Introduction
Neurofibroma is usually associated with
neurofibromatosis (NF) type 1, and is among the most common
neurogenic tumors of the head and neck region in NF-1 patients.
Solitary cases that are not associated with NF-1 are rarely
reported. Among these, neurofibromas arising from peripheral
divisions of the trigeminal nerve are even rarer (1–6). In the
majority of cases, the tumor tends to extend outside the mandible,
leading to deformity of the jaw as the initial symptom (3,7). Other
common symptoms include pain or paresthesia of the affected
division of the trigeminal nerve.
The excision of tumors located in the infratemporal
fossa (ITF) is challenging, as such lesions are surrounded by the
skull base, mandible, lateral and medial pterygoid plate, maxillary
sinus and parapharyngeal structures. A number of approaches,
including the transtemporal-transzygomatic,
transzygomatic-transmandibular, transmaxillary, posterior
high-cervical and transoral approaches, may be applied, depending
on the tumor location (8–16). This study presents a rare case of a
trigeminal neurofibroma arising from the inferior alveolar nerve,
which was successfully excised via a combination of the
transtemporal and transoral-retromolar approaches, as well as a
discussion of these two approaches.
Case report
A 27-year-old man presented in June 2015 with
progressive numbness of the right jaw, and was diagnosed with an
ITF tumor at another hospital. The only neurological finding was
paresthesia in the area innervated by the mental nerve of the
trigeminal mandibular division. The patient's taste sensation was
normal, and the motor function of the trigeminal nerve was intact.
There was no inflammatory reaction in the parapharyngeal area or
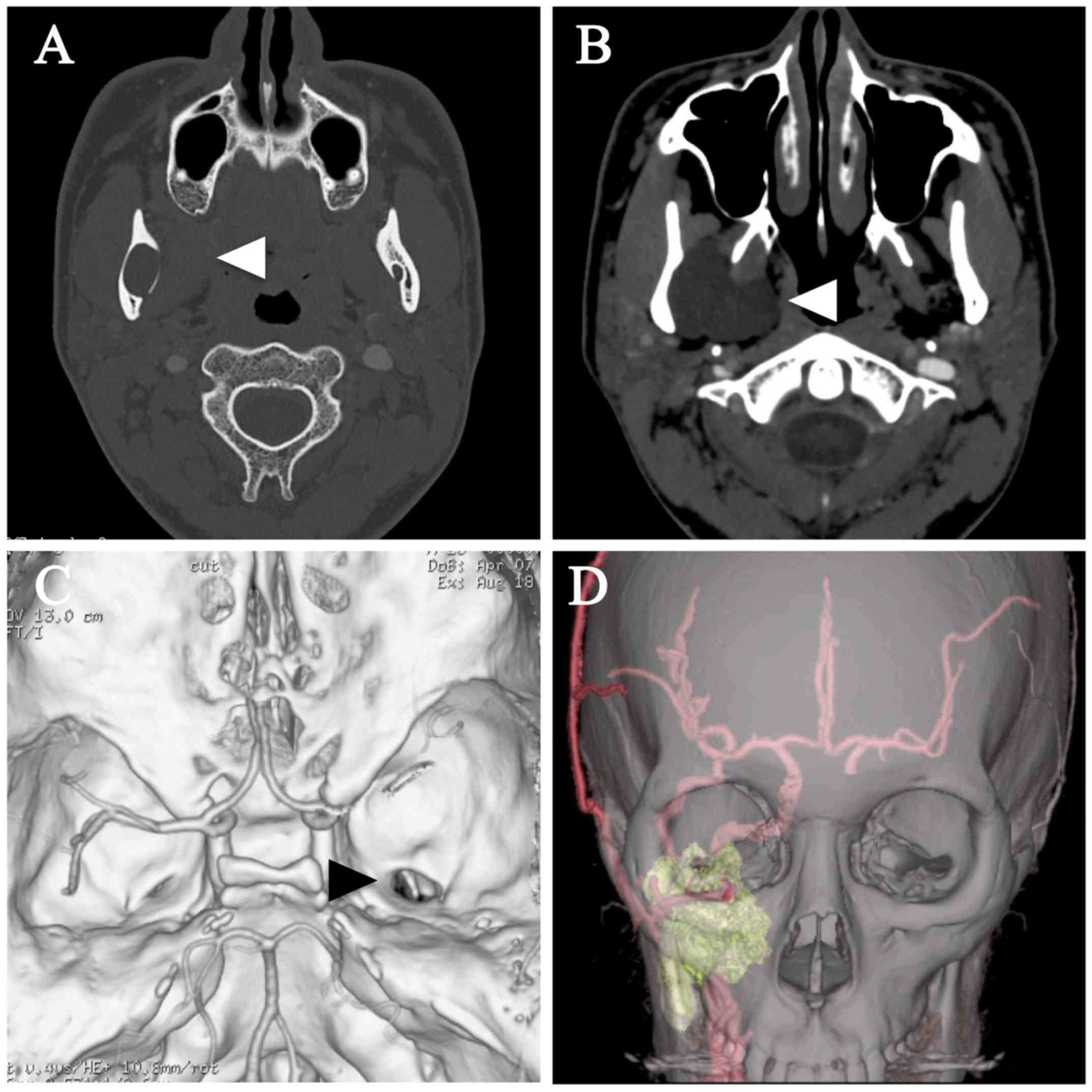
family history of NF. A computed tomography (CT) scan revealed a
non-enhanced mass in the infratemporal region, with an enlarged
mandibular canal and foramen ovale, suggesting a neurogenic tumor
along the third branch of the trigeminal nerve (Fig. 1A and B). A 3D-CT scan clearly
depicted the mass located within the mandible, occupying the ITF
and widening the foramen ovale. The internal carotid artery was
displaced posteriorly, and the maxillary artery ran along the
anterior surface of the tumor (Fig. 1C
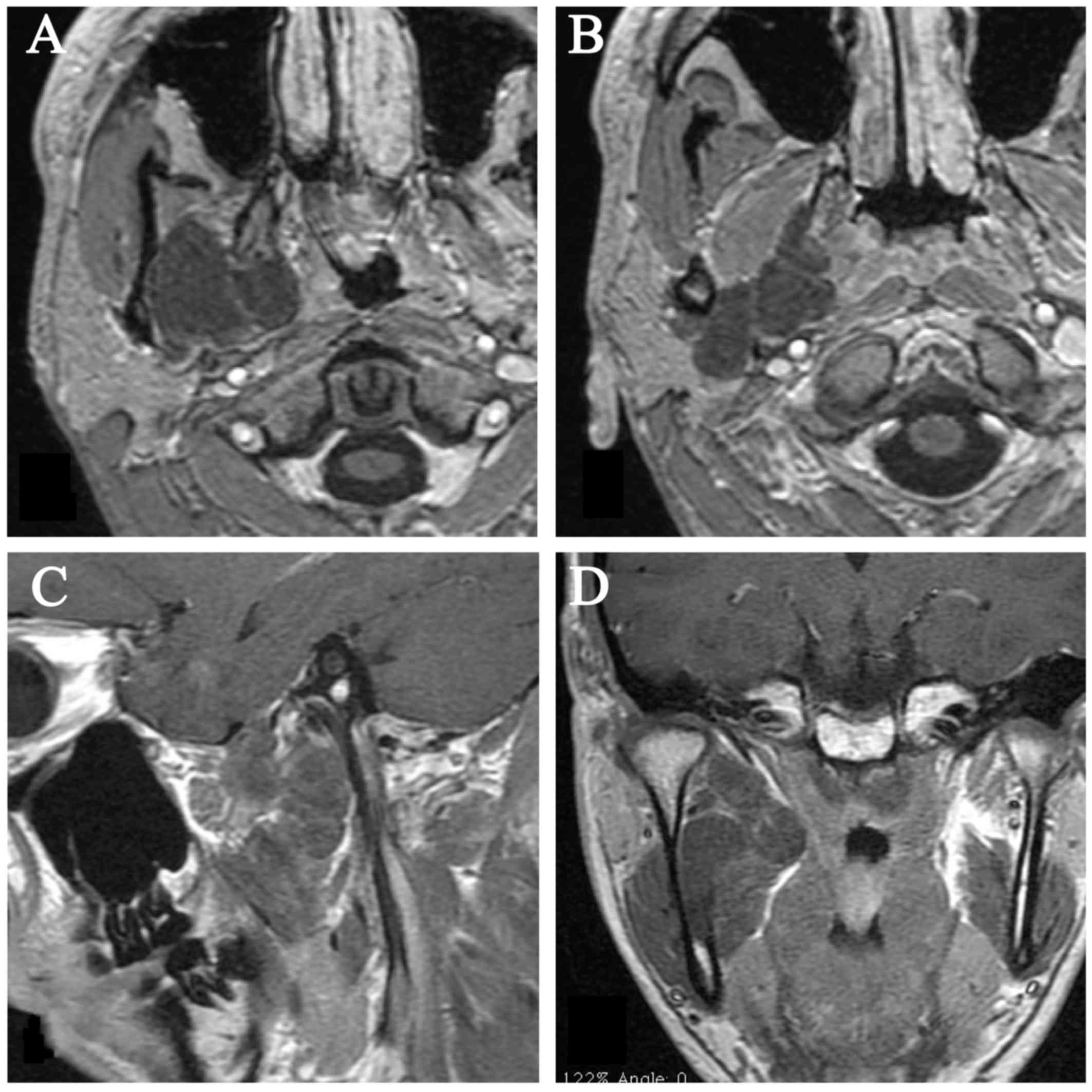
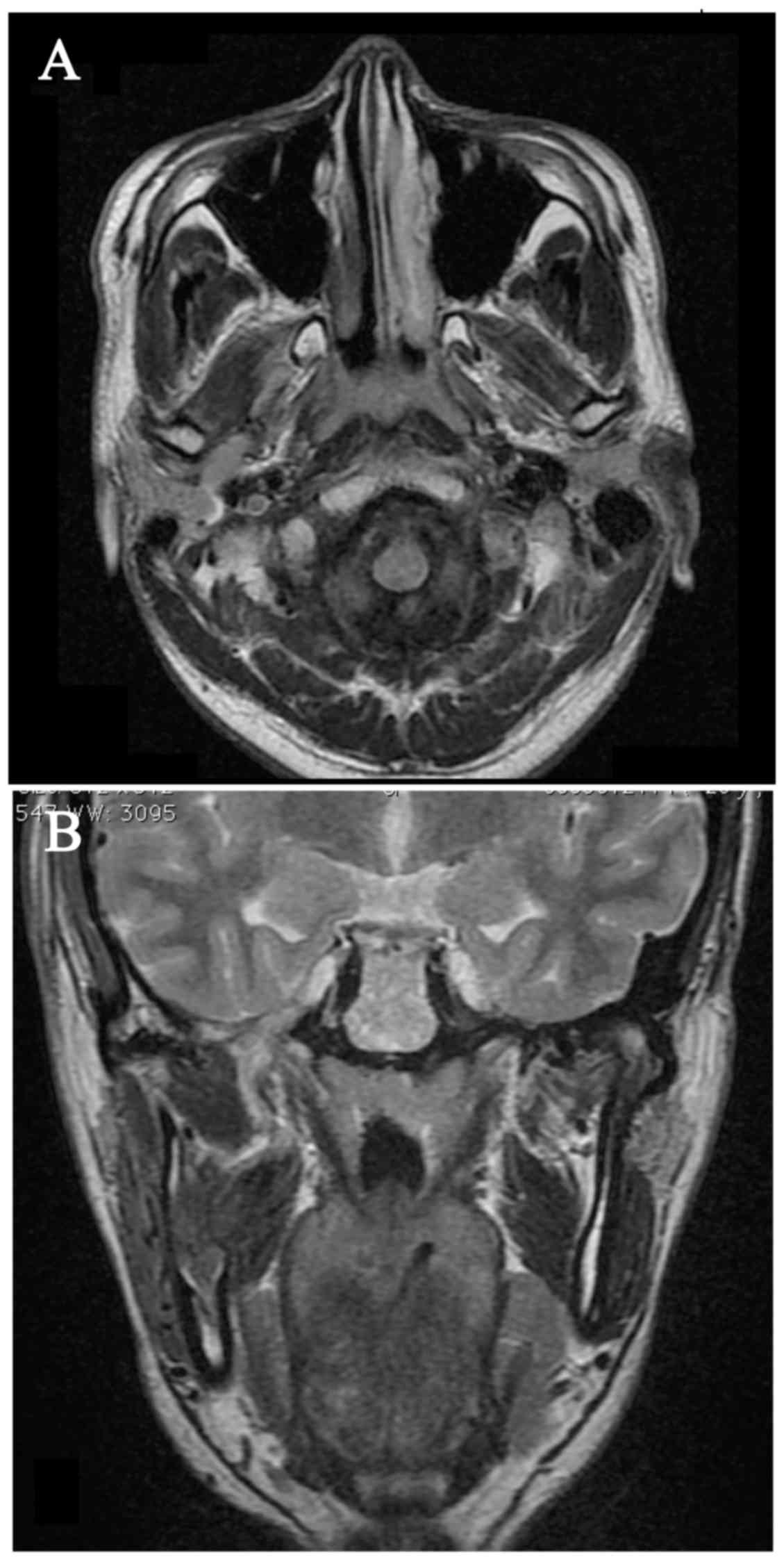
and D). A magnetic resonance imaging (MRI) scan revealed a
large mass in the ITF, extending from the intramandibular region to
the foramen ovale. The mass exhibited no enhancement following
administration of contrast medium (Fig.
2).
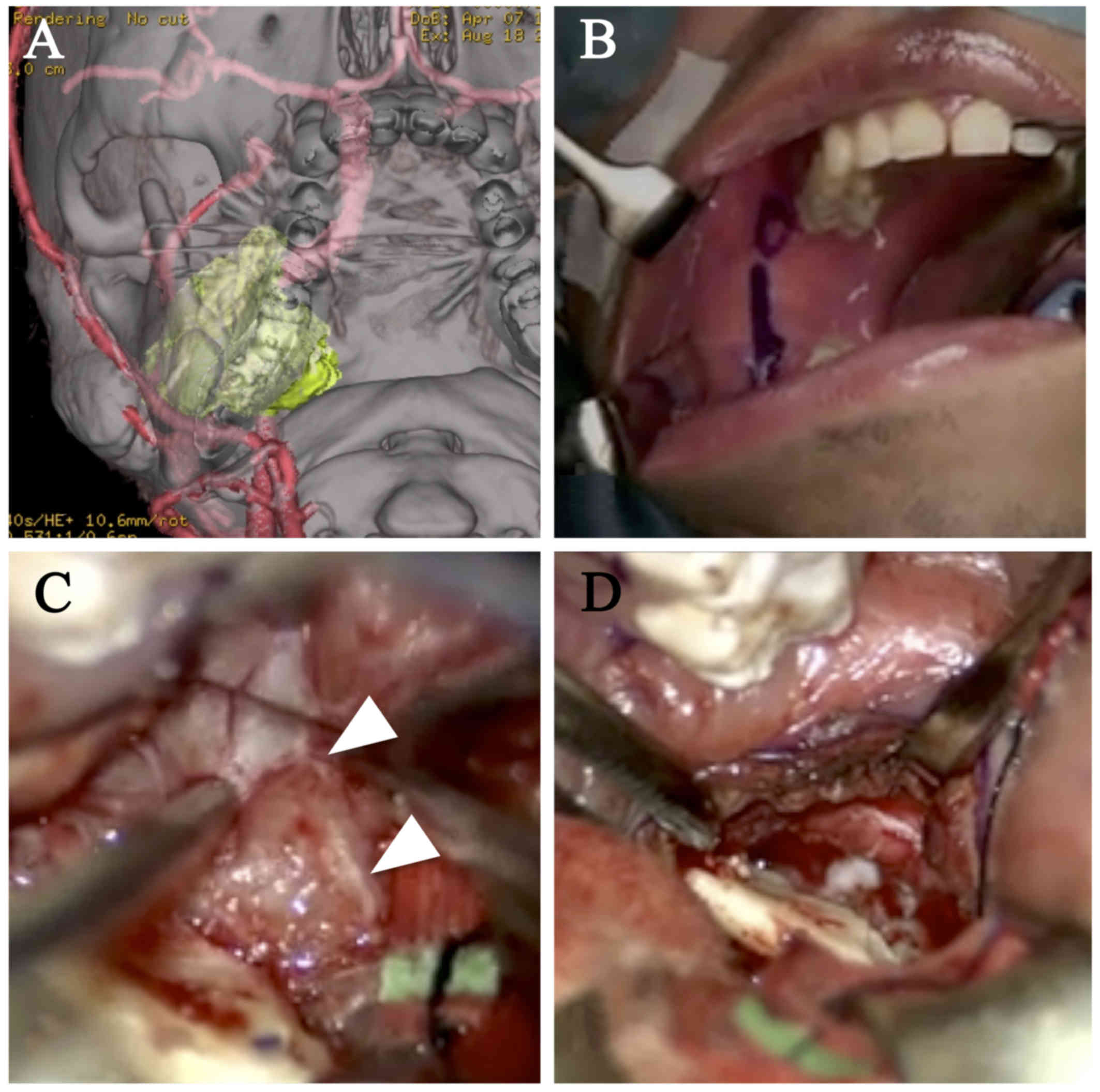
As the patient's symptoms progressed, a staged
surgical excision was considered. A transtemporal approach was
employed, which involved retraction of the temporal lobe
extradurally, followed by drilling around the foramen ovale.
Following removal of the upper third of the tumor, the remaining
tumor was removed via a transoral-retromolar approach (Fig. 3). The tumor was soft and fibrous,
without a capsule, which was consistent with the typical findings
of a neurofibroma. As the tumor had originated from the inferior
alveolar nerve, preservation of this nerve was not possible.
However, the lingual nerve, which was identified on the anterior
surface of the tumor, was completely preserved. Using Doppler
ultrasound and intraoperative navigation, the course of the
internal carotid artery was identified as running immediately
behind the tumor and then entering into the carotid canal.
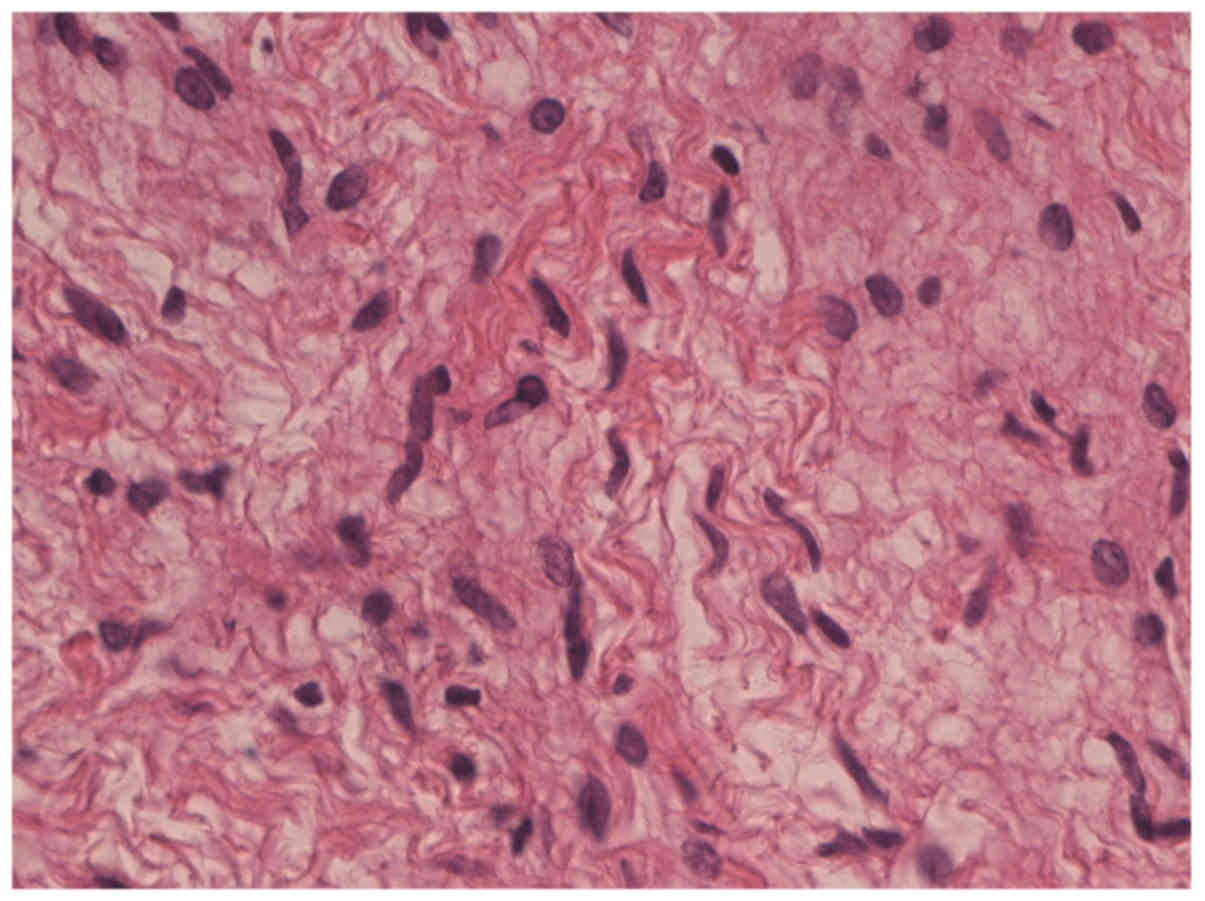
Histological examination revealed that the tumor
cells were situated in a loose, delicate and myxoid stroma, and had
wavy or serpiginous nuclei, suggesting a neurofibroma (Fig. 4). Immunohistochemical examination
revealed that the lesion contained numerous S-100 protein-positive
cells. Immunoreactivity for neurofilament protein was observed in
the scattered axons. There was no immunoreactivity for epithelial
membrane antigen. As the patient had no other neurofibromas, the
diagnosis was established as solitary neurofibroma of the inferior
alveolar nerve in the mandible.
The patient's neurological symptom did not subside;
the numbness of the right jaw, which was present prior to surgery,
persisted postoperatively. No recurrence was observed on an MRI
scan 12 months after the surgery (Fig.
5). The last follow-up visit was in June 2016. Written informed
consent was obtained from the patient regarding the publication of
this case report and associated images.
Discussion
Neurofibroma is a benign tumor that arises from
neurons and perineural cells (5). It
is most commonly associated with NF-1, as multiple tumors may arise
from peripheral nerves in NF-1 patients (1). On the contrary, solitary neurofibromas
arising from a division of the trigeminal nerve are rarely reported
(1–7). Neurofibromas arising from the inferior
alveolar nerve usually present with deformity of the jaw, due to
outgrowth of the mandible, as well as sensory disturbance of the
affected nerve (1–3). Ellis et al summarized
intraosseous benign neural sheath neoplasms of the jaw and
described the characteristics of neurofibromas and neurinomas in
this region (7). Solitary
neurofibromas are reported to be slow-growing tumors; however, an
unencapsulated neurofibroma has a greater probability of recurrence
compared with an encapsulated neurinoma. Therefore, surgical
resection plays an important role in the treatment of solitary
neurofibromas in this region.
The ITF is among the most challenging regions to
access (8,9,11,13). In
addition, in cases with significant tumor extension, more than one
approach may be required to remove the tumor. In the present case,
the tumor extended from the body of the mandible to the foramen
ovale, and was difficult to expose via a single approach. Thus, two
approaches were used: A transtemporal approach for the upper part
of the tumor, and a transoral-retromolar approach for the lower
part of the tumor. The transtemporal approach is a transcranial
extradural approach to the region (8) that provides a wide operative field
around the foramen ovale, where most divisions of the mandibular
nerve can be observed. However, the width of the operative field
depends on the area of the middle fossa that can be drilled away.
Furthermore, although extensive drilling of the middle fossa and
removal of the zygomatic arch provide easy access to the medial and
deeper areas of the ITF, exposing the lateral part of the ITF, just
inside the mandibular ramus, requires excessive retraction of the
temporal lobe. In addition, even with extensive posterior bone
drilling, the temporomandibular joint limits the posterior surgical
exposure around the carotid canal and styloid process. Therefore, a
transtemporal approach is not suitable for the removal of masses
located in the lateral and posterior parts of the ITF.
By contrast, the region difficult to reach via the
aforementioned transtemporal approach may be reached easily via a
transoral-retromolar approach (12,13). The
gingival incision of the oral mucosa may be performed in the
retromolar trigone, allowing direct exposure around the mandibular
ramus, where the inferior alveolar nerve enters into the mandibular
canal. Then, following the inferior alveolar nerve proximally,
dissection of the connective tissues between the medial and lateral
pterygoid muscles leads to the posterior trunk of the mandibular
nerve, from where the lingual nerve branches just below the lateral
pterygoid muscle. In contrast to the limitation of a surgical
corridor formed by the window of bone drilling in the transtemporal
approach, the entry from the oral mucosa allows flexible changes in
the direction of the surgeon's view. In the present case, the tumor
around the jugular foramen could not be reached via the
transtemporal approach, but was easily identified and removed via
the transoral-retromolar approach.
The transzygomatic-transmandibular approach is
another useful approach for accessing the ITF (9,10).
However, the facial nerve is at risk while dissecting around the
parotid gland to expose the lateral ramus of the mandible. In
addition, reconstruction of the mandible and temporomandibular
joint is a major concern following tumor removal. The use of the
transoral-retromolar approach is free from the risk of facial nerve
injury or the necessity for reconstruction of the mandible. In
addition, accessing the ITF and the subsequent closure are fast and
simple, as only the gingival incision is required to create the
corridor to the ITF (13). However,
the risk of infection may be relatively high compared with other
approaches due to the transoral route. Therefore, in cases
involving a tumor of the ITF extending intradurally in the middle
fossa, the transoral-retromolar approach must be applied following
careful consideration.
References
|
1
|
Apostolidis C, Anterriotis D, Rapidis AD
and Angelopoulos AP: Solitary intraosseous neurofibroma of the
inferior alveolar nerve: Report of a case. J Oral Maxillofac Surg.
59:232–235. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jangam SS, Ingole SN, Deshpande MD and
Ranadive PA: Solitary intraosseous neurofibroma: Report of a unique
case. Contemp Clin Dent. 5:561–563. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Polak M, Polak G, Brocheriou C and Vigneul
J: Solitary neurofibroma of the mandible: Case report and review of
the literature. J Oral Maxillofac Surg. 47:65–68. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
da Rosa MR, Ribeiro AL, de Menezes SA,
Pinheiro JJ and Alves-Junior SM: Solitary giant neurofibroma of the
mental nerve: A trauma-related lesion? J Craniofac Surg.
24:e247–e251. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wang HM, Hsu YC, Lee KW, Chiang FY and Kuo
WR: Neurofibroma of the lingual nerve: A case report. Kaohsiung J
Med Sci. 22:461–464. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cartellieri M and Swoboda H: Neurofibroma
of the auriculotemporal nerve. Eur Arch Otorhinolaryngol.
257:396–398. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ellis GL, Abrams AM and Melrose RJ:
Intraosseous benign neural sheath neoplasms of the jaws. Report of
seven new cases and review of the literature. Oral Surg Oral Med
Oral Pathol. 44:731–743. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Terasaka S, Sawamura Y, Goto S and
Fukushima T: A lateral transzygomatic-transtemporal approach to the
infratemporal fossa: Technical note for mobilization of the second
and third branches of the trigeminal nerve. Skull Base Surg.
9:277–287. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Timoshenko AP, Asanau A, Gavid M, Colin V,
Martin C and Prades JM: Preauricular transmandibular and
transzygomatic approach for tumors of the infratemporal fossa
revisited. ORL J Otorhinolaryngol Relat Spec. 75:250–255. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chatni SS, Sharan R, Patel D, Iyer S,
Tiwari RM and Kuriakose MA: Transmandibular approach for excision
of maxillary sinus tumors extending to pterygopalatine and
infratemporal fossae. Oral Oncol. 45:720–726. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liu JK, Sameshima T, Gottfried ON,
Couldwell WT and Fukushima T: The combined transmastoid retro- and
infralabyrinthine transjugular transcondylar transtubercular high
cervical approach for resection of glomus jugulare tumors.
Neurosurgery. 59 1 Suppl 1:ONS115–125. 2006.PubMed/NCBI
|
|
12
|
Cobzeanu BM, Popescu E, Costan VV,
Ungureanu D and Cobzeanu MD: Retromolar trigone-oropharynx junction
maligns tumor surgery: Transmandibular versus oral approach. Rev
Med Chir Soc Med Nat Iasi. 119:119–126. 2015.PubMed/NCBI
|
|
13
|
Scheller K, Eckert AW and Scheller C:
Transoral, retromolar, para-tonsillar approach to the styloid
process in 6 patients with Eagle's syndrome. Med Oral Patol Oral
Cir Bucal. 19:e61–e66. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
El-Sayed I, Pletcher S, Russell M,
McDermott M and Parsa A: Endoscopic anterior maxillotomy:
Infratemporal fossa via transnasal approach. Laryngoscope.
121:694–698. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Carrau RL, Prevedello DM, de Lara D,
Durmus K and Ozer E: Combined transoral robotic surgery and
endoscopic endonasal approach for the resection of extensive
malignancies of the skull base. Head Neck. 35:E351–E358. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Satar B, Yazar F, Ceyhan A, Arslan HH and
Aydin S: Analysis of jugular foramen exposure in the fallopian
bridge technique. Skull Base. 19:203–207. 2009. View Article : Google Scholar : PubMed/NCBI
|