Introduction
Ovarian cancer is the second most frequent
gynecological cancer complicating pregnancy (1,2). Due to
routine ultrasound examinations, the incidence of abdominal masses
diagnosed during pregnancy has increased, and is estimated to be
2–10% of all pregnancies (1–3). Functional cysts are the most common
type of adnexal mass associated with pregnancy (1,2,4). The majority of benign masses are
dermoid cysts, serous cystadenomas or mucinous cystadenomas; on
rare occasions, endometriomas, hydrosalpinx, heterotopic pregnancy
or leiomyomas may be diagnosed (4).
Only 3–6% of all ovarian cysts associated with pregnancy are
malignant, and their diagnosis and management is complicated due to
the lack of large prospective randomized trials and cohort studies
(2). Malignant germ cell tumors are
the most common ovarian malignancies during pregnancy, while
epithelial cancers with low malignant potential are reported less
frequently (1,2,5). The
incidence of epithelial ovarian cancer is 1:12,000–1:50,000 of
pregnancies (1). There are no exact
data on mortality due to epithelial ovarian cancer in pregnancy;
however, the prognosis is similar to that of non-pregnant patients
(6). The rare occurrence and scant
data on this condition prompted the reporting of the present
case.
Case report
In September 2016, a 23-year-old nulliparous woman
was referred to the Department of Obstetrics and Gynecology of Zala
County Saint Rafael Hospital (Zalaegerszeg, Hungary) from another
hospital due to suspected preterm labor in the 27th gestational
week. During early pregnancy, a left ovarian mass was incidentally
detected, which was considered to be a dermoid cyst. The operation
offered was refused by the patient at the time. On bimanual
examination, a significantly thinned, one-finger dilated cervix was
detected. Corticosteroid prophylaxis was administered and
intravenous tocolysis with β-mimetics was started.
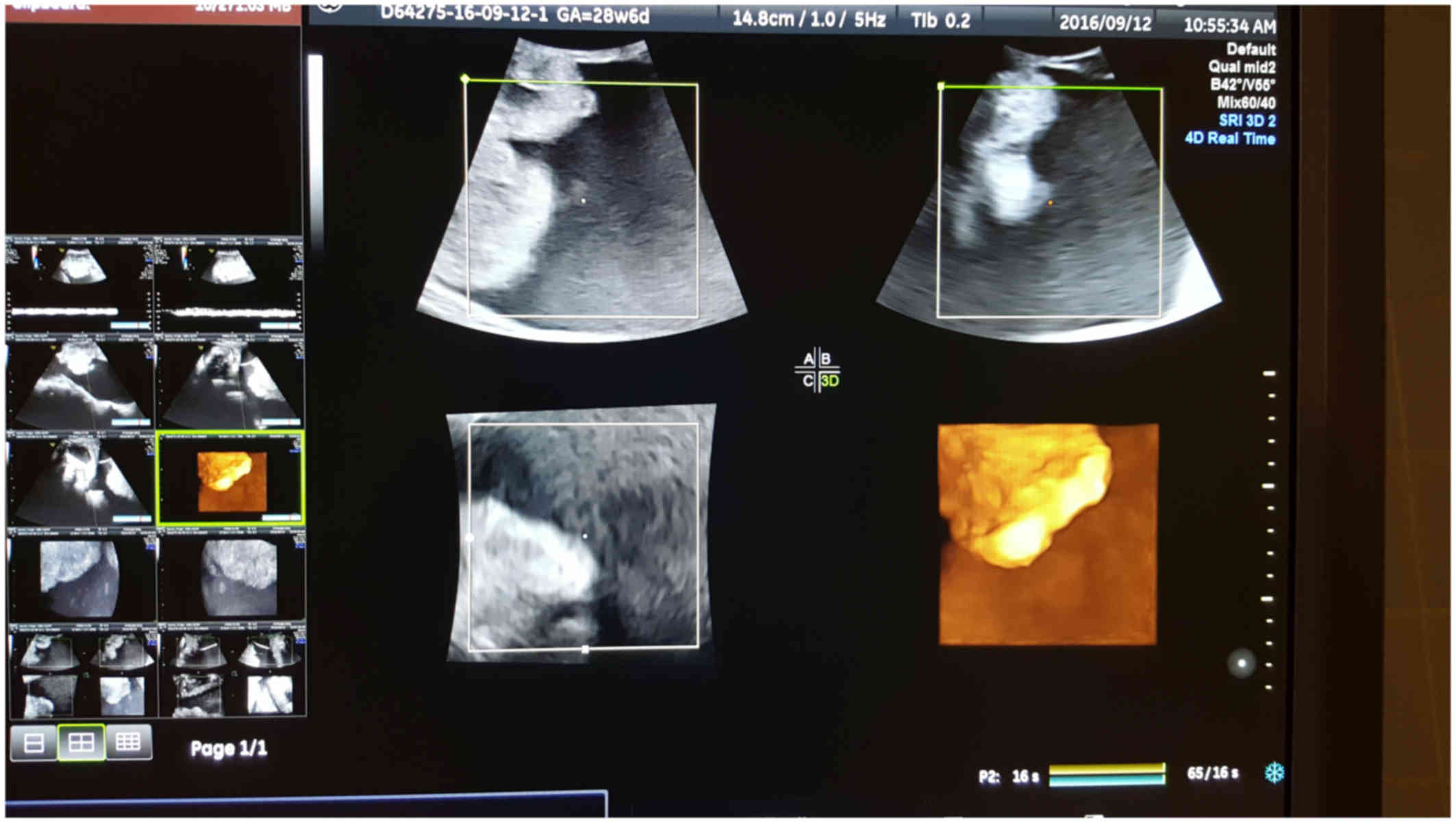
Pelvic ultrasound examination, performed on
admission, demonstrated a multicystic ovarian mass ~30 cm wide,
with low-impedance circulation, dislocating the uterus (Fig. 3). The papillary structure of the mass
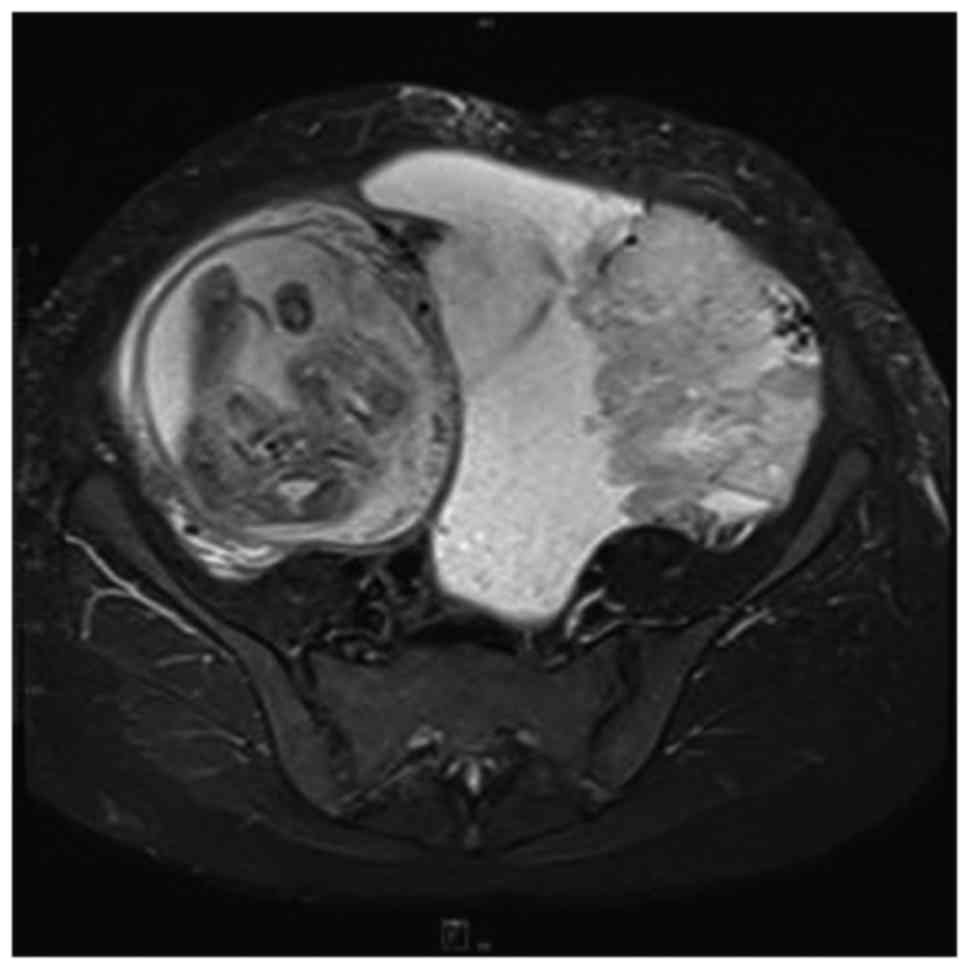
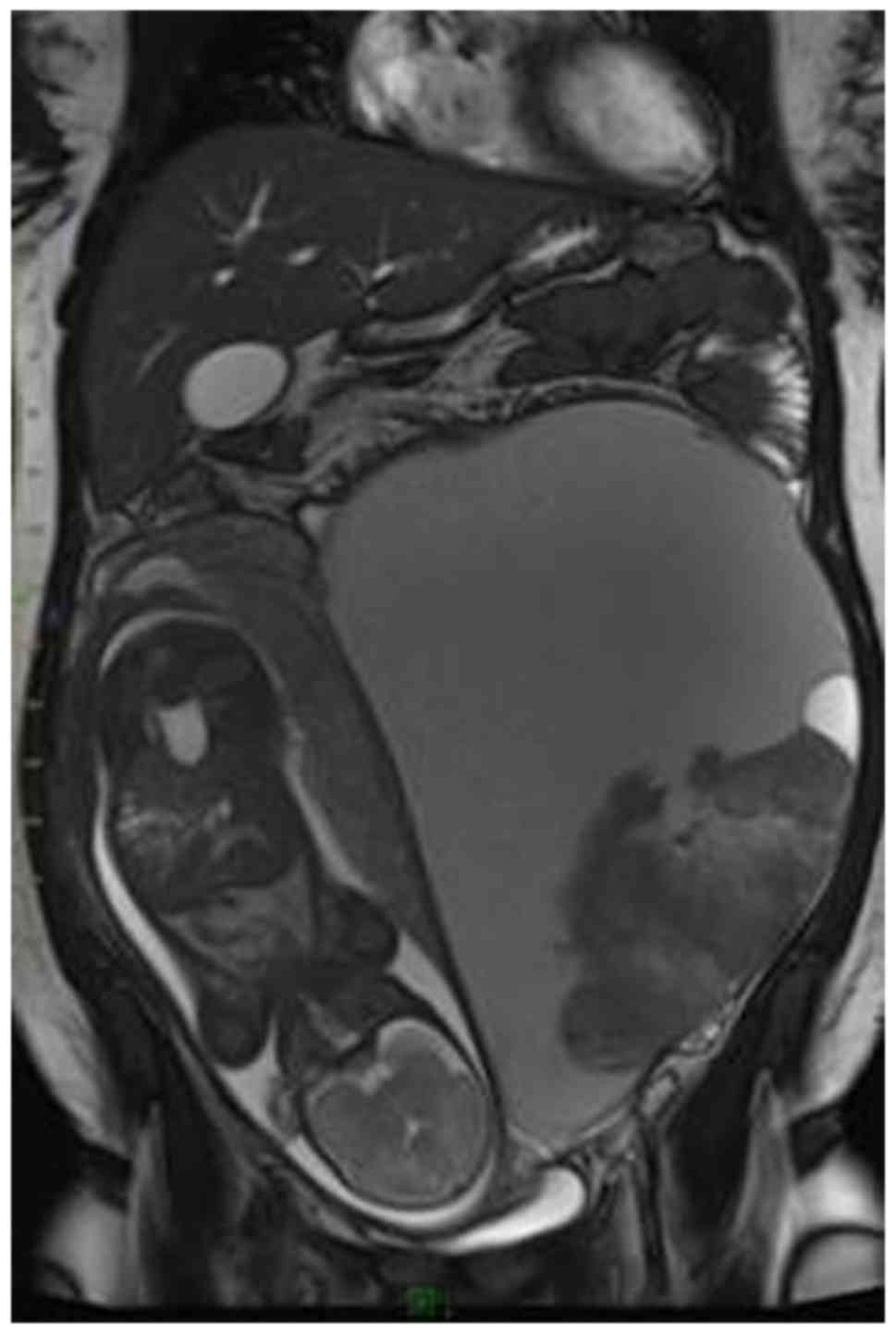
strongly suggested ovarian cancer. Pelvic magnetic resonance
imaging (MRI) revealed a bizarre mass in the left ovary measuring
20×26 cm, morphologically and structurally suspicious of malignancy
(Figs. 1 and 2). The serum levels of tumor markers were
in the normal range, which may be explained by the typical
irrelevance of the tumor markers during pregnancy.
Due to the rapid increase in size of the ovarian
cyst, an exploratory laparotomy was planned. However, as a result
of the preterm rupture of the membranes immediately prior to the
operation, the pregnancy could not be preserved; therefore, a
cesarean section with left adnexectomy was performed, taking into
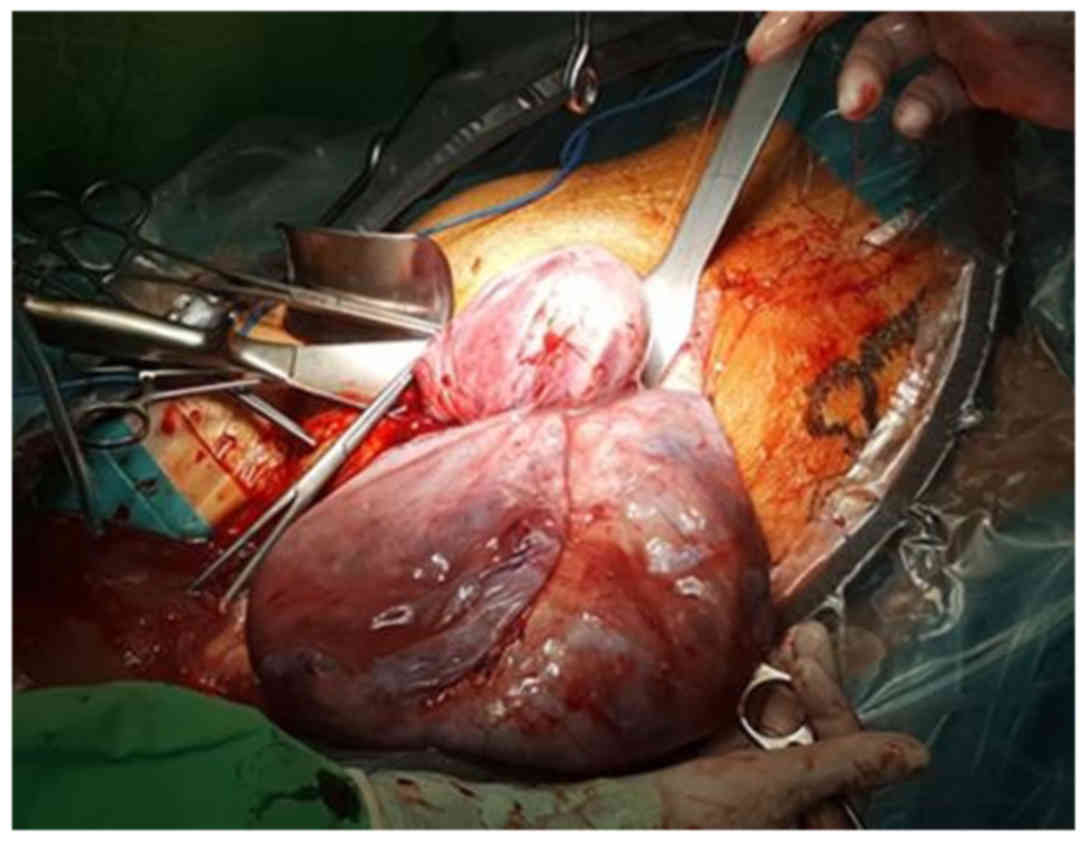
consideration the age of the patient. During surgery, a large
amount of viscous, mucinous fluid was discharged from the cystic
mass. Left adnexectomy was performed and biopsies of the right
ovary and omentum were collected for histopathological examination
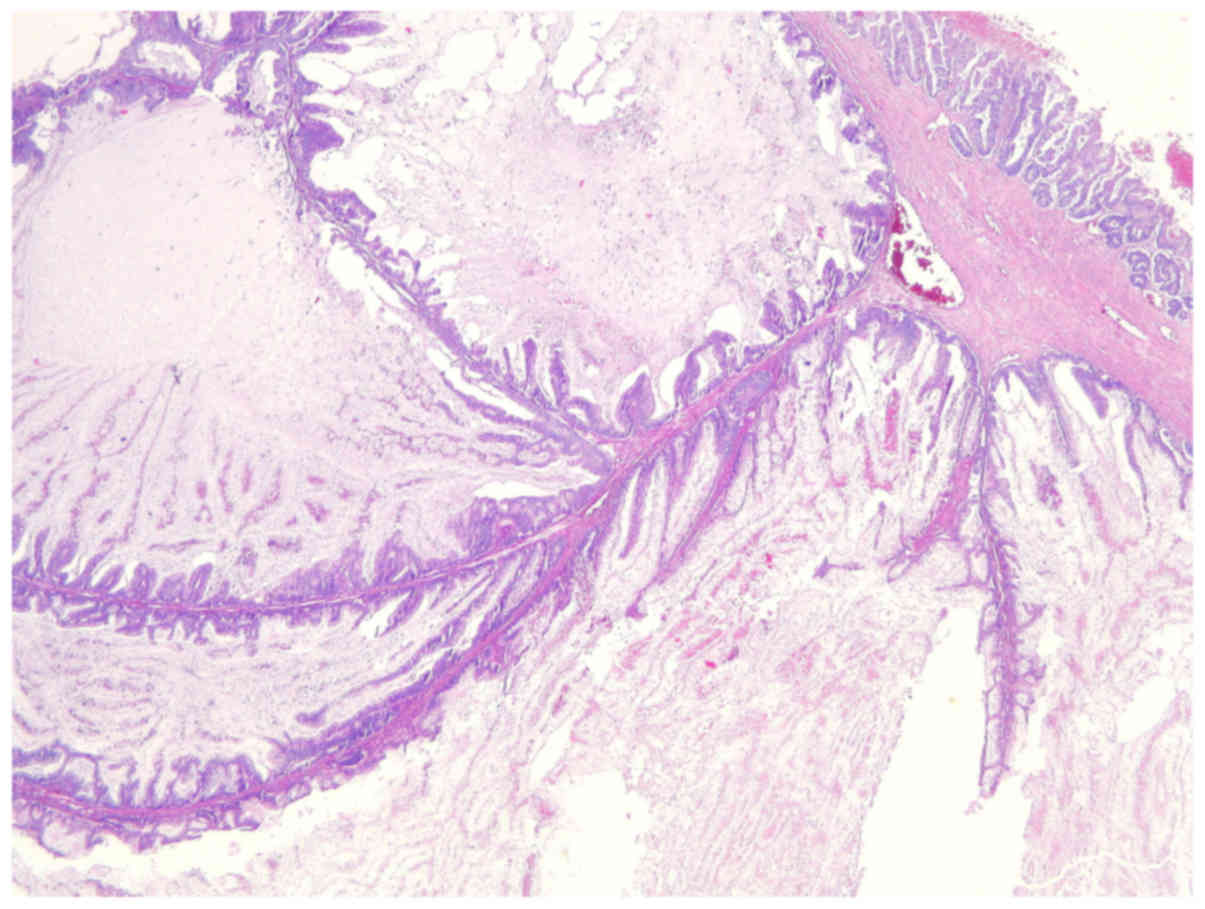
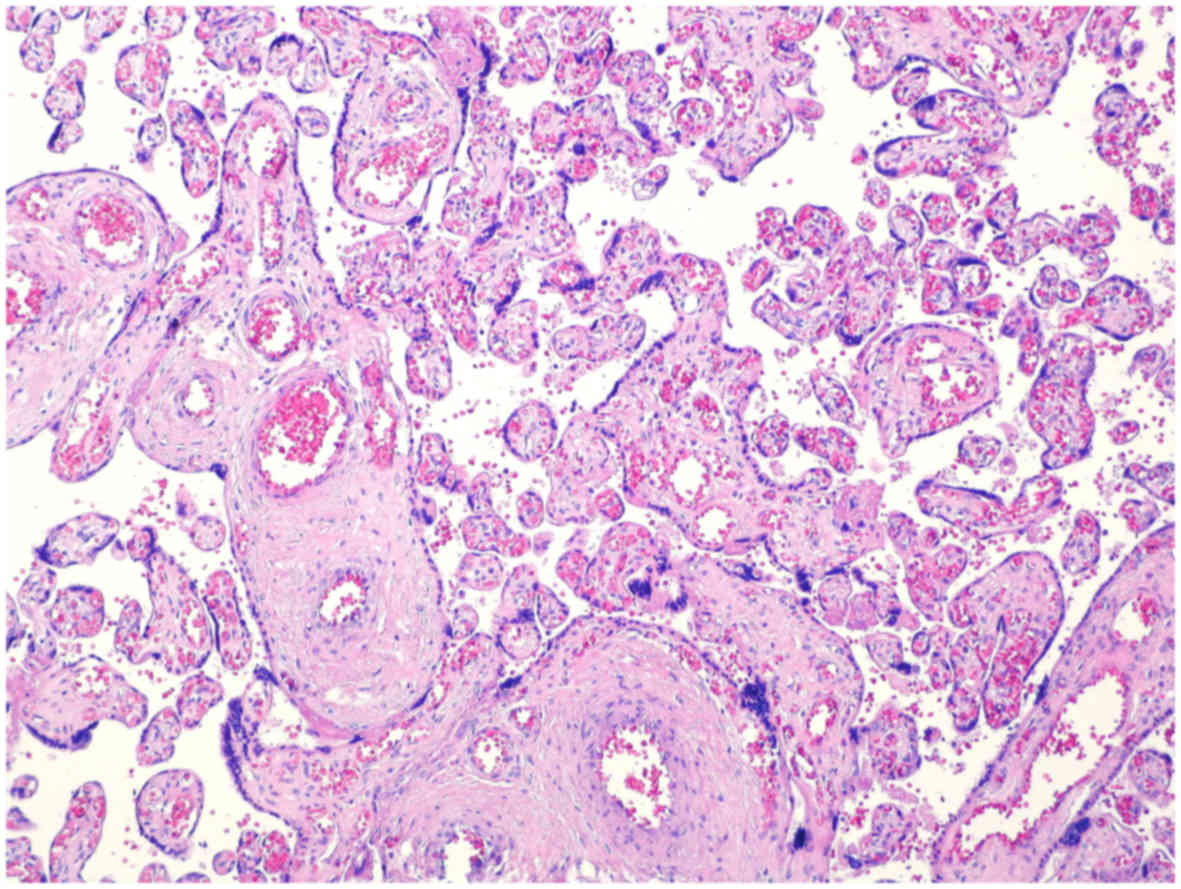
(Figs. 4 and 5). A 910-g preterm infant was born in good
condition by cesarean delivery.
The histopathological findings confirmed the left
ovarian mass to be a low-grade papillary mucinous
cystadenocarcinoma (Figs. 6 and
7). The results of the biopsies from
the omentum and right ovary were negative. The oncological team
suggested adjuvant chemotherapy with carboplatin and paclitaxel.
According to the decision of the oncological team, 6 cycles of
paclitaxel and carboplatin chemotherapy were administered. At the
last follow-up visit (May 29, 2017), all the tumor markers were
negative, and the control MRI and ultrasound examinations did not
reveal tumor recurrence or pathological lymph nodes.
The patient provided informed consent regarding the
publication of the case details and associated images.
Discussion
The incidence of adnexal masses diagnosed during
early pregnancy is 1–4%, and the majority are of ovarian origin
(7,8). Ovarian tumors rarely cause lower
abdominal pain or other symptoms during pregnancy (1,8).
Approximately 2–6% of ovarian tumors associated with pregnancy are
malignant (6,8). Ovarian malignant tumors are more
frequently reported in primigravidas, and the majority are
diagnosed at an early stage (<1C according to the International
Federation of Obstetrics and Gynecology staging guidelines) by
routine ultrasound examinations (4–6,8–10).
Due to its high sensitivity and specificity for
characterizing the morphology of abdominal masses, an ultrasound
examination is the optimal diagnostic tool in pregnancy, and it may
also differentiate between benign and malignant masses (7,11). The
malignant nature of ovarian tumors is indicated by several
sonographic characteristics such as size, solid component or
complex appearance, papillary structure, internal septations,
irregular borders, increased vascularity and low resistance to
blood flow (3). Ultrasound
examinations are not capable of differentiating between benign and
low malignant potential tumors; therefore, further imaging
examinations are necessary (7). MRI
examinations may be safely performed during the second and third
trimesters; furthermore, they may also reveal potential
extraovarian spread (1,11).
The high levels of tumor markers are helpful in
differentiating between benign and malignant tumors. Carbohydrate
antigen-125 is secreted by 80–90% of epithelial ovarian tumors
(3), but in pregnancy the tumor
markers may be normally elevated, or may indicate other
complications, such as hemolysis/elevated liver enzymes/low
platelet count (HELLP syndrome), preeclampsia, or miscarriage
(11). The elevation of inhibin,
human chorionic gonadotropin and α-fetoprotein may indicate germ
cell or sex cord stromal ovarian tumors, or fetal aberrations
(3,4).
The management of malignant tumors associated with
pregnancy represents a challenge, as both the fetal and maternal
well-being must be taken into consideration (12). The therapy is guided by the tumor
type (histopathological subtype, tumor differentiation, nodal
status) and size, gestational age, and the result of the ultrasound
examination (4,5–7,12,13).
Unilateral cysts sized <5 cm that are diagnosed in the first
trimester are usually functional cysts (1,4,10,11).
Surgical resection is indicated in the case of ovarian tumors
during pregnancy that are sized >6-7 cm, contain a solid
component (suggesting malignancy), or are associated with clinical
symptoms (such as ascites) (8,10). In
the case of asymptomatic ovarian masses, the surgery is suggested
to be planned between the 16th and 24th gestational week (6,10,11). Due
to the unfavorable prognosis of malignant epithelial cancers, the
standard therapy is staging laparotomy and adjuvant chemotherapy
following debulking surgery (1). In
two-thirds of patients diagnosed with epithelial ovarian cancer,
there is spread to the peritoneum and lymph nodes; therefore,
standard surgery includes the resection of appendages, peritoneal
metastases and lymph nodes (13).
The majority of the patients with advanced-stage disease require
chemotherapy, which should be avoided in the first trimester
(6,13). Platinum-based chemotherapy combined
with cyclophosphamide may be safely used during pregnancy; while
the data on the administration of paclitaxel are limited, there has
been no report of paclitaxel-induced fetal malformations (1,6,10).
In conclusion, malignant tumors associated with
pregnancy are becoming more frequent, probably due to the increased
age at first pregnancy (12).
Although invasive epithelial ovarian cancer is a rare diagnosis,
maternal mortality is high. The scantiness or relevant studies
makes it difficult to select the optimal therapy or diagnostic
approach. A multidisciplinary approach involving neonatologists,
oncologists and gynecologists appears to be the most important
aspect of the management of ovarian cancers during pregnancy
(11,12). The outcome of pregnancy is usually
favorable; however, the long-term effect of chemotherapy during
pregnancy remains unknown.
References
|
1
|
Palmer J, Vatish M and Tidy J: Epithelial
ovarian cancer in pregnancy: A review of the literature. BJOG.
116:480–491. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Behtash N, Karimi Zarchi M, Modares Gilani
M, Ghaemmaghami F, Mousavi A and Ghotbizadeh F: Ovarian carcinoma
associated with pregnancy: A clinicopathologic analysis of 23 cases
and review of the literature. BMC Pregnancy Childbirth. 8:32008.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nick AM and Schmeler K: Adnexal masses in
pregnancy. Perinatology. 1:13–19. 2010.
|
|
4
|
Yakasai IA and Bappa LA: Diagnosis and
Management of Adnexal Masses in Pregnancy. J Surg Tech Case Rep.
4:79–85. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhao XY, Huang HF, Lian LJ and Lang JH:
Ovarian cancer in pregnancy: A clinicopathologic analysis of 22
cases and review of the literature. Int J Gynecol Cancer. 16:8–15.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Huang HP, Fang CN and Kan YY: Chemotherapy
for ovarian mucinous cystadenocarcinoma during pregnancy: A case
report. Eur J Gynaecol Oncol. 25:635–636. 2004.PubMed/NCBI
|
|
7
|
Petinga M and Geprgiou C: The management
of adnexal masses in pregnant women: A case report and review of
literature. Australian Med Stud J. 2015.
|
|
8
|
Takeuchi T, Suzuki S, Hayashi Z, Shinagawa
T and Araki T: Primary ovarian tumor undergoing surgical management
during pregnancy. J Nippon Med Sch. 69:39–42. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Leiserowitz GS, Xing G, Cress R,
Brahmbhatt B, Dalrymple JL and Smith LH: Adnexal masses in
pregnancy: How often are they malignant. Gynecol Oncol.
101:315–321. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Roy P, Biswas B, Thomas S, Kumar RM and
Jose R: Epithelial ovarian cancer in pregnancy: Report of two
cases. Int J Sci Stud. 2:258–261. 2014.
|
|
11
|
de Haan J, Verheecke M and Amant F:
Management of ovarian cysts and cancer in pregnancy. Facts Views
Vis Obgyn. 7:25–31. 2015.PubMed/NCBI
|
|
12
|
Han SN, Verheecke M, Vandenbroucke T,
Gziri MM, Van Calsteren K and Amant F: Management of gynecological
cancers during pregnancy. Curr Oncol Rep. 16:4152014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Skrzypczyk-Ostaszewicz A and Rubach M:
Gynaecological cancers coexisting with pregnancy - a literature
review. Contemp Oncol (Pozn). 20:193–198. 2016.PubMed/NCBI
|