Introduction
It has been demonstrated that there is an
association between chronic inflammation and carcinogenesis
(1), and that subclinical or even
undetectable inflammation may be as significant as chronic
inflammation in increased cancer risk, cancer development and
progression (1). Chronic
inflammation may promote excessive cell proliferation and activate
a cascade of cellular events, promoting tumor cell growth (2). Furthermore, tumor progression per
se may also stimulate host immune response and
inflammation.
Erythrocyte sedimentation rate (ESR) is the most
widely used laboratory test for evaluating the inflammatory status
in clinical practice, including infection, autoimmune and malignant
diseases (3). Elevated ESR is
frequently encountered in patients with cancer. The outcome in
various malignancies depends on the type of the underlying
disorder, the stage and duration of the disease, and the regimen
and intensity of the antitumor treatment. In addition, an elevated
ESR level has also been identified as a prognostic factor adversely
affecting survival in cancer patients (2–8). A
number of studies indicated that an increased ESR level is
associated with worse survival; patients with higher ESR values in
various malignancies, including colorectal cancer (2), renal cell cancer (4), head and neck cancer (5), soft tissue sarcoma (6), breast cancer (7), glioma (8) and prostate cancer (9), had a shorter survival compared with
those with normal ESR levels.
Although there have been sufficient data on other
types of tumors, to the best of our knowledge, the prognostic value
of ESR in melanoma patients has not been adequately investigated
(10,11) and the significance of elevated ESR
levels in melanoma patients has not been fully elucidated. However,
increased ESR levels have been identified as an adverse prognostic
factor for survival in melanoma patients as a secondary finding
when different parameters were investigated in our previously
published trials (12–15).
In the present study, the ESR levels were evaluated
in cutaneous melanoma patients, and the associations with disease
prognosis and various known clinical variables were determined.
Patients and methods
Patients
A total of 139 adult patients with histologically
confirmed cutaneous melanoma in whom ESR was determined were
included in the present analysis and were retrospectively
investigated. The patient records were retrieved from the cancer
registry of the Institute of Oncology, University of Istanbul
(Istanbul, Turkey) for review of the clinicopathological factors
and patient survival. The patients were treated and followed-up
according to standard international guidelines, such as National
Comprehensive Cancer Network (https://www.nccn.org/patients/guidelines/melanoma/)
and European Society for Medical Oncology (http://www.esmo.org/Guidelines/Melanoma)
guidelines.
The ESR values of the patients were determined at
first admission by the standard Westergren method (16,17). The
study protocol was reviewed and approved by the local Ethics
Committee.
Statistical analysis
Comparisons between clinicopathological
characteristics and ESR values were performed using the
Mann-Whitney U test, independent samples t-test and logistic
regression test. Receiver operating characteristic curves were used
to define the cut-off value of ESR levels for survival analysis.
Kaplan-Meier analysis was used for estimation of patient survival
and differences in outcomes were assessed using log-rank
statistics. A P-value of ≤0.05 was considered to indicate
statistically significant differences.
Results
Patient characteristics
A total of 139 cutaneous melanoma patients were
enrolled in the present study. The median age of the patients was
52 years (range, 16–88 years). The demographic and
clinicopathological characteristics are summarized in Table I. The median value of ESR values of
the patients was 22 mm/h (range, 2–122 mm/h). Significant
differences in ESR were only found in association with sex,
histology, blood hemoglobin level, lactate dehydrogenase (LDH)
levels and metastatic disease (Table
I). Female patients (P=0.006) and those with nodular histology
(P=0.005), low hemoglobin concentration (P<0.001), higher LDH
levels (P=0.003) and metastatic disease (P<0.001) were more
likely to have elevated ESR values. However, the ESR levels were
not found to be significantly associated with age, site of lesion,
or pathological indicators such as Clark's level of invasion,
Breslow's depth, mitotic rate, ulceration, vertical growth phase,
tumor-infiltrating lymphocytes, regression, neurotropism,
lymphovascular invasion and BRAF (V600E) mutation (P>0.05). ESR
was also not associated with lymph node involvement (P=0.188) or
responsiveness to chemotherapy (P=0.390).
 | Table I.Patient/disease characteristics and
correlations between ESR and various clinicopathological
variables. |
Table I.
Patient/disease characteristics and
correlations between ESR and various clinicopathological
variables.
| Variables | n | ESR (mm/h), median
(range) | HR (95% CI) | P-value |
|---|
| No. of patients | 139 | 22 (2–122) |
|
|
| Age (years) |
|
| 1.001
(0.985–1.018) | 0.162 |
|
<50 | 64 | 20.5 (2–122) |
|
|
| ≥50 | 75 | 23 (3–83) |
|
|
| Sex |
|
| 1.017
(0.999–1.035) | 0.006 |
| Male | 87 | 19 (2–122) |
|
|
|
Female | 52 | 30 (5–83) |
|
|
| Site of lesion |
|
| 1.005
(0.984–1.026) | 0.652 |
|
Axial | 69 | 22 (3–70) |
|
|
|
Extremities | 58 | 19.5 (2–83) |
|
|
| Histopathology |
|
| 0.978
(0.953–1.003) | 0.005 |
|
Nodular | 24 | 27 (10–70) |
|
|
|
Others | 74 | 19.5 (2–83) |
|
|
| Clark's level |
|
| 1.012
(0.979–1.047) | 0.280 |
|
I–III | 19 | 16 (3–63) |
|
|
| IV–V | 83 | 21 (5–83) |
|
|
| Breslow's thickness,
mm |
|
| 1.016
(0.981–1.051) | 0.398 |
|
<2 | 20 | 18.5 (3–62) |
|
|
| ≥2 | 85 | 21 (3–83) |
|
|
| Mitotic rate,
n/mm2 |
|
| 1.011
(0.986–1.036) | 0.387 |
| ≤3 | 47 | 20 (3–83) |
|
|
|
>3 | 50 | 21 (7–83) |
|
|
| Ulceration |
|
| 1.028
(0.999–1.059) | 0.115 |
|
Absent | 38 | 20 (3–52) |
|
|
|
Present | 62 | 22 (3–83) |
|
|
| Neurotropism |
|
| 1.013
(0.953–1.075) | 0.690 |
|
Absent | 58 | 20.5 (3–83) |
|
|
|
Present | 3 | 25 (22–40) |
|
|
| Vertical growth
phase |
|
| 0.999
(0.925–1.079) | 0.988 |
|
Absent | 3 | 15 (10–42) |
|
|
|
Present | 60 | 20 (3–83) |
|
|
| Lymphovascular
invasion |
|
| 1.026
(0.994–1.060) | 0.107 |
|
Absent | 72 | 19.5 (3–66) |
|
|
|
Present | 15 | 26 (5–83) |
|
|
| Tumor-infiltrating
lymphocytes |
|
| 1.008
(0.978–1.039) | 0.599 |
|
Absent | 23 | 16 (3–83) |
|
|
|
Present | 70 | 21.5 (3–83) |
|
|
| Regression |
|
| 1.012
(0.987–1.039) | 0.350 |
|
Absent | 61 | 20 (3–66) |
|
|
|
Present | 28 | 21 (7–83) |
|
|
| BRAF (V600E)
mutation |
|
| 0.972
(0.931–1.015) | 0.171 |
|
Negative | 12 | 27 (7–96) |
|
|
|
Positive | 15 | 22 (6–63) |
|
|
| Hemoglobin level |
|
| 0.953
(0.931–0.975) | <0.001 |
| Low | 36 | 35.5 (10–122) |
|
|
|
Normal | 98 | 18 (2–83) |
|
|
| Serum lactate
dehydrogenase |
|
| 1.033
(1.012–1.055) | 0.003 |
|
Normal | 109 | 21 (2–83) |
|
|
| High | 24 | 34 (11–122) |
|
|
| Lymph node
metastasis |
|
| 1.023
(0.994–1.054) | 0.188 |
| No | 35 | 18 (2–52) |
|
|
| Yes | 68 | 22 (5–83) |
|
|
| No. of lymph node
metastasis |
|
| 1.028
(0.996–1.060) | 0.078 |
| 1 | 37 | 21 (5–51) |
|
|
| ≥2 | 30 | 22 (5–83) |
|
|
| Metastatic stage
(M1) |
|
| 1.044
(1.022–1.066) | <0.001 |
| No | 99 | 18 (2–75) |
|
|
|
Yes | 40 | 31.5 (2–122) |
|
|
| Stage of metastatic
disease |
|
| 0.989
(0.965–1.014) | 0.401 |
|
M1a-b | 14 | 37 (15–96) |
|
|
|
M1c | 26 | 31.5 (2–122) |
|
|
| Response to
chemotherapy |
|
| 0.987
(0.959–1.016) | 0.390 |
| No | 20 | 38 (15–122) |
|
|
|
Yes | 14 | 31.5 (6–83) |
|
|
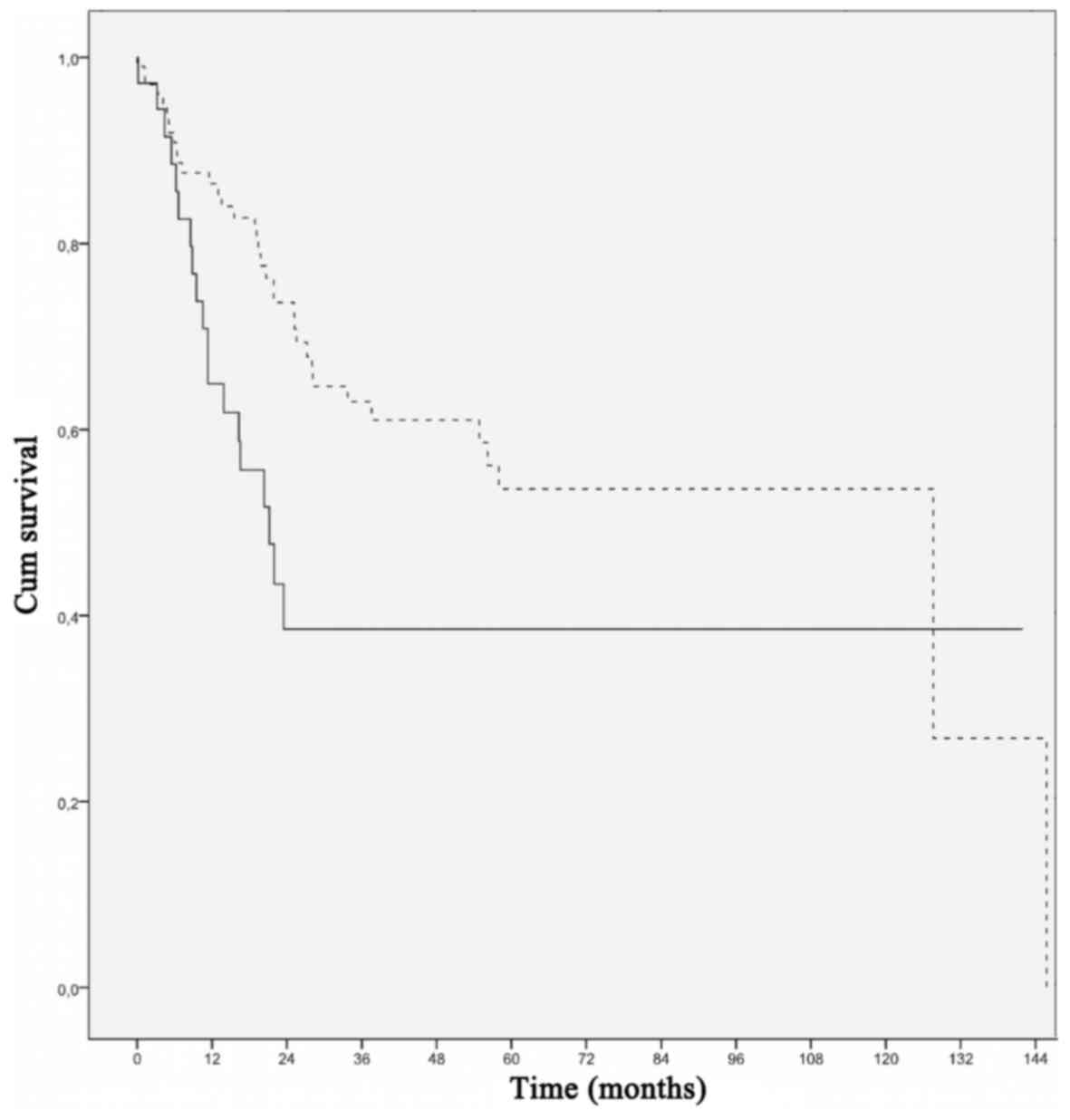
Effect of elevated ESR on
survival
When survival analyses of possible
clinicopathological variables affecting outcome were performed,
nodular histology (P=0.043), high mitotic rate (P=0.004), presence
of ulceration (P=0.034), presence of lymphovascular invasion
(P<0.001), increased serum LDH level (P<0.001), lymph node
involvement (P=0.005), multiple node involvement (P=0.010), distant
metastasis (P<0.001) and failure to respond to chemotherapy
(P=0.002) were found to be poor prognostic factors for overall
survival (Table II). ESR was found
to be significantly associated with outcome, with patients with
elevated ESR exhibiting worse survival compared with those with
normal ESR values (P=0.012) (Table
II, Fig. 1).
| Table II.Analysis of variables in association
with overall survival. |
Table II.
Analysis of variables in association
with overall survival.
| Variables | HR (95% CI) | P-value |
|---|
| Age | 1.037
(0.607–1.772) | 0.893 |
| Sex | 0.677
(0.377–1.215) | 0.191 |
| Site of lesion | 0.608
(0.332–1.115) | 0.104 |
| Histology | 0.457
(0.211–0.993) | 0.043 |
| Clark's level | 2.054
(0.717–5.881) | 0.171 |
| Breslow's
thickness | 1.824
(0.702–4.743) | 0.211 |
| Ulceration | 2.362
(1.045–5.341) | 0.034 |
| Mitotic rate | 2.972
(1.354–6.523) | 0.004 |
| Neurotropism | 2.430
(0.314–18.77) | 0.379 |
| Vertical growth
phase | 22.06
(0.001–48851) | 0.356 |
| Lymphovascular
invasion | 5.681
(2.432–13.27) | <0.001 |
| Tumor-infiltrating
lymphocytes | 0.886
(0.383–2.049) | 0.776 |
| Regression | 0.892
(0.370–2.146) | 0.798 |
| BRAF (V600E)
mutation | 1.037
(0.397–2.709) | 0.940 |
| Hemoglobin
level | 0.903
(0.492–1.657) | 0.740 |
| Serum lactate
dehydrogenase | 3.844
(2.104–7.020) | <0.001 |
| Lymph node
metastasis | 4.002
(1.396–11.47) | 0.005 |
| No. of lymph node
metastases | 2.729
(1.233–6.044) | 0.010 |
| Metastatic
disease | 8.299
(4.717–14.60) | <0.001 |
| Stage of metastatic
disease | 1.384
(0.647–2.964) | 0.398 |
| Response to
chemotherapy | 0.268
(0.110–0.651) | 0.002 |
| Erythrocyte
sedimentation rate | 2.033
(1.156–3.577) | 0.012 |
Discussion
The aim of the present study was to evaluate the
prognostic value of ESR elevation focusing specifically on
cutaneous melanoma patients. The study analyzed 139 melanoma
patients, including all disease stages, which, to the best of our
knowledge, is the largest population-based sample size from a
single institution to date.
At the time of the analysis, to our knowledge, only
a limited number of studies had focused on the prognostic value of
the ESR level in cutaneous melanoma patients (10,11). In
the Norwegian Radium Hospital, 177 metastatic melanoma patients
treated with various chemotherapy regimens were included in a
regression analysis of prognostic factors (10). Multivariate analysis identified ESR
>15 mm/h as a significant prognostic factor indicating short
survival with a low probability of surviving for 3 months, whereas
patients with normal ESR values had a median survival of 11.5
months, with 94% surviving for 3 months. In another study, 71
patients with metastatic disease were included (11). The serum ESR levels were
significantly elevated in patients with progressive disease. On
logistic regression analysis, ESR was found to be of low
specificity.
The present study revealed that an elevated ESR
level was associated with metastatic disease, but not lymph node
involvement. ESR level at diagnosis was a prognostic factor for
survival in melanoma patients and it was associated with other poor
prognostic factors. A number of previously reported trials
suggested that increased ESR values at presentation may adversely
affect prognosis in patients with various types of cancer (2,4–9). Our findings were in agreement with the
results reported by these studies. A limited number of our
previously performed trials, which included small sample sizes
(<100 patients), were focused specifically on melanoma and
yielded similar confirmative results (12–15). The
P-values in those studies were significantly low, namely P<0.001
(12,14), P=0.001 (13) and P=0.002 (15).
The association of systemic inflammation and patient
survival may have implications for immune modulation in melanoma.
The correlation of inflammatory status with metastatic disease
suggests that melanoma with metastasis may be more immunogenic,
thus inducing a more prominent inflammatory response. ESR, as a
widely used laboratory test for evaluating the inflammatory status
in clinical practice was found to be significantly associated with
survival in melanoma patients, suggesting an important role of
inflammation in melanoma progression. Inflammatory cells have been
suggested to promote carcinogenesis, possibly by augmenting DNA
damage, promoting tumor cell proliferation, and stimulating
angiogenesis and metastasis.
In conclusion, elevated ESR was found to be
associated with metastasis and it predicts worse survival in
cutaneous melanoma patients. Therefore, ESR may be a prognostic
risk factor and be correlated with other powerful prognostic
variables. Despite its relatively low sensitivity and specificity
in monitoring disease activity, the ESR assessment is a widely
used, cost-effective and simple test, which may be a viable
alternative to novel, more expensive methods in the prognostication
of cutaneous melanoma patients. The present study was limited by
its retrospective design and relatively small number of included
patients. A prospective study of a larger patient sample is
required to confirm the results of the present study.
References
|
1
|
Grivennikov SI, Greten FR and Karin M:
Immunity, inflammation, and cancer. Cell. 140:883–899. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Seong MK: Prognostic inflammation score in
surgical patients with colorectal cancer. J Korean Med Sci.
30:1793–1799. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bochen K, Krasowska A, Milaniuk S,
Kulczynska M, Prystupa A and Dzida G: Erythrocyte sedimentation
rate-an old marker with new applications. J Pre-Clin Clin Res.
5:50–55. 2011.
|
|
4
|
Sengupta S, Lohse CM, Cheville JC,
Leibovich BC, Thompson RH, Webster WS, Frank I, Zincke H, Blute ML
and Kwon ED: The preoperative erythrocyte sedimentation rate is an
independent prognostic factor in renal cell carcinoma. Cancer.
106:304–312. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chen Z, Malhotra PS, Thomas GR, Ondrey FG,
Duffey DC, Smith CW, Enamorado I, Yeh NT, Kroog GS, Rudy S, et al:
Expression of proinflammatory and proangiogenic cytokines in
patients with head and neck cancer. Clin Cancer Res. 5:1369–1379.
1999.PubMed/NCBI
|
|
6
|
Choi ES, Kim HS and Han I: Elevated
preoperative systemic inflammatory markers predict poor outcome in
localized soft tissue sarcoma. Ann Surg Oncol. 21:778–785. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Eboreime O, Atoe K and Idemudia JO:
Erythrocyte sedimentation rate and C-reactive protein levels in
breast cancer patients in Benin City, Nigeria. IOSR J Dent Med Sci.
14:116–119. 2015.
|
|
8
|
Strojnik T, Smigoc T and Lah TT:
Prognostic value of erythrocyte sedimentation rate and C-reactive
protein in the blood of patients with glioma. Anticancer Res.
34:339–347. 2014.PubMed/NCBI
|
|
9
|
Johansson JE, Sigurdsson T, Holmberg L and
Bergström R: Erythrocyte sedimentation rate as a tumor marker in
human prostatic cancer. An analysis of prognostic factors in 300
population-based consecutive cases. Cancer. 70:1556–1563. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Heimdal K, Hannisdal E and Gundersen S:
Regression analyses of prognostic factors in metastatic malignant
melanoma. Eur J Cancer Clin Oncol. 25:1219–1223. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Deichmann M, Benner A, Bock M, Jäckel A,
Uhl K, Waldmann V and Näher H: S100-Beta, melanoma-inhibiting
activity, and lactate dehydrogenase discriminate progressive from
nonprogressive American Joint Committee on Cancer stage IV
melanoma. J Clin Oncol. 17:1891–1896. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tas F, Ciftci R, Kilic L, Bilgin E, Keskin
S, Sen F, Yildiz I and Yasasever V: Clinical and prognostic
significance of coagulation assays in melanoma. Melanoma Res.
22:368–375. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tas F, Karabulut S, Serilmez M, Yildiz I,
Sen F, Ciftci R and Duranyildiz D: Clinical significance of serum
M30 and M65 levels in melanoma. Melanoma Res. 23:390–395. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tas F, Karabulut S, Bilgin E, Tastekin D
and Duranyildiz D: Clinical significance of serum fibronectin and
vitronectin levels in melanoma patients. Melanoma Res. 24:475–479.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tas F, Bilgin E, Erturk K and Duranyildiz
D: Clinical significance of serum claudin-1 levels in melanoma
patients. Melanoma Res. 26:377–381. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Westergren A: The technique of the red
cell sedimentation reaction. Am Rev Tuberc. 14:94–101. 1926.
|
|
17
|
ICSH recommendations for measurement of
erythrocyte sedimentation rate. International Council for
Standardization in Haematology (Expert Panel on Blood Rheology). J
Clin Pathol. 46:198–203. 1993. View Article : Google Scholar : PubMed/NCBI
|