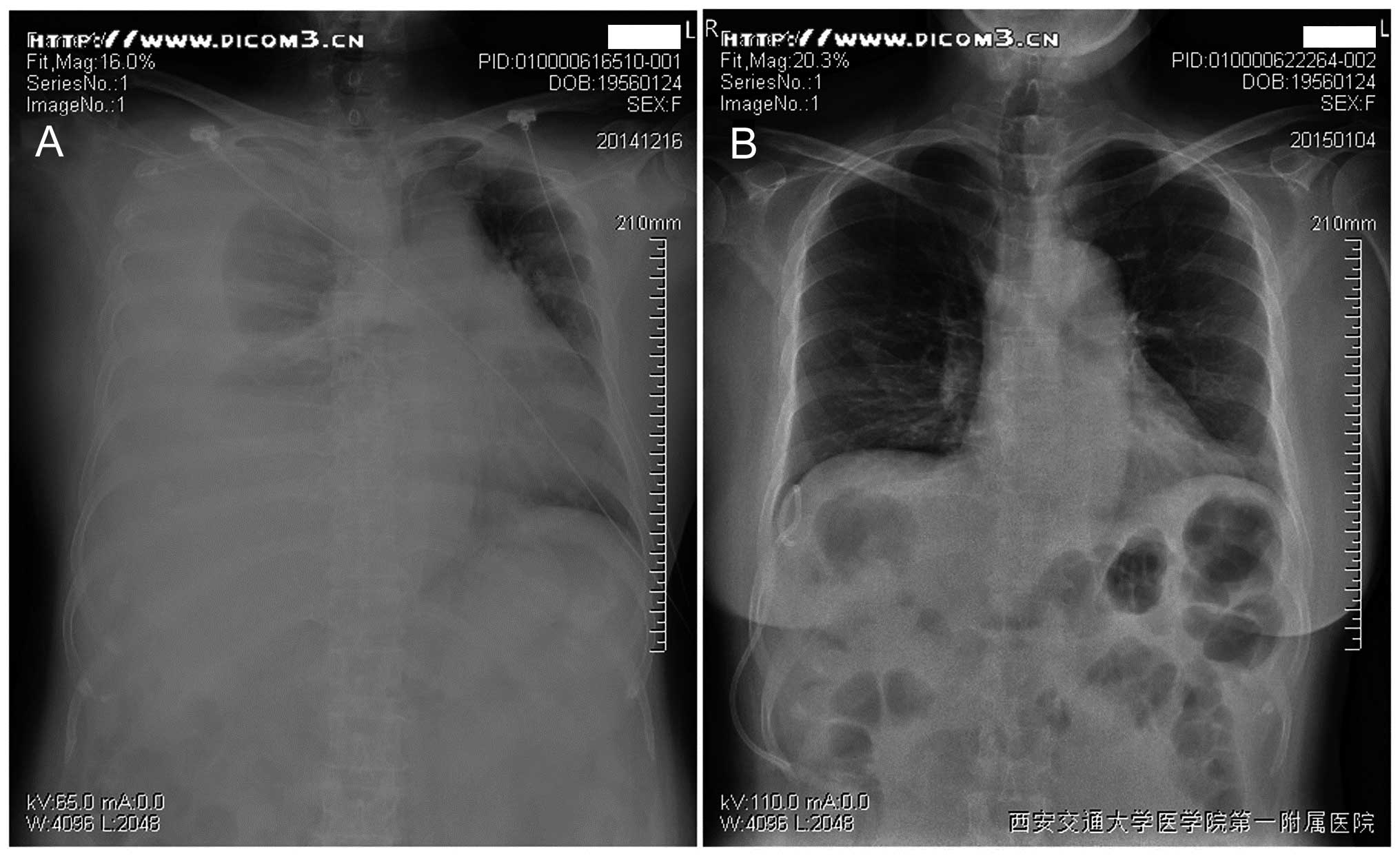
Chest radiography revealed right pleural effusions (Fig. 1A). The patient underwent
thoracentesis, followed by draining of yellowish pleural effusion
(5,000 ml) by closed thoracic drainage. Pleural fluid cytology
revealed no malignant cells. The CA125 tumor marker level was
reported as 577 IU/ml (normal, <35 U/ml), and other studies,
including respiratory virus antibody, Mycobacterium
tuberculosis antibody immunoglobulin G, tuberculosis-DNA,
tuberculosis spot test, endotoxin and fungal glucan, revealed
negative findings. A pelvic ultrasound revealed a hypoechoic mass
measuring 16.5×13.8×13 cm and the uterus endometrium thickness of
0.4 cm, with some pelvic ascites (6.2×2.7 cm). The patient was
finally referred to the Department of Obstetrics and Gynecology,
The First Affiliated Hospital of Xi'an Jiaotong University,
(Shaanxi, China) as a result of this mass. Following the initial
hypothesized diagnosis of an ovarian tumor with ascites and
hydrothorax, an exploratory laparotomy was performed. During the
operation, the left ovary measured 20×15×15 cm and had a smooth
surface with no excrescences or papillary projections. The left
tube was elongated along the course of the distended ovary, The
right ovary was small with no evidence of cysts. The right
fallopian tube was normal and the uterus was normal. No evidence of
ascites or peritoneal deposits were observed, and the surfaces of
the bowel, liver and omentum were normal. No pelvic or para-aortic
nodal enlargement was observed. The patient underwent a right
salpingo-oophorectomy and the frozen section appeared to be
benign.
Upon gross examination, the ovary measured 17×14×6
cm and no surface excrescences or nodules were observed. The cyst
itself was multiloculated and contained clear, watery serous-type
fluid, with a smooth inner wall of gray. The length of fallopian
tube was 2.5 cm, the diameter was 0.5 cm and the oviduct fimbria
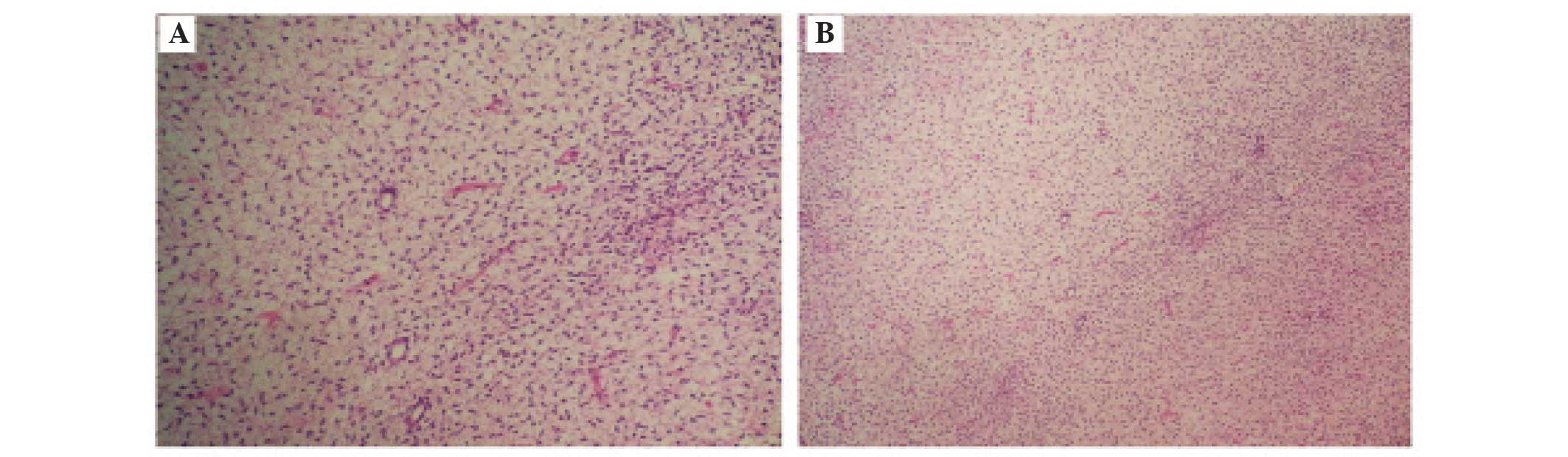
was opening. Microscopic images of the tumor revealed uniform and
cytologically bland-looking spindle cells arranged in fascicles.
Pathological diagnosis was benign ovarian thecoma (Fig. 2). The chest radiograph revealed no
pleural effusion even 6 days after the surgery (Fig. 1B).
Discussion
Thecomas make up only 0.5–1% of ovarian tumor types.
They occur mostly in postmenopausal women, with a mean age of 59
years, and only 10% of the patients are normally <30-years-old.
Thecomas range from small tumors to large solid or solid-cystic
masses of up to 15 cm. They are unilateral in >90% of cases and
are rarely malignant (2,3). Thecomas are stromal tumors made up of
cells that resemble theca cells, lutein cells and fibroblasts
(4). They are traditionally
classified within the sex cord-stromal tumor category of ovarian
tumor types (5).
In the present case, the patient was admitted to the
Respiratory Department at The First Affiliated Hospital of Xi'an
Jiantong University due to breathlessness with no abdominal pain,
bloating and other symptoms. It was revealed that the expression of
CA-125 was increased, and then a reproductive system tumor was
considered. CA125 has been demonstrated to be elevated in benign
conditions, including pelvic inflammatory disease, endometriosis,
uterine leiomyoma and early pregnancy. The serum CA125 levels are
also increased with peritoneal pleural and pericardial inflammation
or irritation. A certain misdiagnosis rate occurs with
Hydroperitonia theca cell tumors.
In 1954 Meigs reviewed 122 cases of abdominal or
pelvic lesions with ascites and hydrothorax, and found 84 typical
cases of Meigs' syndrome (6). The
importance of Meigs' syndrome is that the presence of ascites and
pleural effusion does not necessarily indicate that a pelvic mass
is malignant. The benign tumors in Meigs syndrome are usually
fibromas or fibrothecomas, and constitute 4% of all ovarian
neoplasms (7). Others include
mucinous cystadenomas and Brenner tumors of the ovary (8). Ascites probably occurs by means of a
transudative mechanism through the tumor surface, which exceeds the
peritoneum's resorptive capacity (9).
Other possible mechanisms include obstruction of peritoneal
lymphatics by the tumor or increased permeability of the
neovasculature with protein leakage. From the basic biological
point of view, inflammatory cytokines are known to induce capillary
leakage and third-space fluid accumulation in numerous gynecologic
and non-gynecologic disorders. The cytokines, including interleukin
(IL)-1β, IL-6, IL-8 and tumor necrosis factor (TNF)-α in the
interstitial fluid of Meigs' syndrome with ascites and hydrothorax
were investigated, and they all decreased following tumor removal,
with the exception of TNF-α (10).
The present study reported an uncommon case of a
benign ovarian thecoma, associated with hydrothorax, which mimicked
an ovarian malignancy. Surgery is the preferred treatment for
thecoma, and the present study suggested that the patient accept
the hysterectomy and bilateral salpingo-oophorectomy in order to
avoid endometrial cancer in postmenopausal women. However,
salpingo-oophorectomy may be used for older or weaker patients.
Increased attention must be paid to determine the surgical
procedures used, due to the common ovarian thecoma combined with
endometrial cancer.
References
|
1
|
Takemori M, Nishimura R and Hasegawa K:
Ovarian thecoma with ascites and high serum levels of CA125. Arch
Gynecol Obstet. 264:42–44. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen VW, Ruiz B, Killeen JL, Coté TR, Wu
XC and Correa CN: Pathology and classification of ovarian tumors.
Cancer. 97(Suppl 10): S2631–S2642. 2003. View Article : Google Scholar
|
|
3
|
Nocito AL, Sarancone S, Bacchi C and
Tellez T: Ovarian thecoma: Clinicopathological analysis of 50
cases. Ann Diagn Pathol. 12:12–16. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tavassoli FA, Mooney E and Gersell DJ: Sex
cord-stromal tumors. Tumors of the breast and female genital
organs. Tavassoli FA and Deville P: (Lyon). IARC Press. 149–151.
2003.
|
|
5
|
Scully RE, Young RH and Clement PB:
Stromal tumors. In: Tumors of the ovary, maldevelopment gonads,
fallopian tube and broad ligament. Atlas of tumor pathology. Rosai
J: (Washington). Armed Forces Institute of Pathology. 189–197.
1998.
|
|
6
|
Meigs JV: Fibroma of the ovary with
ascites and hydrothorax; Meigs' syndrome. Am J Obstet Gynecol.
67:962–985. 1954. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nemeth AJ and Patel SK: Meigs syndrome
revisited. J Thorac Imaging. 18:100–103. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Buttin BM, Cohn DE and Herzog TJ: Meigs'
syndrome with an elevated CA 125 from benign Brenner tumors. Obstet
Gynecol. 98:980–982. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Samanth KK and Black WC III: Benign
ovarian stromal tumors associated with free peritoneal fluid. Am J
Obstet Gynecol. 107:538–545. 1970.PubMed/NCBI
|
|
10
|
Abramov Y, Anteby SO, Fasouliotis SJ and
Barak V: The role of inflammatory cytokines in Meigs' syndrome.
Obstet Gynecol. 99:917–919. 2002. View Article : Google Scholar : PubMed/NCBI
|