Introduction
Colon cancer is one of the most common cancers
worldwide, with the predominant type being adenocarcinoma (1). Squamous cell carcinoma (SCC) of the
colon is a rare pathological type, representing ~0.06% of all
colorectal malignancies (2). The
clinical characteristics of colon SCC are similar to those of
adenocarcinoma. The treatment of SCC is mainly surgical resection.
In terms of chemotherapy, there is currently no standard regimen
for the treatment of colon SCC and its prognosis has been reported
to be worse compared with that of adenocarcinoma. We herein present
the case of a 58-year-old male patient diagnosed with adenosquamous
carcinoma of the colon, who was treated with systemic
gemcitabine-based neoadjuvant chemotherapy, followed by surgery and
adjuvant chemotherapy.
Case report
A 58-year old male patient was hospitalized with a
5-month history of abdominal pain accompanied by a mass in the
right lower quadrant. The symptoms gradually worsened and the
patient experienced hematochezia, anorexia and weight loss of ~10%
body weight. The patient had a history of smoking and alcohol
consumption.
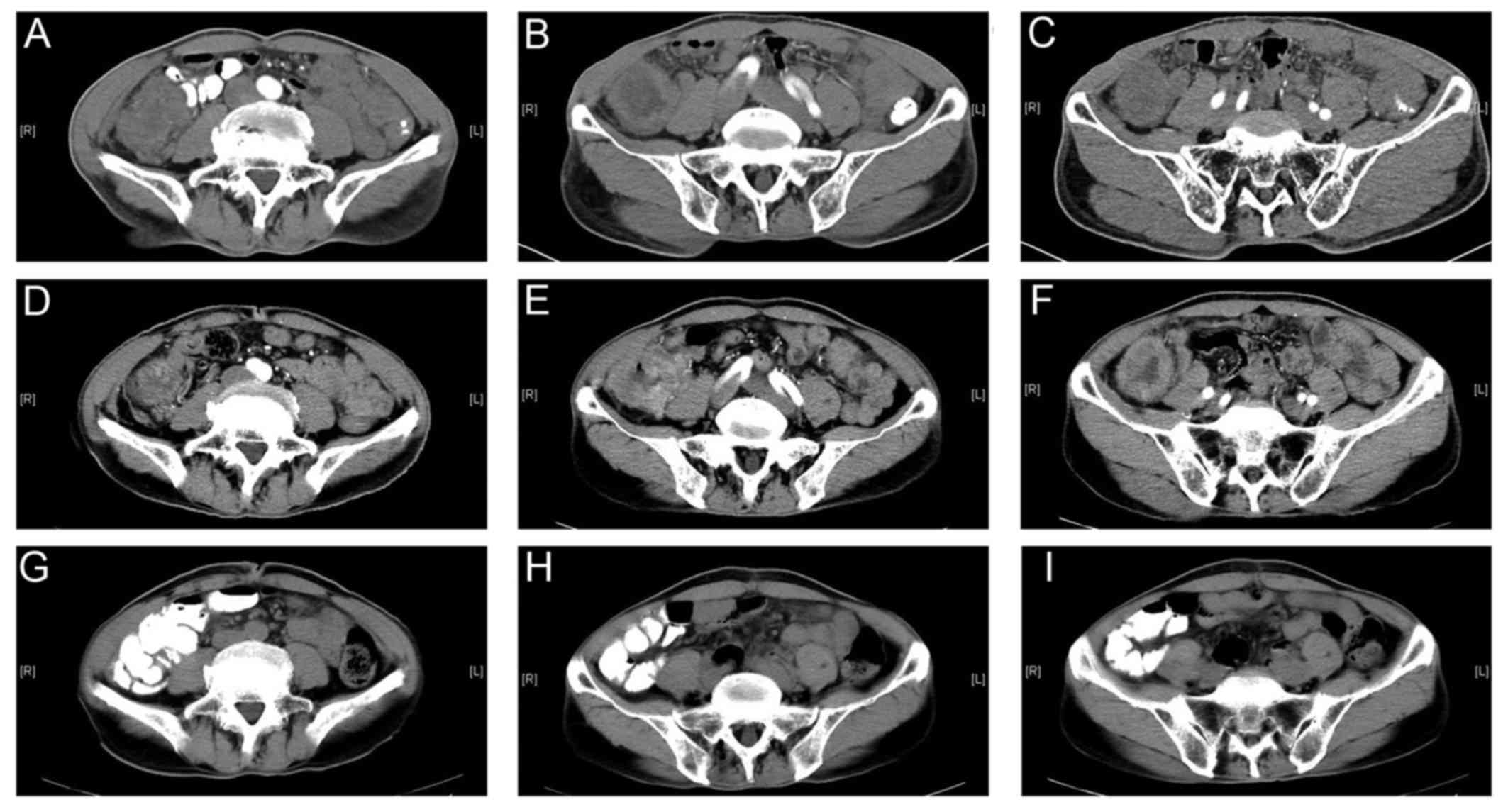
The contrast-enhanced computed tomography (CT) scan
revealed a mass located in the lower part of the ascending colon.
On enteroscopy, space-ocuppying lesions were identified in the
rectum and ascending colon. The result of the pathological
examination of the rectal lesion was moderately differentiated
adenocarcinoma, while sampling from the colon was unsuccessful. In
order to obtain a sample from the lesion of the ascending colon,
the patient underwent CT-guided biopsy twice. The first time the
pathology result was poorly differentiated carcinoma, while the
immunohistochemistry findings were consistent with adenosquamous
carcinoma with a predominant SCC component, whereas the second
biopsy was used for verification due to the atypical pathological
characteristics (Table I).
 | Table I.Pathological characteristics of the
tumors. |
Table I.
Pathological characteristics of the
tumors.
| A, Pathology of the
colon tumor |
|---|
|
|---|
| 1st CT guided
biopsy | 2nd CT guided
biopsy | Surgery |
|---|
| Poorly
differentiated carcinoma, tumor cells arranged in nests, partially
seen intercellular junctions. CK+, P63+,
Syn−, CgA−, CD56−,
CK7+, CK20−, CDX-2−,
GATA-3−, Ki-67 70% | Poorly
differentiated carcinoma, consistent with adenosquamous carcinoma
with a predominant SCC component. P63+, P40+,
CK7+, CK20−, CDX-2−,
Syn− | Poorly
differentiated SCC (ulcerative type) with involvement of outer
serosal fat and vessels, with or without PNI. Infiltration of
pericolic lymph nodes (1/22). CK5/6+, P40+,
P63+, CK7+ (partly) CK20−,CDX
2−, Syn−, CD31+ (indicating
vascular invasion) |
|
| B, Pathology of the
rectal tumor |
|
|
| Endoscopic
biopsy | Surgery |
|
|
| Rectal
adenocarcinoma | Moderately
differentiated adenocarcinoma (ulcerative type) with serosal
involvement, without resection margin involvement. Perirectal lymph
nodes free of metastasis (0/13). PMS-2+,
MLH1+, MSH2−, MSH6−, Her-2 (0),
S-100− (neural invasion), CD31+ (indicating
extensive vascular invasion), Ki 67 80–90%. |
After excluding distant metastasis by thoracic CT,
whole-abdomen CT, whole-body bone scan emission computed tomography
and head magnetic resonance imaging, the patient received
neoadjuvant chemotherapy. The chemotherapy regimen was designed
based on the therapeutic regimen for adenocarcinoma and the poor
prognosis of this pathological subtype. The chemotherapy was
conducted every 21 days and included gemcitabine (1,000
mg/m2 intravenously, 1,800 mg on d1 and 1,600 mg on d8),
oxaliplatin (130 mg/m2 intravenously, 200 mg on d1) and
capecitabine (625 mg/m2 orally, 1,000 mg bid on days
d1-14). The capecitabine dose was reduced by 50% in order to avoid
severe side effects. Between August 18th, 2015 and September 24th,
2015, the patient received two cycles of neoadjuvant chemotherapy.
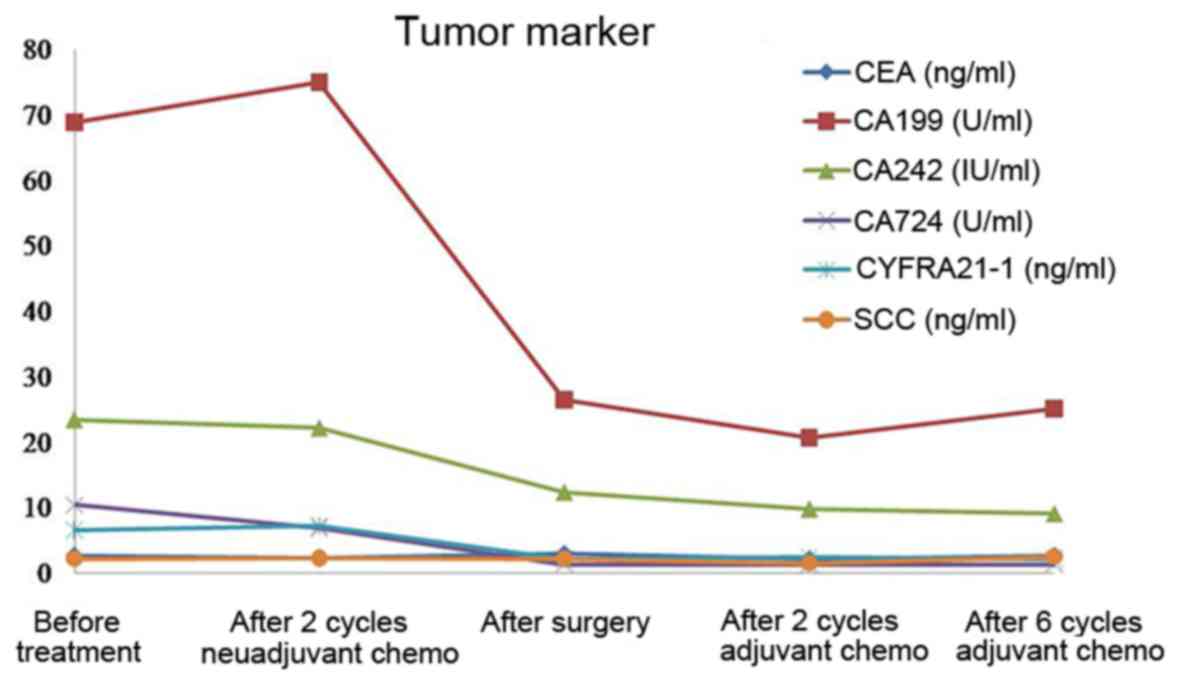
Contrast-enhanced CT (Fig. 1) and
measurement of tumor marker serum levels were used to evaluate
treatment efficacy (Table IB).
According to the World Health Organization criteria, the evaluation
was stable disease.
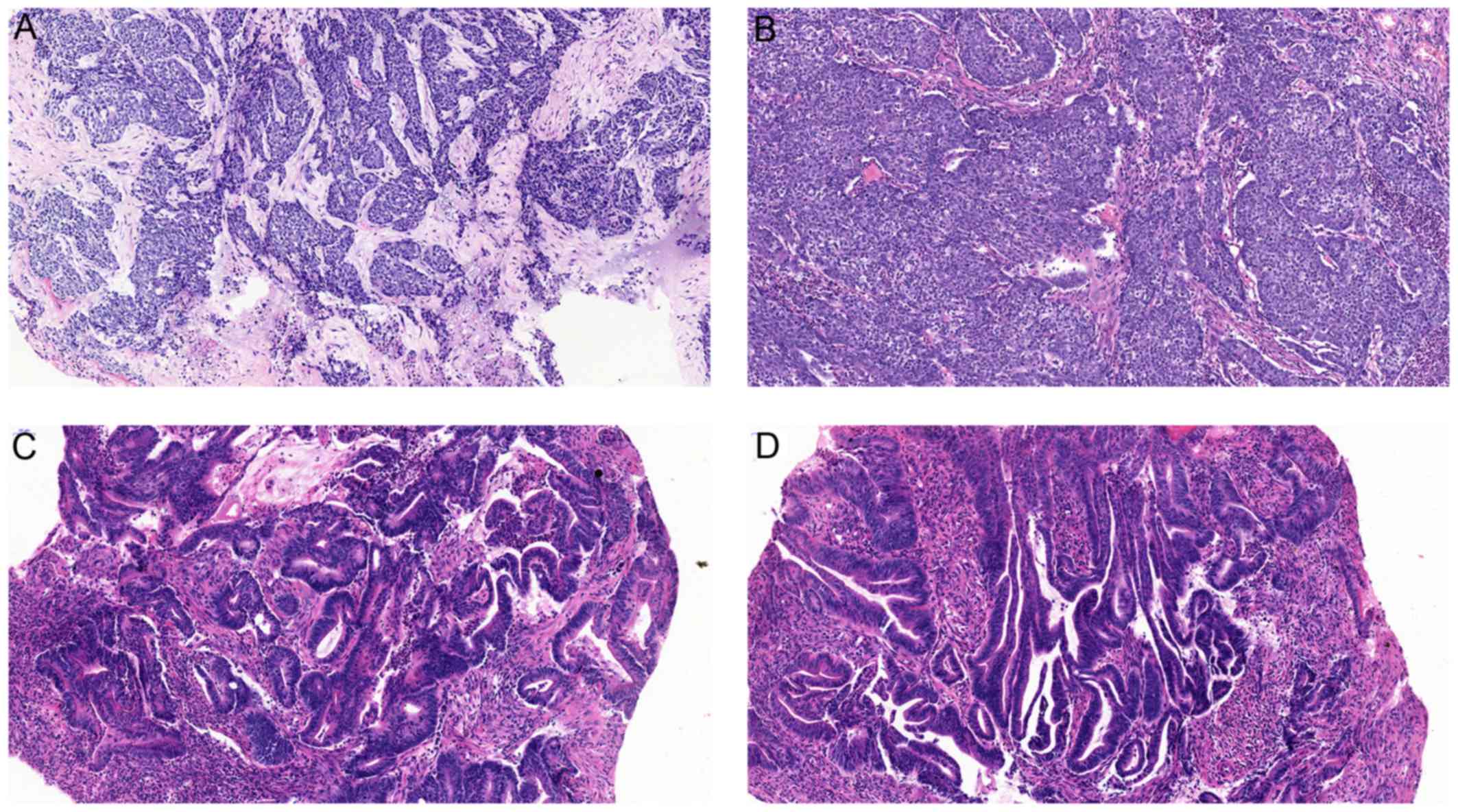
On October 19th, 2015, the patient underwent radical
right hemicolectomy and radical resection of rectal carcinoma
(Dixon operation). The postsurgical pathology of the colon lesion
revealed poorly differentiated SCC (ulcerative type) with
infiltration of pericolic lymph nodes (1/22). The postsurgical
pathology of the rectal lesion was moderately differentiated
adenocarcinoma with no perirectal lymph node metastasis (0/13)
(Fig. 2).
After surgery, the patient received six cycles of
adjuvant chemotherapy within 2 months and remained disease-free
(Figs. 1 and 3) up to the time this article was submitted
(date of last follow-up, June 10th, 2016; follow-up time, 10.5
months).
Discussion
SCC is uncommon in the colon and rectum and was
first reported by Herxheimer in 1907 (3). In 1927, White et al published
the first report of primary adenosquamous cell carcinoma of the
colon in the English medical literature (4). From then on, apart from a few small
series from large institutions, the majority of the data comes from
individual case reports (5–10).
Generally, SCC in the colon and rectum occurs in the
anal canal, the lining of which is squamous epithelium, or in the
lower part of the rectum adjacent to the anal canal, where it may
originate from the nearby squamous or transitional cells.
Adenosquamous carcinoma is a malignancy containing glandular and
squamous histological components. However, the histogenesis of the
squamous component remains unclear. There are several opinions as
follows: i) Differentiation from stem cells (11–15); ii)
squamous metaplasia (16–23); and iii) differentiation from
adenocarcinoma (24–29).
The optimal treatment for SCC has not been
determined due to its low incidence. Generally, the treatment is
based on that for adenocarcinomas, which is predominantly surgery
combined with chemotherapy and radiotherapy. With the advances in
chemotherapy and radiotherapy, the accuracy of determining stage
and evaluating response, a multitude of recent studies utilizing
various treatment regimens have been reported, which included
5-fluorouracil (5FU)/mitomycin C, 5FU, 5FU/cisplatin,
capecitabine/cisplatin, capecitabine, raltitrexed/oxaliplatin and
S-1 (10,11,30–52).
The most important prognostic predictor is cancer
stage. Colorectal SCC follows the same route of lymphatic spread as
adenocarcinoma; additionally, they share similar metastatic sites,
such as the liver, lung and bone (53). In 1996, Petrelli et al
described the cases of 5 men and 2 women diagnosed with
adenosquamous carcinoma originating from the colon or rectum. All
the patients were treated surgically. Chemotherapy was used as
adjuvant treatment, or in patients with local recurrence and
distant metastasis. The median overall survival was 23 months
(7). In 1999, Cagir et al
reported a review of 145 cases of adenosquamous carcinoma using the
National Cancer Institute Surveillance, Epidemiology, and End
Results database program over a 20-year period (1973–1992).
Patients with localized disease (stages I and II) exhibited
survival curves similar to those with comparably staged
adenocarcinoma. Adenosquamous cancer patients with regional disease
(stages IIB and III) had a shorter survival compared with patients
with similar-stage colorecal adenocarcinoma. Patients with stage IV
adenosquamous carcinoma had a significantly shorter survival
compared with those with comparably staged adenocarcinoma (2). Frizelle et al published a report
on 44 patients with adenosquamous carcinoma and SCC. In that study,
they found the prognosis to be similar to that of colorectal
adenocarcinoma for stage I–II node-negative disease. However, when
nodal disease occurs, the prognosis is worse than that expected for
adenocarcinoma of similar stage. The characteristics predicting a
poor prognosis included right-sided lesions, ulcerated or annular
carcinomas, node-positive disease, grade 3–4 cancer and stage IV
disease (54).
Gemcitabine (2′-deoxy-2′,2′-difluorocytidine
monohydrochloride) is a potent and specific pyrimidine nucleoside
antimetabolite, which is structurally analogous to deoxycytidine.
In in vitro and phase I studies, gemcitabine had shown
activity against various types of hematological and solid tumors
(55–58). Furthermore, its antitumor activity
had been confirmed in clinical practice. Gemcitabine has been used
to treat patients with non-small-cell lung cancer, pancreatic,
bladder and breast cancer, malignant mesothelioma and ovarian
cancer. In preclinical studies, gemcitabine was found to act
synergistically with a number of DNA-damaging agents, including
platinum drugs and irradiation. Gemcitabine also has an extremely
mild toxicity profile, which has prompted investigations of the
agent in combination with other cytotoxic compounds. To the best of
our knowledge, gemcitabine was selected as part of the chemotherapy
regimen in colon SCC for the first time in the present case. As a
result, the patient had achieved a PFS of 10 months by the time
this article was submitted.
Colorectal SCC is rare, and its treatment is
currently largely based on that applied for adenocarcinoma cases.
As reported, SCC patients with stage III–IV disease have a poorer
prognosis compared with those with adenocarcinoma. Thus, a more
aggressive chemotherapeutic approach may be a viable choice for
patients with a good performance status. In the present case,
gemcitabine, oxaliplatin and capecitabine were selected as the
chemotherapy regimen, which has never been reported in clinical
practice. The PFS was 10 months until this manuscript was
submitted. Thus, this new regimen may provide a reference for the
future treatment for SCC of the colorectum.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2016. CA Cancer J Clin. 66:7–30. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cagir B, Nagy MW, Topham A, Rakinic J and
Fry RD: Adenosquamous carcinoma of the colon, rectum, and anus:
Epidemiology, distribution, and survival characteristics. Dis Colon
Rectum. 42:258–263. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Herxheimer G: Ober heterologue cancroide.
Beitr Pathol Anat. 41:348–412. 1907.
|
|
4
|
White CP and Brunton CE: Some uncommon
tumours. J Pathol. 30:313–330. 1927. View Article : Google Scholar
|
|
5
|
Crissman JD: Adenosquamous and squamous
cell carcinoma of the colon. Am J Surg Pathol. 2:47–54. 1978.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cerezo L, Alvarez M, Edwards O and Price
G: Adenosquamous carcinoma of the colon. Dis Colon Rectum.
28:597–603. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Petrelli NJ, Valle AA, Weber TK and
Rodriguez-Bigas M: Adenosquamous carcinoma of the colon and rectum.
Dis Colon Rectum. 39:1265–1268. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rajan R, Baqar A and Menon T: An
interesting case of primary squamous cell carcinoma of the colon
with synchronous metastatic adenocarcinoma. Clin Case Rep.
2:323–325. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
TA II Schneider, Birkett DH and AM III
Vernava: Primary adenosquamous and squamous cell carcinoma of the
colon and rectum. Int J Colorectal Dis. 7:144–147. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lyttle JA: Primary squamous carcinoma of
the proximal large bowel. Report of a case and review of the
literature. Dis Colon Rectum. 26:279–282. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nahas CS, Shia J, Joseph R, Schrag D,
Minsky BD, Weiser MR, Guillem JG, Paty PB, Klimstra DS, Tang LH, et
al: Squamous-cell carcinoma of the rectum: A rare but curable
tumor. Dis Colon Rectum. 50:1393–1400. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jaworski RC, Biankin SA and Baird PJ:
Squamous cell carcinoma in situ arising in inflammatory cloacogenic
polyps: Report of two cases with PCR analysis for HPV DNA.
Pathology. 33:312–314. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hicks JD and Cowling DC: Squamous-cell
carcinoma of the ascending colon. J Pathol Bacteriol. 70:205–212.
1955. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ouban A, Nawab RA and Coppola D:
Diagnostic and pathogenetic implications of colorectal carcinomas
with multidirectional differentiation: A report of 4 cases. Clin
Colorectal Cancer. 1:243–248. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Michelassi F, Mishlove LA, Stipa F and
Block GE: Squamous-cell carcinoma of the colon. Experience at the
University of Chicago, review of the literature, report of two
cases. Dis Colon Rectum. 31:228–235. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
LeBlanc LJ, Buie LA and Dockerty MB:
Squamous-cell epithelioma of the rectum. Ann Surg. 131:392–399.
1950. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lugo M and Putong PB: Metaplasia. An
overview. Arch Pathol Lab Med. 108:185–189. 1984.PubMed/NCBI
|
|
18
|
Lee SD, Haggitt RC and Kimmey MB: Squamous
metaplasia of the rectum after argon plasma coagulation.
Gastrointest Endosc. 52:683–685. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cabrera A and Pickren JW: Squamous
metaplasia and squamous-cell carcinoma of the rectosigmoid. Dis
Colon Rectum. 10:288–297. 1967. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Woods WG: Squamous cell carcinoma of the
rectum arising in an area of squamous metaplasia. Eur J Surg Oncol.
13:455–458. 1987.PubMed/NCBI
|
|
21
|
Dukes CE: The Surgical Significance of the
Unusual in the Pathology of Intestinal Tumours: Imperial Cancer
Research Fund Lecture delivered at the Royal College of Surgeons of
England on 23rd November, 1948. Ann R Coll Surg Engl. 4:1169–1170.
1949.
|
|
22
|
Reeve DRE: Squamous metaplasia in the
healing of chronic colonic ulcers of the rat. J Pathol. 117:15–22.
1975. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wells HG, Slye M and Holmes HF:
Comparative Pathology of Cancer of the Alimentary Canal, with
Report of Cases in Mice Studies in the Incidence and Inheritability
of Spontaneous Tumors in Mice: 34th Report. Am J Cancer.
33:223–238. 1938.
|
|
24
|
Williams GT, Blackshaw AJ and Morson BC:
Squamous carcinoma of the colorectum and its genesis. J Pathol.
129:139–147. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Chen KTK: Colonic adenomatous polyp with
focal squamous metaplasia. Hum Pathol. 12:848–849. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Almagro UA, Pintar K and Zellmer RB:
Squamous metaplasia in colorectal polyps. Cancer. 53:2679–2682.
1984. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kontozoglou T: Squamous metaplasia in
colonic adenomata: Report of two cases. J Surg Oncol. 29:31–34.
1985. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Forouhar F: Neoplastic colonic polyp with
extensive squamous metaplasia. Case report. Tumori. 70:99–103.
1984.PubMed/NCBI
|
|
29
|
Lundquest DE, Marcus JN, Thorson AG and
Massop D: Primary squamous cell carcinoma of the colon arising in a
villous adenoma. Hum Pathol. 19:362–364. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Theodosopoulos TK, Marinis AD, Dafnios NA,
Vassiliou JG, Samanides LD, Carvounis EE and Smyrniotis VE:
Aggressive treatment of metastatic squamous cell carcinoma of the
rectum to the liver: A case report and a brief review of the
literature. World J Surg Oncol. 4:492006. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Choi H, Lee HW, Ann HW, Kim JK, Kang HP,
Kim SW, Ku NS, Han SH, Kim JM and Choi JY: A case of rectal
squamous cell carcinoma with metachronous diffuse large B cell
lymphoma in an HIV-infected patient. Infect Chemother. 46:257–260.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Martinez-Gonzalez MD, Takahashi T,
Leon-Rodriguez E, Gamboa-Dominguez A, Lome C, Garcia-Blanco MC,
Bezaury P and Moran MA: Case report of primary squamous carcinoma
of the rectum. Revista de investigación clínica; organo del
Hospital de Enfermedades de la Nutrición. 48:453–456. 1996.
|
|
33
|
Rasheed S, Yap T, Zia A, McDonald PJ and
Glynne-Jones R: Chemo-radiotherapy: An alternative to surgery for
squamous cell carcinoma of the rectum-report of six patients and
literature review. Colorectal Dis. 11:191–197. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Iannacone E, Dionisi F, Musio D, Caiazzo
R, Raffetto N and Banelli E: Chemoradiation as definitive treatment
for primary squamous cell cancer of the rectum. World J Radiol.
2:329–333. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Funahashi K, Nemoto T, Koike J, Kurihara
A, Shiokawa H, Ushigome M, Kaneko T, Arai K, Nagashima Y, Koda T,
et al: Chemoradiation therapy with S-1 for primary squamous cell
carcinoma of the rectum: Report of three cases. Surg Case Rep.
1:142015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Wang MLC, Heriot A, Leong T and Ngan SYK:
Chemoradiotherapy in the management of primary squamous-cell
carcinoma of the rectum. Colorectal Dis. 13:296–301. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ozuner G, Aytac E, Gorgun E and Bennett A:
Colorectal squamous cell carcinoma: A rare tumor with poor
prognosis. Int J Colorectal Dis. 30:127–130. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Jeong BG, Kim DY and Kim SY: Concurrent
chemoradiotherapy for squamous cell carcinoma of the rectum.
Hepatogastroenterology. 60:512–516. 2013.PubMed/NCBI
|
|
39
|
Matsuda A, Takahashi K, Yamaguchi T,
Matsumoto H, Miyamoto H, Kawakami M, Kawachi H, Suzuki H, Furukawa
K, Tajiri T, et al: HPV infection in an HIV-positive patient with
primary squamous cell carcinoma of rectum. Int J Clin Oncol.
14:551–554. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Brammer RD, Taniere P and Radley S:
Metachronous squamous-cell carcinoma of the colon and treatment of
rectal squamous carcinoma with chemoradiotherapy. Colorectal Dis.
11:219–220. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Péron J, Bylicki O, Laude C, Martel-Lafay
I, Carrie C and Racadot S: Nonoperative management of squamous-cell
carcinoma of the rectum. Dis Colon Rectum. 58:60–64. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Gelas T, Peyrat P, Francois Y, Gerard JP,
Baulieux J, Gilly FN, Vignal J and Glehen O: Primary squamous-cell
carcinoma of the rectum: Report of six cases and review of the
literature. Dis Colon Rectum. 45:1535–1540. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Al Hallak MN, Hage-Nassar G and Mouchli A:
Primary Submucosal Squamous Cell Carcinoma of the Rectum Diagnosed
by Endoscopic Ultrasound: Case Report and Literature Review. Case
Rep Gastroenterol. 4:243–249. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Tronconi MC, Carnaghi C, Bignardi M, Doci
R, Rimassa L, Di Rocco M, Scorsetti M and Santoro A: Rectal
squamous cell carcinoma treated with chemoradiotherapy: Report of
six cases. Int J Colorectal Dis. 25:1435–1439. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Kulaylat MN, Doerr R, Butler B,
Satchidanand SK and Singh A: Squamous cell carcinoma complicating
idiopathic inflammatory bowel disease. J Surg Oncol. 59:48–55.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Kassir R, Baccot S, Bouarioua N, Petcu CA,
Dubois J, Boueil-Bourlier A, Patoir A, Epin A, Ripamonti B and
Tiffet O: Squamous cell carcinoma of middle rectum: Literature
review. Int J Surg Case Rep. 5:86–90. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Berardi RS, Chen HP and Lee SS: Squamous
cell carcinoma of the colon and rectum. Surg Gynecol Obstet.
163:493–496. 1986.PubMed/NCBI
|
|
48
|
Pikarsky AJ, Belin B, Efron J, Woodhouse
S, Weiss EG, Wexner SD and Nogueras JJ: Squamous cell carcinoma of
the rectum in ulcerative colitis: Case report and review of the
literature. Int J Colorectal Dis. 22:445–447. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Yeh J, Hastings J, Rao A and Abbas MA:
Squamous cell carcinoma of the rectum: A single institution
experience. Tech Coloproctol. 16:349–354. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Seshadri RA, Pancholi M, Jayanand SB and
Chandrasekar S: Squamous cell carcinoma of the rectum: Is
chemoradiation sufficient? J Cancer Res Ther. 11:6642015.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Musio D, De Felice F, Manfrida S, Balducci
M, Meldolesi E, Gravina GL, Tombolini V and Valentini V: Squamous
cell carcinoma of the rectum: The treatment paradigm. Eur J Surg
Oncol. 41:1054–1058. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Clark J, Cleator S, Goldin R, Lowdell C,
Darzi A and Ziprin P: Treatment of primary rectal squamous cell
carcinoma by primary chemoradiotherapy: Should surgery still be
considered a standard of care? Eur J Cancer. 44:2340–2343. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Torricelli P: Rectal cancer staging. Surg
Oncol. 16 Suppl 1:S49–S50. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Frizelle FA, Hobday KS, Batts KP and
Nelson H: Adenosquamous and squamous carcinoma of the colon and
upper rectum: A clinical and histopathologic study. Dis Colon
Rectum. 44:341–346. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Abbruzzese JL, Grunewald R, Weeks EA,
Gravel D, Adams T, Nowak B, Mineishi S, Tarassoff P, Satterlee W,
Raber MN, et al: A phase I clinical, plasma, and cellular
pharmacology study of gemcitabine. J Clin Oncol. 9:491–498. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Csoka K, Liliemark J, Larsson R and Nygren
P: Evaluation of the cytotoxic activity of gemcitabine in primary
cultures of tumor cells from patients with hematologic or solid
tumors. Semin Oncol. 22 Suppl 11:47–53. 1995.PubMed/NCBI
|
|
57
|
Von Hoff DD; San Antonio Drug Development
Team, : Activity of gemcitabine in a human tumor cloning assay as a
basis for clinical trials with gemcitabine. Invest New Drugs.
14:265–270. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Pollera CF, Ceribelli A, Crecco M, Oliva C
and Calabresi F: Prolonged infusion gemcitabine: A clinical phase I
study at low- (300 mg/m2) and high-dose (875 mg/m2) levels. Invest
New Drugs. 15:115–121. 1997. View Article : Google Scholar : PubMed/NCBI
|