Introduction
Hyperthyroidism is associated with accelerated bone
remodeling, reduced bone density and osteoporosis (1). These changes in bone metabolism are
associated with a negative calcium balance, hypercalciuria and,
rarely, hypercalcemia, which occurs in hyperthyroidism alone or due
to concurrent hyperparathyroidism. Asymptomatic serum calcium
elevation has been documented in ≤20% of patients with
hyperthyroidism and is associated with increased bone resorption
(2). Symptomatic hypercalcemia has
been reported as an uncommon occurrence in hyperthyroidism, with
calcium levels rarely exceeding 12 mg/dl (3). We herein report the case of a patient
with hyperthyroidism, who presented with persistent arthralgia,
hypercalcemia and vomiting as the initial manifestations.
Case presentation
A 53-year-old post-menopausal woman (menopause at 46
years of age) presented with a 6-year history of joint pain and
edema, with intermittent nausea and vomiting over the past 6
months. Initially, the patient had experienced edema and pain of
the metacarpophalangeal and proximal interphalangeal joints, and
the wrist, knee and ankle joints, accompanied by periods of
stiffness in the morning, lasting ~20 min. The patient was
diagnosed with rheumatoid arthritis and was prescribed appropriate
medication at a local hospital; however, the symptoms did not
subside with the treatment. Three years later, the patient was
diagnosed with osteoarthritis by the orthopedist in our hospital
and treated with topical diclofenac (Voltaren) and intra-articular
injection of betamethasone, without significant benefit. The
patient's general condition gradually deteriorated, with
intermittent nausea and vomiting developing over the previous 6
months; she was referred to another hospital, where the diagnosis
of rheumatoid arthritis was again considered. Prednisone (15
mg/day) was initiated and after ~10 days, the patient was
discharged. Prednisone treatment was continued at a lower dosage (5
mg/day); however, the symptoms of nausea and vomiting reappeared.
After 1 month, thyroid function tests showed a thyroid-stimulating
hormone (TSH) level of 0.001 µIU/ml (normal range, 0.55–4.78
µIU/ml); triiodothyronine (T3) 6.07 ng/ml (normal range,
0.60–1.81 ng/ml) and thyroxine (T4) 30 µg/dl (normal
range, 4.50–10.90 µg/dl), consistent with a diagnosis of
hyperthyroidism. Therapy with methimazole (10 mg three times a day)
and propranolol (10 mg three times a day) was initiated. However,
the symptoms of nausea and vomiting persisted and after 2 weeks the
patient was referred to our hospital.
At first appearance, the patient looked wasted and
chronically ill. The findings of the physical examination at the
time of admission were as follows: Temperature, 36.8°C; pulse, 100
beats/min; respiration, 20 breaths/min; and blood pressure, 120/80
mmHg. No ophthalmopathy, lymphadenopathy or jaundice were observed,
although there was mild anemia. The thyroid gland was enlarged,
without an audible bruit. The heart and lungs were normal. No fine
finger tremor was observed, the extremities appeared normal and the
neurological examination was negative.
The laboratory tests revealed a TSH level of 0.003
µIU/ml, a T3 level of 4.44 ng/ml, a T4 level
of >30 µg/dl, a free T3 level of 14.03 pg/ml (normal
range, 2.3–4.2 pg/ml), and a free T4 level of 8.84 ng/dl
(normal range, 0.89–1.76 ng/dl). The TSH receptor antibodies,
thyroid peroxidase antibodies and thyroglobulin antibodies were
negative. The hemoglobin level was 90 g/l and the white blood cell
count was 5.54×109/l, with a normal differential count.
The liver and renal function tests were normal. The serum calcium
was 2.96 mmol/l (normal range, 2.10–2.80 mmol/l), with a normal
albumin level and a serum phosphate level of 0.84 mmol/l (normal,
0.97–1.60 mmol/l). The serum intact parathyroid hormone level was
4.8 pg/ml (normal range, 14–72 pg/ml), the 25-hydroxy vitamin D was
52.13 nmol/l (normal range, 47.7–144 nmol/l), osteocalcin was 128.8
ng/ml (normal range, 12.8–55 ng/ml) and bone-specific alkaline
phosphatase was 22.1 ng/ml (normal range, 7.3–22.4 ng/ml). The
urine calcium was 11.29 mmol/24 h (normal range, 2.5–7.5 mmol/24
h), and the urine phosphate was 9.55 mmol/24 h (normal range, 23–48
mmol/24 h). The serum immunoglobulin (Ig) A, IgG and IgM levels
were normal. The urine was negative for Bence-Jones protein. The
erythrocyte sedimentation rate, components 3, 4, and rheumatoid
factor were normal. Parathyroid scintigraphy revealed no
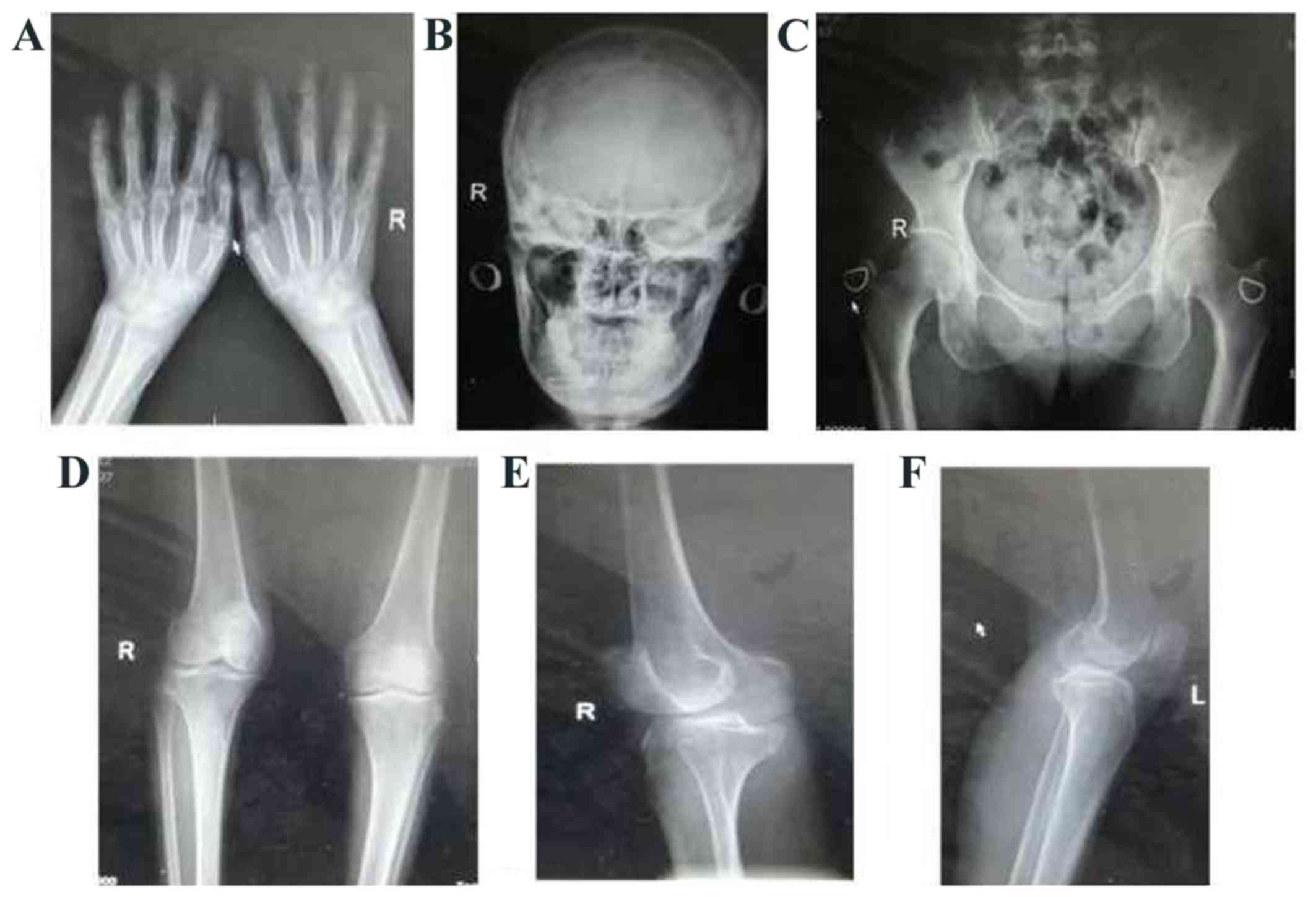
abnormalities. X-ray examination of the skeleton revealed mildly
narrowed hand and knee joint gaps as a result of degenerative
changes, and osteoporosis in the joints of the hand, skull, knees
and pelvis (Fig. 1). The bone
mineral density, as assessed by quantitative ultrasound, was 0.254
g/cm2 (T-score, −3.2).
Hypercalcemia was considered to be secondary to
hyperthyroidism and methimazole therapy (10 mg three times a day)
was continued. The patient was also managed with hydration by
intravenous infusion of isotonic saline for 3 days, after which
time the serum calcium level remained at 3.0 mmol/l and serum
phosphate at 1.25 mmol/l. Therefore, therapy with salmon calcitonin
(50 IU once a day) and alendronate (70 mg once a week) was
initiated. After 1 week, the serum calcium and phosphate levels had
decreased to 2.71 and 1.26 mmol/l, respectively, and were
normalized to 2.44 and 1.19 mmol/l, respectively, after 2 weeks.
The thyroid function tests revealed a TSH level of 0.001 µIU/ml,
T3 of 1.87 ng/ml and a T4 of 13.90 µg/dl. The
patient's appetite gradually improved and she started to gain
weight. Calcitonin was then discontinued, while therapy with
methimazole (30 mg/day) and alendronate (70 mg/week) was
continued.
Three months after the start of anti-thyroid
treatment, the patient had no nausea, vomiting or joint pain and
had recovered a normal appetite, with a weight gain of ~10 kg.
Euthyroidism was achieved and the serum calcium and phosphate
levels returned to normal (2.31 and 1.12 mmol/l, respectively);
therefore, the dose of methimazole was reduced (5 mg three times a
day) and alendronate was discontinued. Six months later, the
patient's serum calcium and phosphate levels remained normal, and
her osteocalcin levels had diminished compared with the previously
measured level (80.40 ng/ml).
Discussion
The most common cause of hypercalcemia in
hyperthyroidism is concurrent primary hyperparathyroidism; however,
in 15–20% of the cases, alterations in calcium metabolism are
related solely to hyperthyroidism (2). A linear correlation exists between
serum calcium levels and the parameters of thyroid function; this
effect is more pronounced in the >60 age group (4).
Hypercalcemia secondary to hyperthyroidism is
non-PTH dependent, with enhanced bone resorption and calcium
mobilization proposed as the underlying mechanism. The high
circulating levels of interleukin (IL)-6 associated with
hyperthyroidism stimulate bone osteoclastic activity and alter
osteoblast-osteoclast coupling (5).
Furthermore, T3 increases the sensitivity of the bone to
IL-6 (6). Elevated serum calcium
levels may inhibit antidiuretic hormone and PTH secretion (7), increase urine output and promote
calcium and phosphate excretion from the renal tubules by
interaction with the calcium-sensing receptors in the loops of
Henle (8). Additionally, the
intestinal absorption of calcium is reduced as a result of the
reduced PTH secretion, as well as thyroid hormone inhibition of
1,25-dihydroxyvitamin D synthesis and interference with vitamin D
metabolism.
The incidence of osteoporosis in patients with
hyperthyroidism is ~20–50%. Despite a diagnosis of hyperthyroidism,
our patient presented with extensive osteoporosis and significantly
increased osteocalcin levels, indicative of increased osteoblastic
activity and bone formation. Following treatment for
hyperthyroidism, the osteocalcin levels were reduced, but remained
higher than normal; these observations are consistent with a
previous report by Nagasaka et al, who reported that bone
resorption occurs in untreated patients with Graves' thyrotoxicosis
and is rapidly ameliorated following normalization of thyroid
hormone levels. However, the accelerated bone formation persists
for at least 4–8 months (9). With
regard to the patient described herein, further follow-up is
required to determine whether her osteoporosis was secondary to
hyperthyroidism or also due to menopause.
Control of hyperthyroidism is the main treatment for
hypercalcemia and osteoporosis secondary to hyperthyroidism, with
anti-thyroid drug therapy as the first choice. However, in the
initial stages, when anti-thyroid treatment has not achieved full
efficacy, prompt reduction in serum calcium may be required,
particularly if hypercalcemia or other symptoms are severe. In
resistant cases, other modalities of treatment, such as calcitonin
or diphosphate, may be required in addition to general management
with saline hydration or diuretics. However, 131Iodine treatment
may lead to the destruction of thyroid follicular cells and
increased thyroid hormone release, which may even induce a
hypercalcemic crisis; therefore, this treatment should be avoided
in hyperthyroid patients with hypercalcemia (10).
The patient in the present case did not exhibit
clinical manifestations typical of hyperthyroidism; as a result,
she was misdiagnosed with rheumatoid arthritis and osteoarthritis
for several years, with poor efficacy of the prescribed treatment.
The hypercalcemia was confirmed to be secondary to hyperthyroidism,
as supported by the relief of her symptoms and resolution of
hypercalcemia with treatment of the underlying thyroid condition.
Therefore, clinicians should include hyperthyroidism in the
differential diagnosis of persistent arthralgia, even if the
patients do not present with the typical symptoms of
hyperthyroidism.
References
|
1
|
Reddy PA, Harinarayan CV, Sachan A, Suresh
V and Rajagopal G: Bone disease in thyrotoxicosis. Indian J Med
Res. 135:277–286. 2012.PubMed/NCBI
|
|
2
|
Baxter JD and Bondy PK: Hypercalcemia of
thyrotoxicosis. Ann Intern Med. 65:429–442. 1966. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Alikhan Z and Singh A: Hyperthyroidism
manifested as hypercalcemia. South Med J. 89:997–998. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Szabó ZS and Ritzl F: Hypercalcemia in
hyperthyroidism. Role of age and goiter type. Klin Wochenschr.
59:275–279. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Akalin A, Colak O, Alatas O and Efe B:
Bone remodelling markers and serum cytokines in patients with
hyperthyroidism. Clin Endocrinol (Oxf). 57:125–129. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Iqbal AA, Burgess EH, Gallina DL, Nanes MS
and Cook CB: Hypercalcemia in hyperthyroidism: Patterns of serum
calcium, parathyroid hormone, and 1,25-dihydroxyvitamin D3 levels
during management of thyrotoxicosis. Endocr Pract. 9:517–521. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mosekilde L, Eriksen EF and Charles P:
Effects of thyroid hormones on bone and mineral metabolism.
Endocrinol Metab Clin North Am. 19:35–63. 1990.PubMed/NCBI
|
|
8
|
Marx SJ, Sharp ME, Krudy A, Rosenblatt M
and Mallette LE: Radioimmunoassay for the middle region of human
parathyroid hormone: Studies with a radioiodinated synthetic
peptide. J Clin Endocrinol Metab. 53:76–84. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nagasaka S, Sugimoto H, Nakamura T, Kusaka
I, Fujisawa G, Sakuma N, Tsuboi Y, Fukuda S, Honda K, Okada K, et
al: Antithyroid therapy improves bony manifestations and bone
metabolic markers in patients with Graves' thyrotoxicosis. Clin
Endocrinol (Oxf). 47:215–221. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Du W, Cuige L, Liu X, et al: A case of
calcium crisis after 131I therapy of Graves' disease. Chin J Integr
Med. 51:315–316. 2012.
|