Case report
An 18-year-old woman patient was admitted to
hospital with complaints of abdominal distension, and the patient
had experienced intermittent mild abdominal pain since birth. The
abdominal girth had slowly increased in diameter over the previous
18 years, and the patient's general condition of health was poor,
presenting symptoms including fatigue, fever, nausea, vomiting,
decreased appetite and weight loss. No specific urinary or bowel
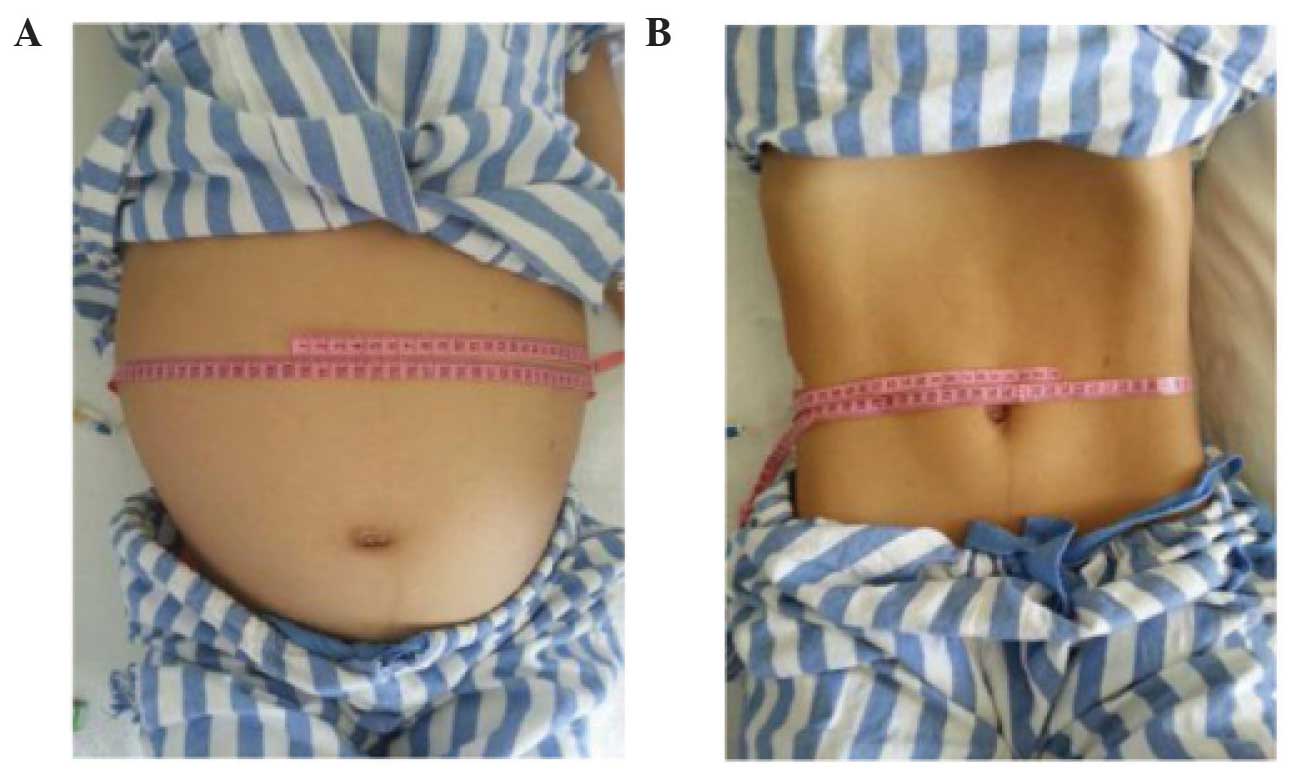
dysfunction was identified. Clinically, the diagnosis of a giant
hydronephrose (GH) was made, and upon physical examination, an
extremely distended abdomen was revealed, with a palpable mass in
the all-flank region (Fig. 1A). Bowel
sounds could not be auscultated, and neither was there any shifting
dullness. An examination of the other systems failed to disclose
any noteworthy phenomena.
The blood laboratory analyses revealed a
concentration of blood urea nitrogen of 30.1 mg/dl, and a level of
creatinine of 1.56 mg/dl. The level of hemoglobin was 12 g/dl, and
the hematocrit was determined to be 45.7%, whereas tumor markers
were all revealed to be in normal range, The results of the urine
analysis revealed a red blood cell count of 32/high power field
(HPF) a white blood cell count of 6/HPF and a yeast cell count of
5/HPF. Blood sugar, phosphate, liver function, serum calcium, serum
amylase and electrolyte analyses all yielded results within the
normal limits. A diagnostic aspiration performed from the area of
abdominal swelling revealed the presence of urine. Ultrasonography
revealed the presence of a massive hypoechoic lesion occupying
almost the entire abdomen, which exerted pressure on the bowel on
the left-hand side. The left kidney appeared normal, although the
right kidney could not be identified. A cystic lesion revealed
multiple septations, which were likely to have arisen from the
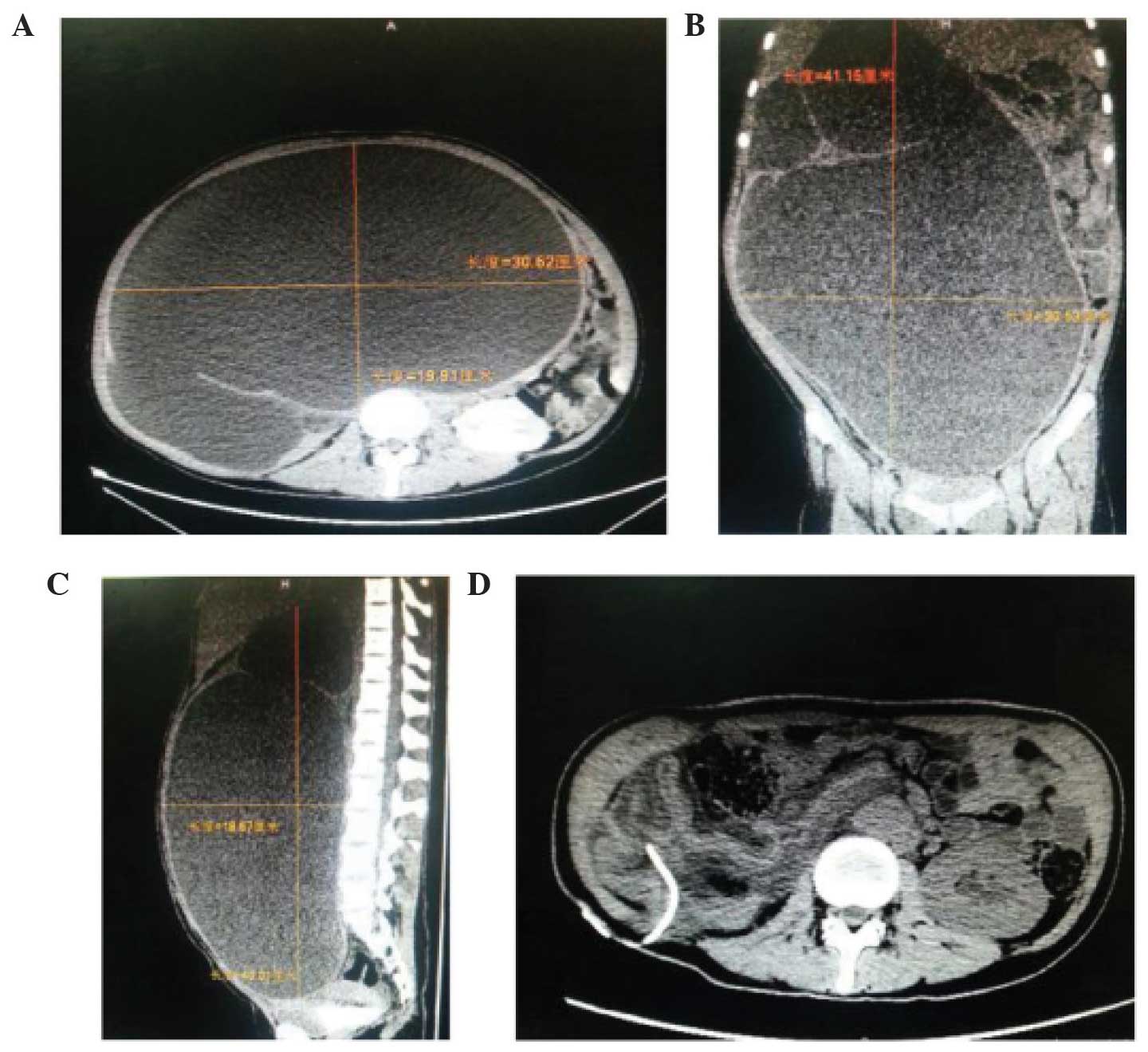
right kidney. A computerized tomography (CT) scan revealed a large
abdominal mass of water density in the all-abdomen area, which
comprised a huge cystic mass (41.5×30.5×30.5 cm; Fig. 2A–C) that, in the right kidney,
occupied almost the entire abdominal cavity. This mass had
displaced the small intestine, colon, pancreas, spleen and the left
kidney. After admission, the cystic mass was punctured, and a total
of ~24 l urinal fluid was drained by urethral catheterization over
a period of 8 days (3 liters each day). There was an improvement in
the general condition of the patient: The distended abdomen
decreased in size (Fig. 1B), the
level of urea declined to 1.42 g/l, and the level of creatinine was
63 mg/l. The results of subsequent laboratory analyses and urine
culture were normal. A subsequent CT scan revealed an almost
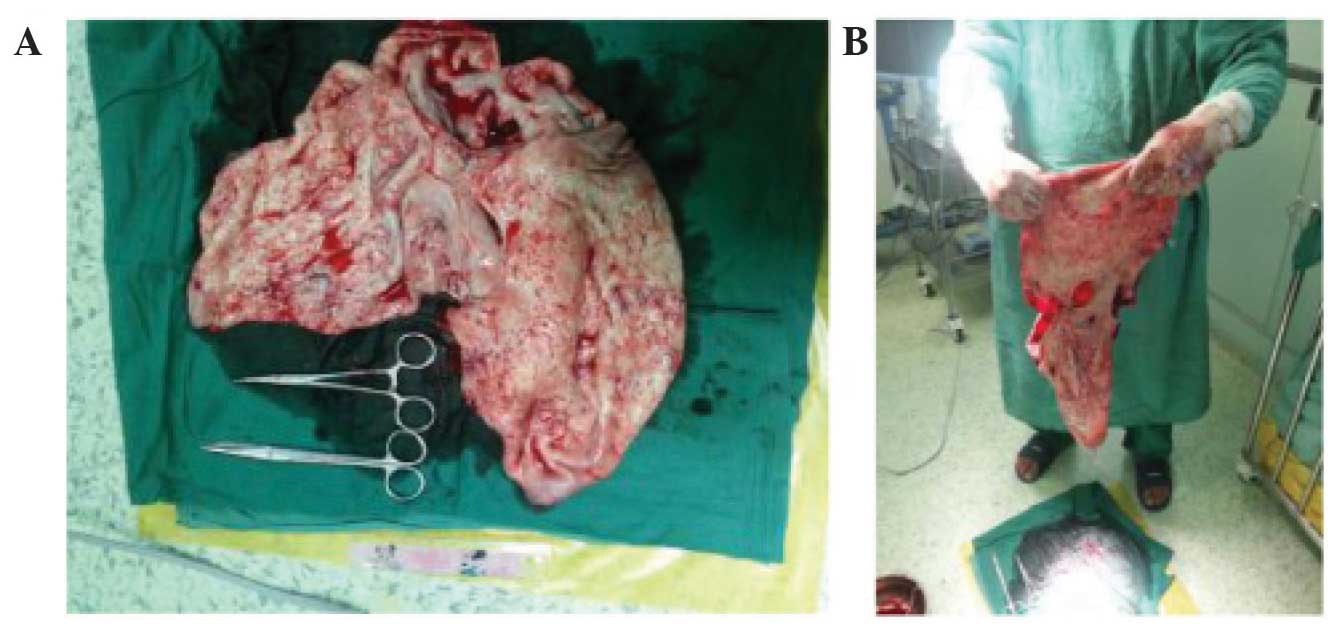
complete disappearance of the hydronephrosis (Fig. 2D). A right nephrectomy was performed:
When an incision was made in the right lumbar region, the cyst
presented as a retroperitoneal soft cystic dilatation mass, lacking
in definition, measuring almost 30×20×15 cm (Fig. 3), which was able to adhere to adjacent
organs, including the liver and the pelvic cavity, lifting the
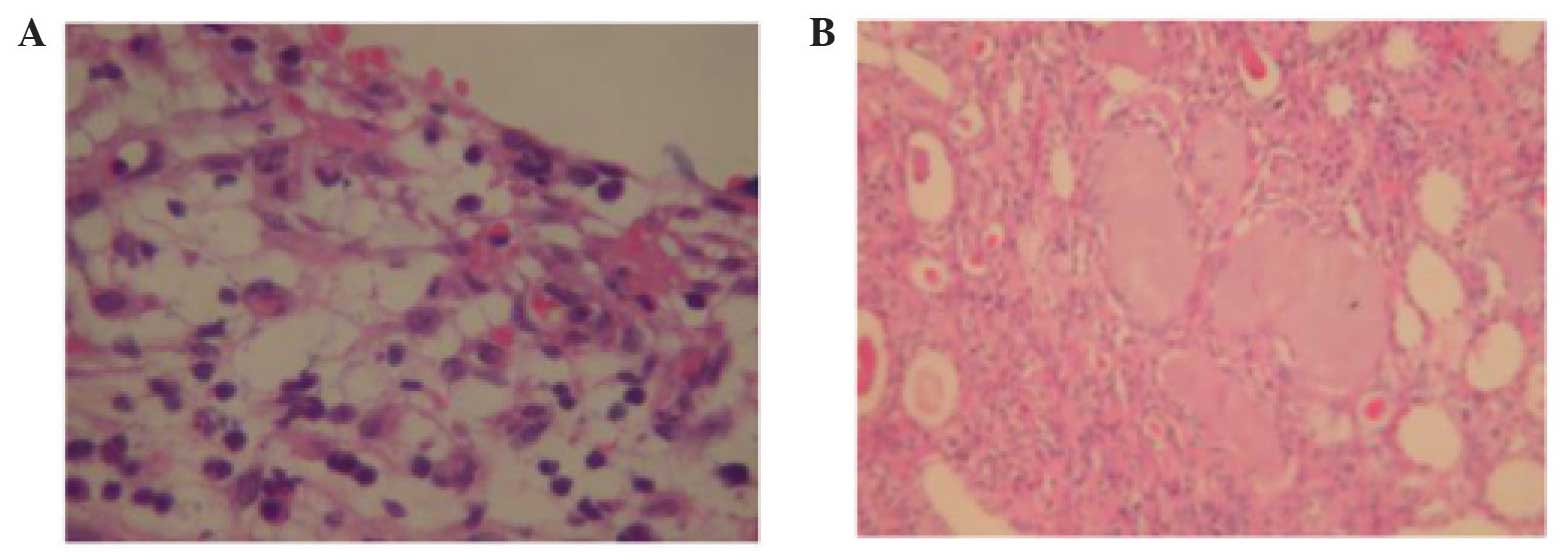
cecum and the ascending colon. The ureter was normal, and
ureteropelvic junction obstruction (UPJO) was established as the
cause of GH. The pathological tissue sections are shown in Fig. 4.
Discussion
GH is a rare urological condition, which occurs in
patients of all ages, defined as the presence of >1 liter of
fluid in the collecting system (1).
It is considered to develop gradually over a long period of time.
Symptomatic nephrolithiasis and hydronephrosis more frequently
present as clinical conditions, and GH is a rare clinical
phenomenon. Although numerous cases of GH have been reported in the
literature, only a few of them contained > 2 liters of fluid
(Table I). In the present case
report, the hydronephrotic kidney contained 24 l urine, and GHs
seldom fill the entire abdomenal space, as had occurred in our
patient. The most common cause of GH, as detailed in the
literature, is a condition caused by UPJO, although stone disease,
trauma, renal ectopy and ureteral tumors have also been reported
(2). In the present study, UPJO was
the cause of GH.
 | Table I.List of documented cases of GHs
reported in the literature of the present study. |
Table I.
List of documented cases of GHs
reported in the literature of the present study.
| Patient no. | Year | Age/gender | Refs. | Size of mass
(cm)/quantity of fluid (ml) | Initial symptoms | Treatment | Cause of GH |
|---|
| 1 | 2009 | 65/F | (1) | 30×20×25/15,000 | Fatigue, fever | Nephrectomy | Obstruction |
| 2 | 2003 | 78/F | (2) | 35×30×25/30,000 | Nausea, vomit,
fatigue, fever, weight loss | Puncture/drainage,
nephrectomy | Tumor |
| 3 | 2012 | 42/M | (3) | 44×32×30/20,000 | Weight loss | Nephrectomy | Bladder neck
obstruction |
| 4 | 2013 | 82/M | (4) | 30×21×10/4,500 | Fever | Nephrectomy | Tumor |
| 5 | 2009 | 45/M | (5) | 30×20×20/15,000 | Anemia, liver
dysfunction | Nephrectomy | Stone |
| 6 | 2014 | 83/M | (6) | 20×16×22/4,000 | Fatigue, nausea,
vomit, weight loss | Puncture/drain
nephrectomy | Ureteral stone |
The clinical symptoms of GH are non-specific, and
may present with vague symptoms, including an increased abdominal
girth due to the presence of a mass in the flank. GH is a slowly
progressive disease, and a huge abdominal mass or distended abdomen
may cause pain, and be symptomatic of hematuria, recurrent urinary
tract infection or other symptoms or complications described in the
literature, including nausea, fatigue or dyspepsia, urinary tract
infection, loss of weight, renal insufficiency, gross hematuria
resulting from trauma in the area, the compression of surrounding
structures, or even rupture of the kidney (3). Ultrasonography and CT scans have
facilitated the diagnosis of hydronephrosis, and a case of GH may
be defined as the presence of hydronephrosis occupying a
hemiabdomen, which meets, or extends beyond, the midline, and which
extends at least five or six vertebral bodies in length (4). However, in a number of cases, a
differential diagnosis between GH and other cystic formations
proves to be difficult. Therefore, as demonstrated in the present
case report, an accurate diagnosis of GH in individual cases
remains challenging. Contrast-enhanced CT of the abdomen and the
pelvis provides the ‘gold standard’ for an accurate diagnosis of
GH, and other useful diagnostic imaging techniques include
abdominal radiography and intravenous urography. The ideal
treatment for GH is nephrectomy, and this is the procedure of
choice; other treatment options in a functional kidney include
percutaneous nephrostomy, reduction pyeloplasty with nephropexy
calycoureterostomy, and calycocystostomy (5). In spite of the widespread use of
prenatal ultrasound and the development of new diagnostic
techniques, GH is encountered in all age groups. A
puncture/drainage procedure may be performed in cases where the
condition of the patient does not allow other treatments to be
performed, or where hemodynamic changes may occur following a
sudden abdominal decompression (6).
In the present case study, the patient underwent a right
nephrectomy and was discharged on postoperative day 8. In
conclusion, GH is a rare condition, which is associated with the
occurrence of cystic abdominal masses, and the puncture/drainage
procedure or nephrectomy provides the most suitable method for
surgical intervention.
References
|
1
|
Vishwanath M, Pattanshetti MK, Swamy SI,
Godhi AS and Metgud SC: Giant hydronephrosis. Indian J Surg.
72:359–360. 2009.
|
|
2
|
Schrader AJ, Anderer G, von Knobloch R,
Heidenreich A and Hofmann R: Giant hydronephrosis mimicking
progressive malignancy. BMC Urol. 3:42003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tazi MF, Riyach O, Ahallal Y, Mellas S,
Khallouk A, El Fassi MJ and Farih MH: Giant urinary bladder and
bilateral giant hydronephrosis due to bladder neck obstruction: One
case report and literature review. Case Rep Urol.
2012:8175192012.PubMed/NCBI
|
|
4
|
Mediavilla E, Ballestero R, Correas MA and
Gutierrez JL: About a case report of giant hydronephrosis. Case Rep
Urol. 2013:2579692013.PubMed/NCBI
|
|
5
|
Wu CC and Sun GH: Giant hydronephrosis.
Mayo Clin Proc. 84:9542009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Golcuk Y, Ozsarac M, Eseroglu E and Yuksel
MB: Giant hydronephrosis. West J Emerg Med. 15:3562014. View Article : Google Scholar : PubMed/NCBI
|