Introduction
Hepatocellular carcinoma (HCC) is the sixth most
prevalent cancer and the second most frequent cause of
cancer-associated mortality worldwide, with nearly 780,000 new
cases diagnosed annually (1,2). The prognosis of HCC has been improved
due to the availability of curative options, such as liver
transplantation, hepatic resection and radiofrequency ablation used
at an early stage. However, due to its high metastatic potential,
more than half of HCC patients develop recurrence or distant
metastasis within 5 years post-surgery. Transcatheter arterial
chemoembolization (TACE) is the major treatment method for
intermediate-stage HCC; however, treatment-refractory disease or
metastasis can lead to TACE failure (3,4).
Therefore, systemic therapies, such as sorafenib, are applied as
alternative treatment options.
Sorafenib is an oral, multi-target and multi-kinase
inhibitor, and is used to treat HCC through blocking
mitogen-activated protein kinase signaling and through inhibiting
vascular endothelial growth factor (VEGF) receptor and
platelet-derived growth factor receptor to produce anti-angiogenic
effects (5,6). Currently, it is the only molecular
targeted drug that exerts a clear survival benefit and has been
approved by the Food & Drug Administration for advanced HCC
(7); it is regarded as a first-line
therapy according to the 2008 National Comprehensive Cancer Network
guidelines (8). In the SHARP study,
the median overall survival (OS) times were 10.7 months in the
sorafenib group and 7.9 months in the placebo group (P<0.001);
and the median times to radiological progression were 5.5 months in
the sorafenib group and 2.8 months in the placebo group
(P<0.001) (9). The phase III
Sorafenib Asia-Pacific trial, restricted to an eastern population,
also showed that sorafenib could significantly prolong the median
OS time from 4.2 to 6.5 months compared with placebo group
(10). However, the objective
response rates (ORRs) in these two trials were 2 and 3.3%,
suggesting that the efficacy of sorafenib remained limited. A
propensity score analysis indicated that initial half-dose
sorafenib treatment led to fewer severe adverse effects and a
comparable survival benefit compared with a full dose in patients
of advanced age (median, 75 years) with HCC (11). In addition, another study indicated
that skin toxicity should be closely monitored in HCC patients
treated with sorafenib, due to its association with sorafenib
efficacy (12).
To date, the innate mechanisms of tumor pathogenesis
and progression remains unclear. However, several studies have
indicated that tumor pathogenesis and progression are closely
associated with the tumor microenvironment, as well as tumor cells
themselves (13). Recent studies
have suggested that a systemic inflammatory state is associated
with the malignant biological behavior of the tumor (14,15). In
particular, the neutrophil-lymphocyte ratio (NLR) has been
evaluated as a predictor of prognosis in various types of solid
tumor, including gastric, colorectal, pancreatic, breast and lung
cancers (16–19). An elevated NLR has already been shown
to be associated with poor prognosis in patients with HCC treated
by liver transplantation, surgical resection, or TACE (20–22). The
present study evaluated the association between peripheral blood
neutrophil count and the prognosis of HCC treated with sorafenib,
and revealed peripheral neutrophil count as a prognostic factor in
such cases.
Materials and methods
Patients
A total of 464 patients with HCC and who were
treated with sorafenib at the Department of Hepatic Oncology of
Zhongshan Hospital affiliated to Fudan University (Shanghai, China)
between January 1st, 2008 and December 31st, 2012, were initially
included in the present study. The study was retrospective and
non-interventional. At the time the patients were enrolled, the
majority of them had passed away due to disease progression.
Therefore, the requirement for informed consent was waived, and the
study protocol was approved by the Ethics Committee of Zhongshan
Hospital, Fudan University. The study conformed to the principles
of the Declaration of Helsinki.
The inclusion criteria were as follows: i) Diagnosis
of HCC based on pathology or non-invasive diagnostic criteria [such
as liver cirrhosis; evidence of chronic hepatitis B virus
(HBV)/hepatitis C virus infection; or dynamic computed tomography
(CT) or magnetic resonance imaging (MRI) with intense
contrast-uptake during the arterial phase followed by contrast
washout during the venous or delayed phases]; and ii) patients
received sorafenib therapy continually for ≥3 months. The following
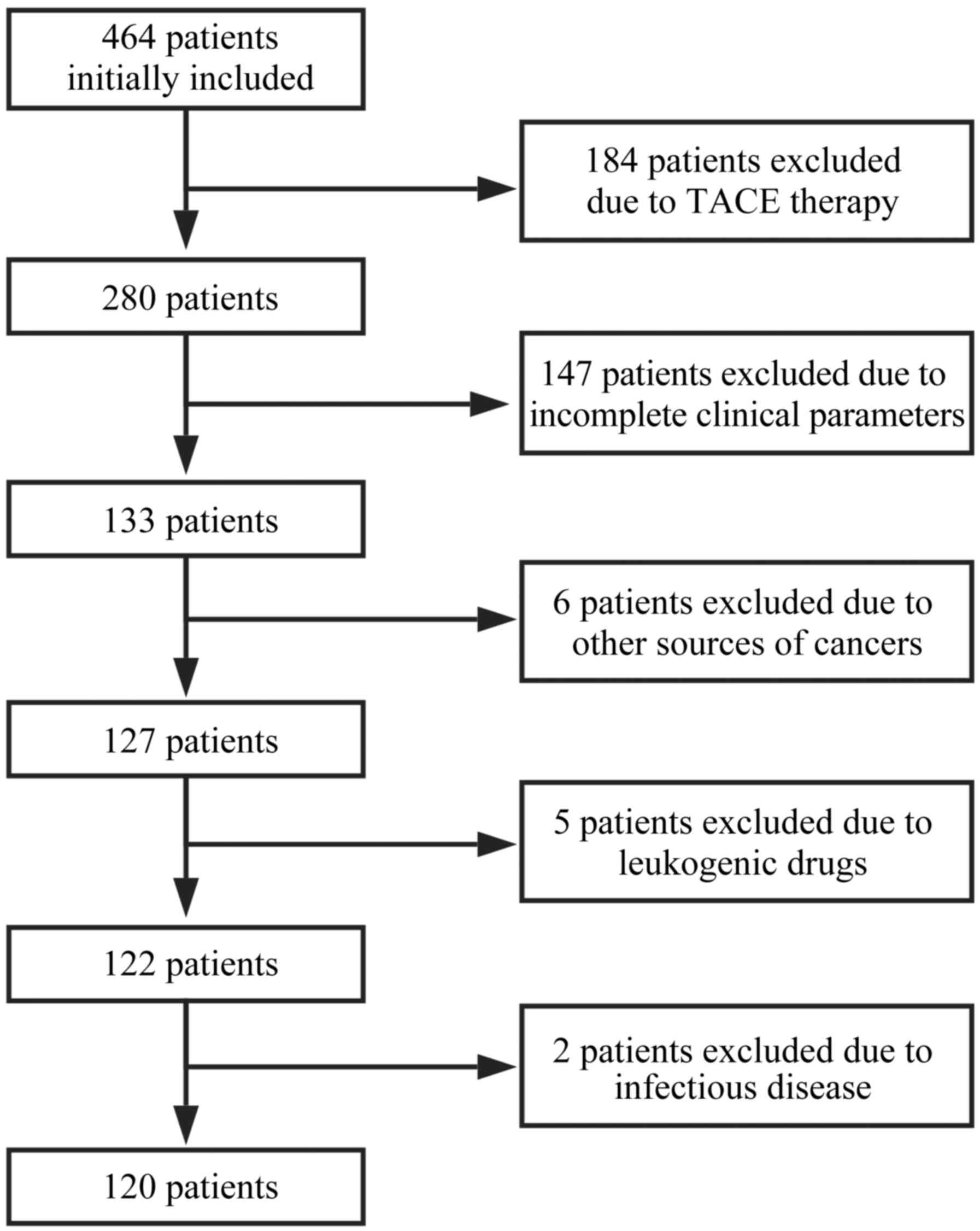
exclusion criteria were applied: i) treatment combination included
TACE therapy following sorafenib; ii) incomplete clinical
parameters were available, affecting outcome analysis; iii) other
concurrent cancers were present; iv) leukogenic drug treatment had
been taken within 1 week prior to blood collection; v) concurrent
infectious diseases were present. Finally, 120 patients were
enrolled in the present study, as illustrated in the enrollment
flowchart (Fig. 1). The
characteristics of these 120 patients are presented in Table I.
 | Table I.Baseline demographic and clinical
characteristics of the patients (n=120). |
Table I.
Baseline demographic and clinical
characteristics of the patients (n=120).
| Variable | n (%) | Average (range) |
|---|
| Age (years) |
| 52.5
(21–78)a |
| ≤60 | 87 (72.5) |
|
|
>60 | 33 (27.5) |
|
| Sex |
| – |
| Male | 105 (87.5) |
|
|
Female | 15 (12.5) |
|
| HBsAg status |
| – |
|
Positive | 83 (72.2) |
|
|
Negative | 32 (23.4) |
|
| HBV DNA status |
| – |
|
Positive | 39 (40.6) |
|
|
Negative | 57 (59.4) |
|
| Neutrophil count
(×109/l) |
| 3.34±1.73
(0.7–9.1)b |
| ≤3.3 | 75 (62.5) |
|
|
>3.3 | 45 (37.5) |
|
| Lymphocyte count
(×109/l) |
| 1.12±0.51
(0.2–2.6)b |
| ≤1.1 | 68 (56.7) |
|
|
>1.1 | 52 (43.3) |
|
| Platelet count
(×109/l) |
| 121.73±72.47 |
|
|
|
(23.0–347.0)b |
|
<125 | 77 (64.2) |
|
|
≥125 | 43 (35.8) |
|
| Child-Pugh
class |
| – |
| A | 98 (89.9) |
|
| B | 11 (10.1) |
|
| α-fetoprotein level
(ng/ml) |
|
10,490.31±19,851.40 |
|
|
|
(1.2–60,500.0)b |
|
≤20 | 28 (23.3) |
|
|
>20 | 87 (72.5) |
|
| Tumor number |
| – |
|
<3 | 52 (47.7) |
|
| ≥3 | 57 (52.3) |
|
| Tumor size
(cm) |
| 42.66±38.99 |
|
|
| (0.0–173.0)b |
| ≤5 | 64 (62.7) |
|
|
>5 | 38 (37.3) |
|
| Thrombus |
| – |
|
Yes | 30 (25.0) |
|
| No | 90 (75.0) |
|
| Metastasis |
| – |
|
Yes | 63 (52.5) |
|
| No | 57 (47.5) |
|
| BCLC stage |
| – |
| B | 41 (34.2) |
|
| C | 79 (65.8) |
|
Sorafenib treatment
The initial sorafenib oral dose was 400 mg twice
daily. Among patients with liver dysfunction of Child-Pugh class B,
sorafenib could be initiated at a reduced starting dose of 400 mg
once daily, with subsequent dose-escalation according to tolerance.
For patients receiving full-dose sorafenib, intake could also be
adjusted for the management of adverse events, depending on their
type and severity according to the NCI Common Terminology Criteria
for Adverse Events (CTCAE) v3.0 (23).
Follow-up and assessment
All patients were followed up every month, which
included a routine blood examination, liver function tests and
analysis of α-fetoprotein (AFP) levels. Response was evaluated by
CT or MRI at intervals of 2–3 months. All patients were followed up
until December 31st, 2015.
The primary endpoint of the study was OS, which was
defined as the time between the commencement of sorafenib therapy
and either the date of mortality due to any cause or the last
observation date of surviving patients. The secondary endpoint was
disease-control rate (DCR), which was defined as the percentage of
patients who had a best-response rating of complete response,
partial response, or stable disease [according to the Response
Evaluation Criteria in Solid Tumors (RECIST) 1.1] (24).
Statistical analysis
Data were evaluated using SPSS software, version
21.0 (IBM Corp., Armonk, NY, USA). Continuous variables were
expressed as the mean ± standard deviation and ranges
(minimum-maximum), and were compared using an unpaired Student's
t-test, Welch's t-test, or Mann-Whitney rank sum test, according to
the normality and homogeneity. Categorical variables were expressed
as the frequency and compared using a χ2 test. The
optimal cutoff point for neutrophil count was obtained from a
receiver operating characteristic (ROC) curve. The Kaplan-Meier
method was used to evaluate OS and to carry out the univariate
analysis, and the differences between groups were analyzed with a
log-rank test. The independent prognostic value of each factor was
explored by multivariate analysis according to a Cox proportional
hazards model. P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics
The median age of the 120 enrolled patients was 52.5
years (range, 21–78 years). The majority of the patients were male
(n=105; 87.5%). HBV surface antigen (HBsAg) was positive in 83
patients (72.2%). Well-preserved liver function (Child-Pugh class
A) was found in 98 patients (89.9%). Elevated AFP levels (>20
ng/ml) were detected in 87 patients (72.5%). There were 57 patients
(52.3%) who had ≥3 tumors. Tumors measuring >5 cm in longest
diameter were found in 38 patients (37.3%). Extrahepatic spread was
found in 63 patients (52.5%), and vascular invasion in 30 patients
(25.0%). Barcelona Clinic Liver Cancer (BCLC) stage C was found in
79 patients (65.8%). The detailed characteristics of the patients
are shown in Table I.
OS and objective response
The patients were followed until December 31st,
2015. The median follow-up time was 8.5 months (range, 1.0–80.5
months). At the time of recording of the data, 92 mortalities
(76.7%) had occurred. The median OS time for the entire cohort was
9.0 months [95% confidence interval (CI), 5.9–12.1 months], and the
1-, 2- and 3-year OS rates were 36, 24, and 16%, respectively.
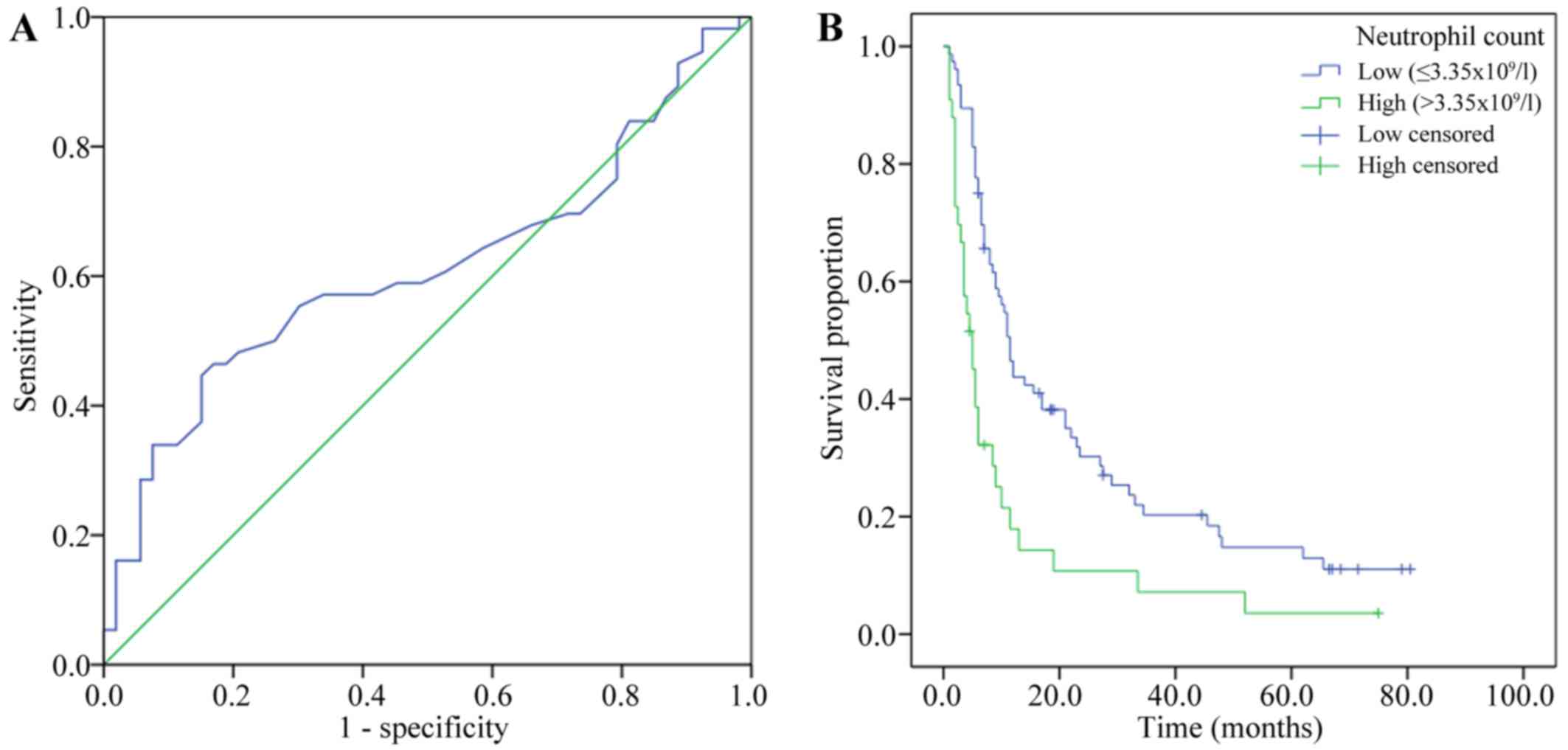
The baseline neutrophil count was measured within 1
week prior to sorafenib treatment. The mean baseline level of
neutrophils was 3.34×109/l, with a range of
0.7–9.1×109/l. Using an ROC curve, the optimal cutoff
point for absolute neutrophil count (3.65×109/l) was
determined according to the median OS time. The area under the
curve was 0.612 (95% CI, 0.504–0.720; P=0.044). The sensitivity and
specificity were 0.446, and 0.849, respectively (Fig. 2A).
According to the cutoff point for neutrophil count
determined from the ROC curve, the patients were divided into two
groups: A low-neutrophil group (count, <3.65×109/l;
n=81) and a high-neutrophil group (count, ≥3.65×109/l;
n=39). The median OS time of the low-neutrophil group was 11.5
months (95% CI, 9.7–13.3 months), compared with 5.0 months (95% CI,
3.2–6.8 months) for patients in the high-neutrophil group
(P<0.001; Fig. 2B). In the
low-neutrophil group, 2 patients (2.5%) had a partial response and
34 (42.0%) had stable disease (according to RECIST), whereas in the
high-neutrophil group, no patients (0%) had a partial response and
8 (20.5%) had stable disease. There were no complete responses in
either group. The DCR was significantly higher in the
low-neutrophil group than in the high-neutrophil group (44.4 vs.
20.5%; P=0.011; Table II).
| Table II.Objective response of patients
grouped according to low or high peripheral neutrophil counts. |
Table II.
Objective response of patients
grouped according to low or high peripheral neutrophil counts.
|
|
| Peripheral
neutrophils |
|
|---|
|
|
|
|
|
|---|
| Outcome | Overall | Low (n=81) | High (n=39) | P-value |
|---|
| Level of response,
n (%) |
|
|
|
|
| CR | 0 (0.0) | 0 (0.0) | 0 (0.0) | NA |
| PR | 2 (1.7) | 2 (2.5) | 0 (0.0) | 0.322 |
| SD | 42 (35.0) | 34 (42.0) | 8 (20.5) | 0.021a |
| PD | 44 (36.7) | 26 (32.1) | 18 (46.2) | 0.135 |
| NA | 32 (26.7) | 19 (23.5) | 13 (33.3) | 0.252 |
| Disease-control
rate, % | 36.7 | 44.4 | 20.5 | 0.011a |
Univariate and multivariate analyses
of prognostic factors
The potential prognostic factors were evaluated to
identify any significant associations with the OS of the patients.
As is shown in the Table III, the
significant prognostic factors were revealed as HBsAg (P=0.037),
neutrophil count (P<0.001), AFP level (P<0.001), tumor number
(P=0.001), tumor size (P<0.001), tumor thrombus (P=0.005),
extrahepatic metastasis (P=0.030) and BCLC stage (P=0.005). All the
statistically significant prognostic factors in the univariate
analysis were included in the multivariate analysis, except BCLC
stage (which is evaluated by tumor size, tumor number, tumor
thrombus and metastasis). The multivariate analysis identified that
a high baseline neutrophil count was an independent prognostic
factor associated with OS (P=0.023, HR=1.796), in addition to AFP
level (P=0.004) and tumor size (P=0.006) (Table III).
| Table III.Univariate and multivariate analyses
of factors in association with overall survival. |
Table III.
Univariate and multivariate analyses
of factors in association with overall survival.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variable | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age (≤60 vs. >60
years) | 1.093
(0.697–1.714) | 0.693 | – | – |
| Sex (male vs.
female) | 1.433
(0.803–2.556) | 0.212 | – | – |
| HBsAg status
(negative vs. positive) | 1.656
(1.018–2.694) | 0.037a | 0.914
(0.502–1.662) | 0.767 |
| HBV DNA status
(negative vs. positive) | 1.306
(0.819–2.085) | 0.254 | – | – |
| Neutrophil count
(≤3.65×109 vs. >3.65×109/l) | 2.212
(1.422–3.442) |
<0.001a | 1.796
(1.085–2.973) | 0.023a |
| Lymphocyte count
(≤1.1×109 vs. >1.1×109/l) | 0.816
(0.607–1.450) | 0.335 | – | – |
| Platelet count
(≥125×109 vs. <125×109/l) | 0.845
(0.543–1.315) | 0.447 | – | – |
| Child-Pugh class (A
vs. B) | 1.784
(0.912–3.491) | 0.081 | – | – |
| α-fetoprotein level
(≤20 vs. >20 ng/ml) | 3.288
(1.875–5.763) |
<0.001a | 2.582
(1.358–4.910) | 0.004a |
| Tumor number (<3
vs. ≥3) | 2.116
(1.342–3.338) | 0.001a | 1.351
(0.820–2.224) | 0.238 |
| Tumor size (≤5 vs.
>5 cm) | 2.805
(1.716–4.584) | <0.001a | 2.387
(1.288–4.426) | 0.006a |
| Thrombus (yes vs.
no) | 1.950
(1.203–3.162) | 0.005a | 1.021
(0.537–1.941) | 0.950 |
| Metastasis (yes vs.
no) | 1.578
(1.036–2.404) | 0.030a | 1.222
(0.761–1.963) | 0.406 |
| BCLC stage (B vs.
C) | 1.880
(1.190–2.969) | 0.005a | – | – |
Prognostic nomogram for OS
To predict the 1-year survival and 3-year survival
rates for HCC patients treated with sorafenib, a nomogram model
that integrated all significant independent factors for OS was
produced according to the multivariate Cox regression model
(Fig. 3). The Harrell's ç-index for
OS prediction was 0.79.
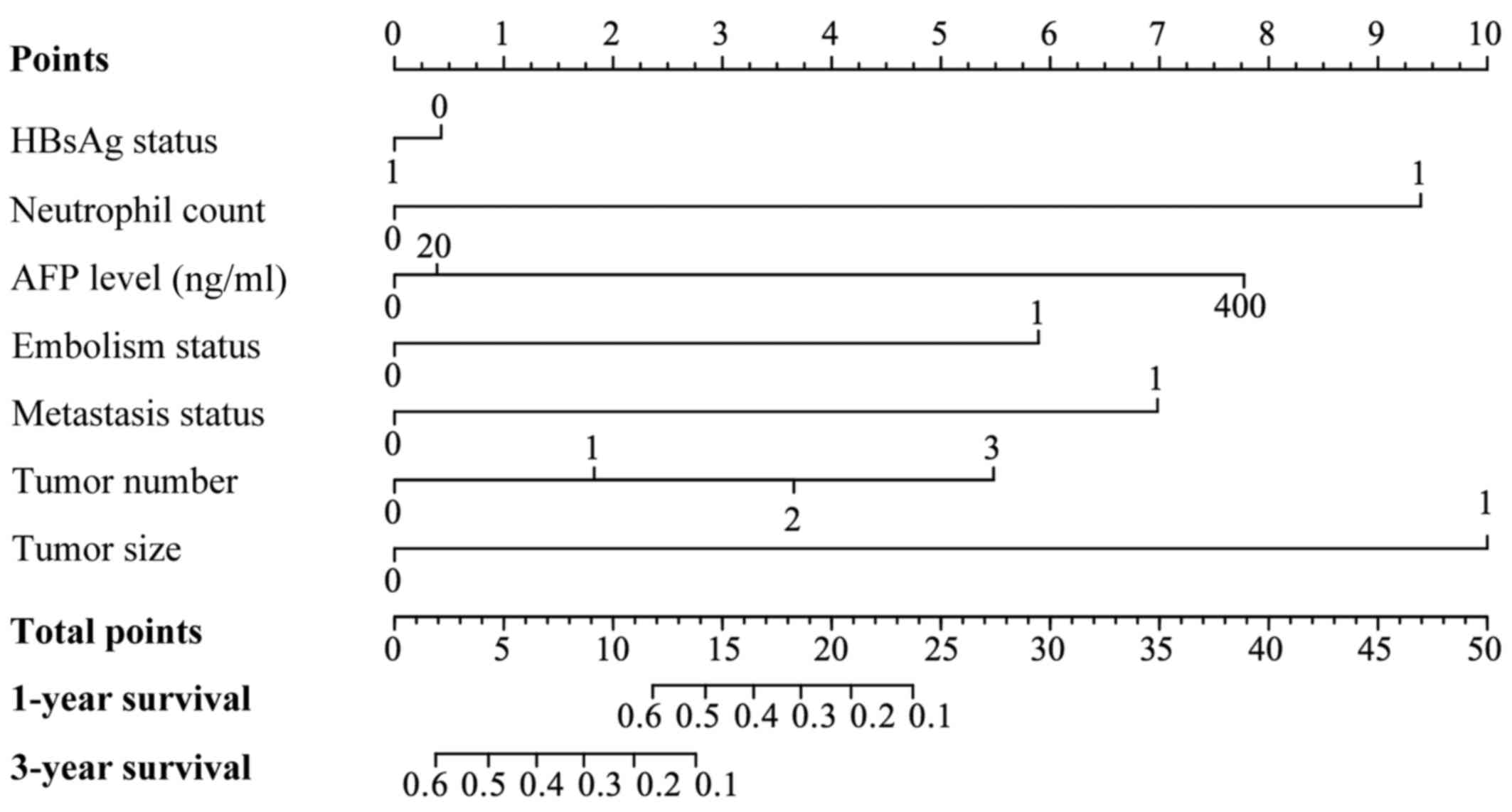 | Figure 3.A nomogram predicts the probability of
OS based on neutrophil and other prognostic factors in HCC patients
treated with sorafenib. To use the nomogram, an individual
patient's value is located on each variable axis, and a line is
drawn upward to determine the number of points received for each
variable value. The sum of these numbers is then located on the
‘Total points’ axis, and a line is drawn downward to the survival
axes to determine the likelihood of survival at 1 or 3 years. The
Harrell's c-index for OS prediction was 0.79. For variables
displayed as binary, 0 and 1 correspond to the following values:
HBsAg, negative=0, positive=1; neutrophil count,
≤3.65×109/l=0, >3.65×109/l=1; thrombus,
no=0, yes=1; metastasis, negative=0, positive=1; tumor size, ≤5
cm=0, >5 cm=1. OS, overall survival. |
Discussion
Currently, sorafenib is the only molecular targeted
drug to provide a clear survival benefit for patients with advanced
HCC; it has been shown to prolong the OS time of these patients for
~3 months (9). A numbers of studies
have proven its safety and effectiveness (25). Although the appearance of sorafenib
brings hope to patients with advanced HCC, the ORR of sorafenib
remains low due to tumor heterogeneity. Therefore, it is important
to identify the best prognostic factors that can predict response
to sorafenib. Certain studies showed that serum VEGF concentration
and extracellular signal-regulated kinase levels were good
predictors (26,27); however, other surrogate biomarkers
must be explored to evaluate prognosis or the efficacy of treatment
with sorafenib HCC.
In the present study, the patients were restricted
to those with BCLC stage C or BCLC stage B but who had previously
experienced TACE failure, for whom sorafenib is the major treatment
method (28). Routine blood tests
are a conventional examination for patients, and neutrophil counts
are commonly used to evaluate a patient's inflammatory state in
clinical practice. Tumor neutrophil infiltration has also been
found to be associated with the promotion of inflammation,
contributing to tumor progression (29). Therefore, we hypothesized that the
peripheral neutrophil count could be a biomarker indicative of the
tumor inflammatory microenvironment in HCC and the efficacy of
sorafenib treatment. The median OS time of the low-neutrophil group
was significantly increased compared with that of the
high-neutrophil group (11.5 vs. 5.0 months). In addition, the DCR
was significantly higher in the low-neutrophil group than in the
high-neutrophil group (44.5 vs. 20.5%). Univariate and multivariate
analyses revealed that neutrophil level is an independent
prognostic factor for OS. In addition, peripheral neutrophil count
was associated with platelet count as they were components of the
same hematopoietic system. Furthermore, peripheral neutrophil count
was associated with AFP level and tumor size (data not shown),
suggesting the following possible mechanism: Increased neutrophil
levels alter the tumor microenvironment, and the formation of the
inflammatory microenvironment affects the sensitivity of HCC to
sorafenib treatment, thus promoting tumor growth, resulting in
elevated AFP concentration.
In similar studies, researchers have investigated
the use of NLR as a prognostic factor. Motomura et al
(30) found there was a correlation
between elevated NLR and upregulated interleukin (IL)-17
concentration in serum and peritumoral regions. IL-17 is a
proinflammatory cytokine that promotes HCC growth (31). In our preliminary data analysis,
neutrophil count was found to have a significant association with
OS, whereas lymphocyte count did not. In addition, NLR was
associated with survival, but was not as significant as the
neutrophil count (data not shown). Therefore, in the present
research, the absolute neutrophil count was used as a predictor.
Furthermore, studies have shown that neutrophils are associated
with the systemic release of growth factors and proteolytic
enzymes, such as VEGF and matrix metalloproteinase-9, which promote
tumor invasion, metastasis and angiogenesis (32,33).
In present study, a nomogram model was created to
predict the survival rate based on neutrophil count and other
prognostic factors. We suggest that this model may be a simple and
easy tool for estimating the survival probability of patients with
HCC. The Harrell's c-index was 0.79 for this model, indicating that
this model was basically consistent with the actual conditions.
Although the present study has revealed a
relationship between peripheral neutrophil count and the efficacy
of sorafenib treatment, the underlying mechanisms require further
exploration. As a retrospective study, there are certain
limitations, such as the presence of possible bias, and further
prospective randomized controlled trials are encouraged to evaluate
the predictive role of peripheral neutrophils in the efficacy of
sorafenib treatment for HCC.
References
|
1
|
Bruix J, Gores GJ and Mazzaferro V:
Hepatocellular carcinoma: Clinical frontiers and perspectives. Gut.
63:844–855. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Abdel-Rahman O: Systemic therapy for
hepatocellular carcinoma (HCC): From bench to bedside. J Egypt Natl
Canc Inst. 25:165–171. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Llovet JM and Bruix J: Novel advancements
in the management of hepatocellular carcinoma in 2008. J Hepatol.
48 Suppl 1:S20–S37. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Llovet JM, Burroughs A and Bruix J:
Hepatocellular carcinoma. Lancet. 362:1907–1917. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chen W, Wu J, Shi H, Wang Z, Zhang G, Cao
Y, Jiang C and Ding Y: Hepatic stellate cell coculture enables
sorafenib resistance in Huh7 cells through HGF/c-Met/Akt and
Jak2/Stat3 pathways. Biomed Res Int. 2014:7649812014.PubMed/NCBI
|
|
6
|
Moeini A, Cornellà H and Villanueva A:
Emerging signaling pathways in hepatocellular carcinoma. Liver
Cancer. 1:83–93. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Huang WS and Yang CH: Sorafenib induced
tumor lysis syndrome in an advanced hepatocellular carcinoma
patient. World J Gastroenterol. 15:4464–4466. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
National Comprehensive Cancer Network, .
(NCCN) Clinical Practice Guidelines in Oncology. Hepatobiliary
Cancers. 2008 https://www.nccn.org/professionals/physician_gls/f_guidelines.aspAccessed.
8–Feb;2008.
|
|
9
|
Llovet JM, Ricci S, Mazzaferro V, Hilgard
P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A,
et al: Sorafenib in advanced hepatocellular carcinoma. N Engl J
Med. 359:378–390. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cheng AL, Guan Z, Chen Z, Tsao CJ, Qin S,
Kim JS, Yang TS, Tak WY, Pan H, Yu S, et al: Efficacy and safety of
sorafenib in patients with advanced hepatocellular carcinoma
according to baseline status: Subset analyses of the phase III
Sorafenib Asia-Pacific trial. Eur J Cancer. 48:1452–1465. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Morimoto M, Numata K, Kondo M, Kobayashi
S, Ohkawa S, Hidaka H, Nakazawa T, Okuwaki Y, Okuse C, Matsunaga K,
et al: Field practice study of half-dose sorafenib treatment on
safety and efficacy for hepatocellular carcinoma: A propensity
score analysis. Hepatol Res. 45:279–287. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Vincenzi B, Santini D, Russo A, Addeo R,
Giuliani F, Montella L, Rizzo S, Venditti O, Frezza AM, Caraglia M,
et al: Early skin toxicity as a predictive factor for tumor control
in hepatocellular carcinoma patients treated with sorafenib.
Oncologist. 15:85–92. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mbeunkui F and Johann DJ Jr: Cancer and
the tumor microenvironment: A review of an essential relationship.
Cancer Chemother Pharmacol. 63:571–582. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Li C, Deng M, Hu J, Li X, Chen L, Ju Y,
Hao J and Meng S: Chronic inflammation contributes to the
development of hepatocellular carcinoma by decreasing miR-122
levels. Oncotarget. 7:17021–17034. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chang TS, Chen CL, Wu YC, Liu JJ, Kuo YC,
Lee KF, Lin SY, Lin SE, Tung SY, Kuo LM, et al: Inflammation
promotes expression of stemness-related properties in HBV-related
hepatocellular carcinoma. PLoS One. 11:e1498972016.
|
|
16
|
Wang F, Liu ZY, Xia YY, Zhou C, Shen XM,
Li XL, Han SG, Zheng Y, Mao ZQ, Gong FR, et al: Changes in
neutrophil/lymphocyte and platelet/lymphocyte ratios after
chemotherapy correlate with chemotherapy response and prediction of
prognosis in patients with unresectable gastric cancer. Oncol Lett.
10:3411–3418. 2015.PubMed/NCBI
|
|
17
|
Pine JK, Morris E, Hutchins GG, West NP,
Jayne DG, Quirke P and Prasad KR: Systemic neutrophil-to-lymphocyte
ratio in colorectal cancer: The relationship to patient survival,
tumour biology and local lymphocytic response to tumour. Br J
Cancer. 113:204–211. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Szkandera J, Stotz M, Eisner F, Absenger
G, Stojakovic T, Samonigg H, Kornprat P, Schaberl-Moser R,
Alzoughbi W, Ress AL, et al: External validation of the derived
neutrophil to lymphocyte ratio as a prognostic marker on a large
cohort of pancreatic cancer patients. PLoS One. 8:e782252013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shao N and Cai Q: High pretreatment
neutrophil-lymphocyte ratio predicts recurrence and poor prognosis
for combined small cell lung cancer. Clin Transl Oncol. 17:772–778.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Xiao GQ, Liu C, Liu DL, Yang JY and Yan
LN: Neutrophil-lymphocyte ratio predicts the prognosis of patients
with hepatocellular carcinoma after liver transplantation. World J
Gastroenterol. 19:8398–8407. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Okamura Y, Ashida R, Ito T, Sugiura T,
Mori K and Uesaka K: Preoperative neutrophil to lymphocyte ratio
and prognostic nutritional index predict overall survival after
hepatectomy for hepatocellular carcinoma. World J Surg.
39:1501–1509. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Fan W, Zhang Y, Wang Y, Yao X, Yang J and
Li J: Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as
predictors of survival and metastasis for recurrent hepatocellular
carcinoma after transarterial chemoembolization. PLoS One.
10:e1193122015.
|
|
23
|
Trotti A, Colevas AD, Setser A, Rusch V,
Jaques D, Budach V, Langer C, Murphy B, Cumberlin R, Coleman CN and
Rubin P: CTCAE v3.0: Development of a comprehensive grading system
for the adverse effects of cancer treatment. Semin Radiat Oncol.
133:176–181. 2003. View Article : Google Scholar
|
|
24
|
Therasse P, Arbuck SG, Eisenhauer EA,
Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van
Oosterom AT, Christian MC and Gwyther SG: New guidelines to
evaluate the response to treatment in solid tumors. European
Organization for Research and Treatment of Cancer, National Cancer
Institute of the United States, National Cancer Institute of
Canada. J Natl Cancer Inst. 92:205–216. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ye SL, Chen X, Yang J, Bie P, Zhang S, Liu
F, Liu L, Zhou J, Dou K, Hao C, et al: Safety and efficacy of
sorafenib therapy in patients with hepatocellular carcinoma: Final
outcome from the Chinese patient subset of the GIDEON study.
Oncotarget. 7:6639–6648. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Llovet JM, Peña CE, Lathia CD, Shan M,
Meinhardt G and Bruix J: SHARP Investigators Study Group: Plasma
biomarkers as predictors of outcome in patients with advanced
hepatocellular carcinoma. Clin Cancer Res. 18:2290–2300. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhang Z, Zhou X, Shen H, Wang D and Wang
Y: Phosphorylated ERK is a potential predictor of sensitivity to
sorafenib when treating hepatocellular carcinoma: Evidence from an
in vitro study. BMC Med. 7:412009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bolondi L, Burroughs A, Dufour JF, Galle
PR, Mazzaferro V, Piscaglia F, Raoul JL and Sangro B: Heterogeneity
of patients with intermediate (BCLC B) Hepatocellular Carcinoma:
Proposal for a subclassification to facilitate treatment decisions.
Semin Liver Dis. 32:348–359. 2012.PubMed/NCBI
|
|
29
|
Kim J and Bae JS: Tumor-associated
macrophages and neutrophils in tumor microenvironment. Mediators
Inflamm. 2016:60581472016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Motomura T, Shirabe K, Mano Y, Muto J,
Toshima T, Umemoto Y, Fukuhara T, Uchiyama H, Ikegami T, Yoshizumi
T, et al: Neutrophil-lymphocyte ratio reflects hepatocellular
carcinoma recurrence after liver transplantation via inflammatory
microenvironment. J Hepatol. 58:58–64. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kuang DM, Zhao Q, Wu Y, Peng C, Wang J, Xu
Z, Yin XY and Zheng L: Peritumoral neutrophils link inflammatory
response to disease progression by fostering angiogenesis in
hepatocellular carcinoma. J Hepatol. 54:948–955. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kusumanto YH, Dam WA, Hospers GA, Meijer C
and Mulder NH: Platelets and granulocytes, in particular the
neutrophils, form important compartments for circulating vascular
endothelial growth factor. Angiogenesis. 6:283–287. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Li XF, Chen DP, Ouyang FZ, Chen MM, Wu Y,
Kuang DM and Zheng L: Increased autophagy sustains the survival and
pro-tumourigenic effects of neutrophils in human hepatocellular
carcinoma. J Hepatol. 62:131–139. 2015. View Article : Google Scholar : PubMed/NCBI
|