Introduction
There have been several previous studies reporting
that various cytokines, including granulocyte colony-stimulating
factor (G-CSF) and interleukin 6 (IL-6), are produced by lung
carcinomas, particularly pleomorphic carcinomas previously
diagnosed as large cell carcinomas (1–7). G-CSF
production by cancer cells has been associated with the rapid
progression of the disease and with the poor prognosis.
Pleomorphic carcinoma of lung was first classified
in 1999 by the World Health Organization as a subset of sarcomatoid
carcinoma. This type of tumor is rare, accounting for 2–3% of all
cancer cases in a previous surgical series, but for <1% in
epidemiological studies (8).
Pleomorphic carcinoma is a poorly-differentiated non-small cell
lung carcinoma, which may consist of a squamous cell carcinoma,
adenocarcinoma or undifferentiated non-small cell carcinoma that
contains ≥10% spindle and/or giant cells or a carcinoma consisting
only of spindle and giant cells. Pleomorphic carcinoma of the lung
has been reported to have aggressive clinical course with a poor
response to chemotherapy and radiotherapy (8). The prognosis is significantly poorer
than that of most other subsets of non-small cell lung cancer, even
in early-stage disease.
G-CSF causes hypermetabolic uptake of bone marrow in
positron emission tomography (PET) using F-18-fluorodeoxyglucose
(FDG) (9,10). The current case encountered diffuse
FDG uptake in the bone marrow by G-CSF-producing pleomorphic
carcinoma prior to the tumor resection, and this uptake was
considered to have occurred due to the amount of G-CSF present.
Case report
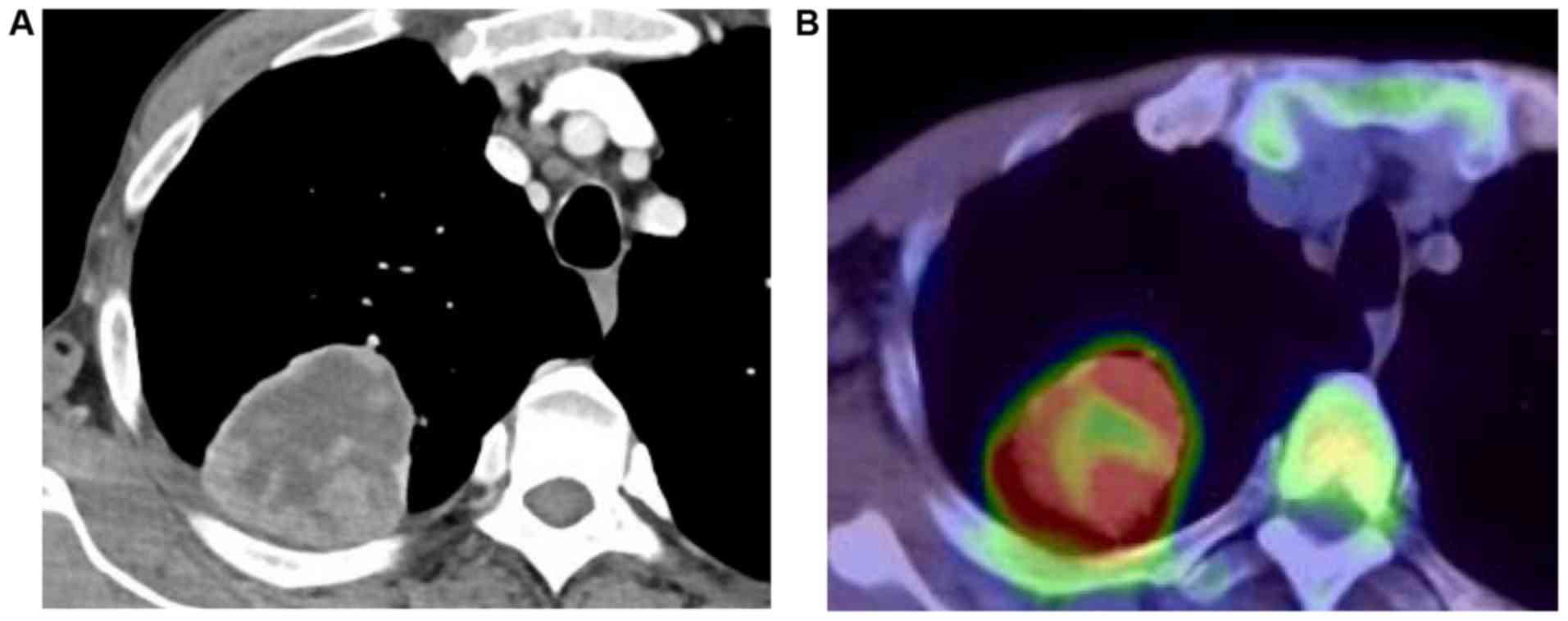
A 66-year-old male presenting with high-grade fever
and chest pain was admitted to Toho University Omori medical center
(Tokyo, Japan) in November, 2013. Chest computed tomography (CT)
revealed a 6-cm mass in the right upper lobe (Fig. 1A), invading the chest wall.
Laboratory testing identified marked peripheral leukocytosis
(2.27×109/l) and an elevated C-reactive protein [CRP,
13.3 mg/dl, normal range (NR), <0.25 mg/dl]. Serum
concentrations of G-CSF and IL-6 were 203 pg/ml (NR <39 pg/ml)
and 44.8 pg/ml (NR <4.4 pg/ml), respectively. 18
Fluorodeoxyglucose-positron emission tomography (FDG-PET) revealed
the localized uptake of the mass lesion in the right upper lobe
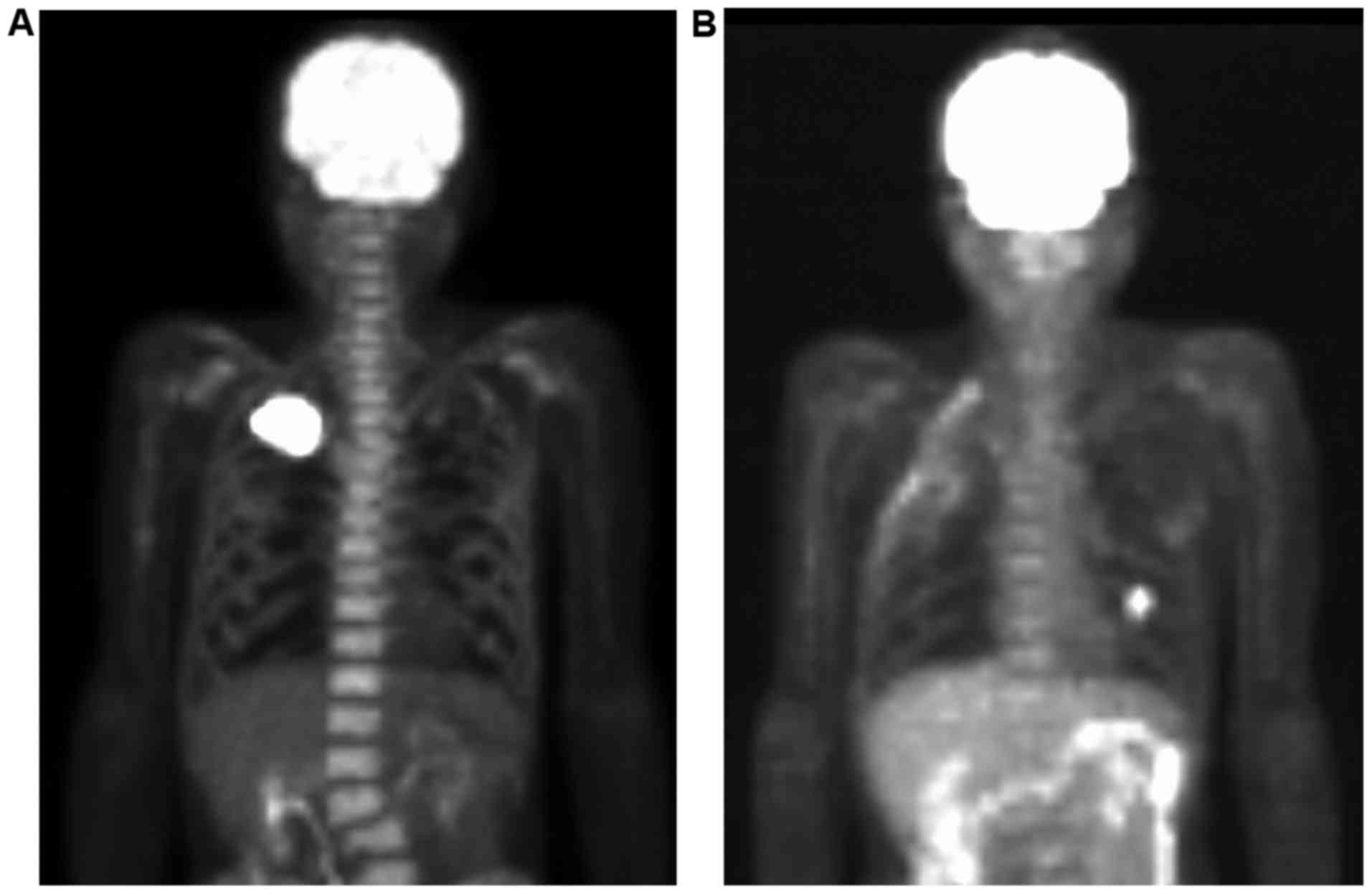
(Fig. 1B), and diffuse uptake in the
bone marrow (Fig. 2). Hematological
disease, including lymphoma and diffuse bone marrow metastases, was
excluded. The tumor cell was not identified by a bone-marrow
aspiration. The biopsy samples revealed hyperplasia of the normal
bone marrow, mainly granulocytes.
Histological examination of the transbronchial
biopsy specimens for the right lung tumor revealed a non-small cell
lung cancer (NSCLC). Based on a clinical diagnosis of NSCLC
(c-T3N0M0 stage IIB), the patient underwent right upper lobectomy
with chest wall resection, and a 6.8×6.0 cm tumor was completely
resected.
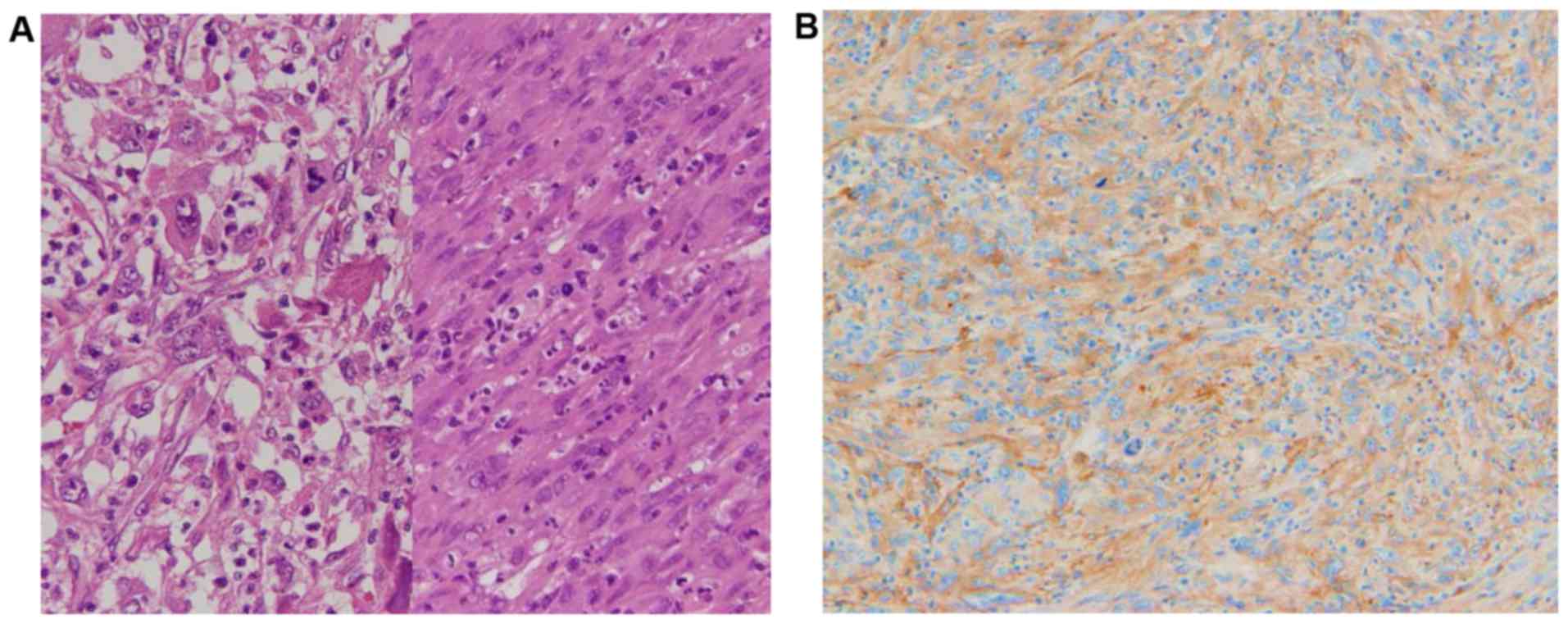
Histological examination using hematoxylin and eosin
staining revealed that the tumor was composed primarily of giant
cells and spindle cell surrounded by inflammatory cells (Fig. 3A). The patient was diagnosed with a
pulmonary pleomorphic carcinoma, pT3N0M0, stage IIB.
Immunohistochemical analysis of the resected tumor tissues revealed
positive staining for G-CSF (cat. no. ab9691; dilution, 1:100;
Abcam, Cambridge, UK) (Fig. 3B).
Tissue underwent heat-mediated antigen retrieval in sodium citrate
buffer (pH 6.0). The primary antibody was used at 0.25 µg/ml and
incubated with the sample at 4°C overnight. A horseradish
peroxidase-labeled polymer detection system was used with a
3,3′-diaminobenzidine chromogen (I-VIEW DAB universal kit, Roche
Tissue Diagnostics, Tokyo, Japan), according to the manufacturer's
protocol. The patient's high-grade fever, leukocytosis and the
elevated CRP level rapidly subsided following the resection.
Therefore, it was confirmed that the tumor was a G-CSF-producing
pulmonary pleomorphic carcinoma.
Following the surgical treatment, the patient
received two courses of adjuvant chemotherapy with cisplatin plus
S-1. However, 5 months after the resection, CT revealed a
metastatic pulmonary nodule in the left lower lobe. FDG-PET
identified abnormal FDG uptake in the nodule without diffuse uptake
in the bone marrow (Fig. 2). The
serum concentration of G-CSF showed marginal elevation as 45.3 (NR
<39 pg/ml). At the time of this report, 12 months after the
resection, the patient had undergone chemotherapy and was alive
with lung and brain metastases.
Written informed consent for the publication of this
case report and associated images was obtained from the
patient.
Discussion
Pleomorphic carcinoma of the lung is defined as a
group of poorly-differentiated NSCLCs that contains a component of
sarcoma or sarcoma-like elements and exhibits carcinomatous as well
as spindle and/or giant cell components (11). Pleomorphic carcinoma of the lung is
rare and accounts for <1% of all lung malignancies (12). Several previous studies have reported
that various cytokines, such as G-CSF and IL-6, were produced by
lung carcinomas, particularly pleomorphic carcinomas previously
diagnosed as large cell carcinomas (13). In the previous cases, the elevated
IL-6 levels may have contributed to high-grade fever and increased
CRP levels (14), and the increased
serum G-CSF levels may have contributed to leukocytosis and
hematopoietic activation (15). The
diagnostic criteria for CSF-producing tumors are as follows: i)
Extreme leukocytosis, ii) elevated CSF activity, iii) decreased WBC
count after resection and iv) proof of CSF production in the tumor
(16). In the present case, all
these criteria were fulfilled.
In FDG-PET, hypermetabolic activity of FDG following
administration of G-CSF corresponds to hyperactive bone marrow, and
lasts ~1 month (9,10). This increased FDG uptake in normal
bone marrow following G-CSF administration may be explained by
increased bone marrow metabolism and cellularity due to G-CSF
treatment. In the present case, the PET findings were due to bone
marrow hyperplasia induced by G-CSF produced by pulmonary
pleomorphic carcinoma, and the high uptake in the bone was absent
in the FDG-PET scan 5 months after the tumor resection, even in the
presence of small pulmonary metastasis and marginal serum G-CSF
elevation. These characteristic imaging findings are due to the
quantity of G-CSF, and are predicted to be useful for the diagnosis
of G-CSF-producing tumors.
In conclusion, the current study reported a case of
diffuse FDG uptake in the bone marrow of a patient with granulocyte
colony-stimulating factor-producing pleomorphic carcinoma of the
lung. Diffuse FDG uptake in bone marrow induced by G-CSF producing
pleomorphic carcinoma must be taken into consideration, in order
for it not to be misinterpreted as diffuse bone marrow metastases
or hematologic malignancy.
Acknowledgements
The present study was supported in part by
Grants-in-aid for Scientific Research (C) (grant nos. 15K10272 and
26462140) from the Japanese Ministry of Education, Culture, Sports,
Science and Technology.
Glossary
Abbreviations
Abbreviations:
|
FDG-PET
|
18-Fluorodeoxyglucose-positron
emission tomography
|
|
CRP
|
C-reactive protein
|
|
G-CSF
|
granulocyte colony-stimulating
factor
|
|
NSCLC
|
non-small cell lung cancer
|
|
IL-6
|
interleukin 6
|
|
CT
|
computed tomography
|
References
|
1
|
Sekido Y, Sato M, Usami N, Shigemitsu K,
Mori S, Maeda O, Yokoi T, Hasegawa Y, Yoshioka H and Shimokata K:
Establishment of a large cell lung cancer cell line (Y-ML-1B)
producing granulocyte colony-stimulating factor. Cancer Genet
Cytogenet. 137:33–42. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Inoue M, Minami M, Fujii Y, Matsuda H,
Shirakura R and Kido T: Granulocyte colony-stimulating factor and
interleukin-6-producing lung cancer cell line, LCAM. J Surg Oncol.
64:347–350. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Katsumata N, Eguchi K, Fukuda M, Yamamoto
N, Ohe Y, Oshita F, Tamura T, Shinkai T and Saijo N: Serum levels
of cytokines in patients with untreated primary lung cancer. Clin
Cancer Res. 2:553–559. 1996.PubMed/NCBI
|
|
4
|
Tsuyuoka R, Takahashi T, Sasaki Y,
Taniguchi Y, Fukumoto M, Suzuki A, Nakamura K, Kobayashi S, Kudo T
and Nakao K: Colony-stimulating factor-producing tumours:
Production of granulocyte colony-stimulating factor and
interleukin-6 is secondary to interleukin-1 production. Eur J
Cancer. 30A:2130–2136. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kimura H, Yamaguchi Y, Sun L, Iwagami S
and Sugita K: Establishment of large cell lung cancer cell lines
secreting hematopoietic factors inducing leukocytosis and
thrombocytosis. Jpn J Clin Oncol. 22:313–319. 1992.PubMed/NCBI
|
|
6
|
Matsuguchi T, Okamura S, Kawasaki C,
Shimoda K, Omori F, Hayashi S, Kimura N and Niho Y: Constitutive
production of granulocyte colony-stimulating factor and
interleukin-6 by a human lung cancer cell line, KSNY: Gene
amplification and increased mRNA stability. Eur J Haematol.
47:128–133. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Suzuki A, Takahashi T, Okuno Y, Nakamura
K, Tashiro H, Fukumoto M, Konaka Y and Imura H: Analysis of
abnormal expression of g-csf gene in a novel tumor cell line (KHC
287) elaborating G-CSF, IL-1 and IL-6 with co-amplification of
c-myc and c-ki-ras. Int J Cancer. 48:428–433. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yendamuri S, Caty L, Pine M, Adem S,
Bogner P, Miller A, Demmy TL, Groman A and Reid M: Outcomes of
sarcomatoid carcinoma of the lung: A Surveillance, Epidemiology,
and End Results Database analysis. Surgery. 152:397–402. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sugawara Y, Fisher SJ, Zasadny KR, Kison
PV, Baker LH and Wahl RL: Preclinical and clinical studies of bone
marrow uptake of fluorine-1-fluorodeoxyglucose with or without
granulocyte colony-stimulating factor during chemotherapy. J Clin
Oncol. 16:173–180. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kazama T, Swanston N, Podoloff DA and
Macapinlac HA: Effect of colony-stimulating factor and
conventional- or high-dose chemotherapy on FDG uptake in bone
marrow. Eur J Nucl Med Mol Imaging. 32:1406–1411. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Brambilla E, Travis WD, Colby TV, Corrin B
and Shimosato Y: The new World Health Organization classification
of lung tumours. Eur Respir J. 18:1059–1068. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ito K, Oizumi S, Fukumoto S, Harada M,
Ishida T, Fujita Y, Harada T, Kojima T, Yokouchi H and Nishimura M;
Hokkaido Lung Cancer Clinical Study Group, : Clinical
characteristics of pleomorphic carcinoma of the lung. Lung Cancer.
68:204–210. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fukuyama T, Ichiki Y, Yamada S, Shigematsu
Y, Baba T, Nagata Y, Mizukami M, Sugaya M, Takenoyama M, Hanagiri
T, et al: Cytokine production of lung cancer cell lines:
Correlation between their production and the
inflammatory/immunological responses both in vivo and in vitro.
Cancer Sci. 98:1048–1054. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Guo Y, Xu F, Lu T, Duan Z and Zhang Z:
Interleukin-6 signaling pathway in targeted therapy for cancer.
Cancer Treat Rev. 38:904–910. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mabuchi S, Morimoto A, Fujita M, Isohashi
K and Kimura T: G-CSF induces focal intense bone marrow FDG uptake
mimicking multiple bone metastases from uterine cervical cancer: A
case report and review of the literature. Eur J Gynaecol Oncol.
33:316–317. 2012.PubMed/NCBI
|
|
16
|
Asano S, Urabe A, Okabe T, Sato N and
Kondo Y: Demonstration of granulopoietic factor(s) in the plasma of
nude mice transplanted with a human lung cancer and in the tumor
tissue. Blood. 49:845–852. 1977.PubMed/NCBI
|