Bone marrow (BM) metastasis from malignant tumors
was first reported as a type of ‘diffusely infiltrative carcinoma’
by Jarcho in 1936 (1). In 1979,
Hayashi et al defined ‘disseminated carcinomatosis of the BM
(DCBM)’ as a clinical entity distinct from the usual types of
metastases to the bone and BM. They reported that diffuse
infiltrative growth is a characteristic feature of DCBM, and
pointed out the association between DCBM and systemic hematological
disorders such as hematocytopenia, disseminated intravascular
coagulation and microangiopathic hemolytic anemia (2). DCBM may also be referred to as
‘symptomatic BM metastasis’ (3) or
‘BM carcinomatosis’ (4); however,
DCBM is considered to be the most appropriate term, as it suggests
the diffuse infiltration of the BM by cancer cells and is
associated with clinically important hematological disorders.
Previous studies have reported that BM metastases from solid tumors
are frequently detected in patients with breast, stomach, lung and
prostate cancers (2,5–7).
Occult cancer cells in the BM have been reported to
occur frequently, even in patients with early-stage breast cancer;
however, whether the presence of isolated tumor cells in the BM has
prognostic significance remains controversial (8–13).
Furthermore, the association between isolated tumor cells in the BM
and clinically symptomatic BM metastasis has not been fully
elucidated (11,14), whereas clinically evident BM
metastasis is relatively common and often progresses to DCBM in
patients with metastatic or recurrent breast cancer. It was
reported that BM metastases were identified in 6–79% of breast
cancer patients at autopsy (15–17), and
27% of autopsy cases were clinically diagnosed with BM metastases
prior to autopsy (15). When
metastasis to the BM progresses to DCBM, a hematological disorder,
such as hematocytopenia, is manifested (4). Therefore, prompt diagnosis and
treatment are required to prevent the development of a
life-threatening hematological disorder. The aim of the present
study was to review the clinical characteristics and treatments of
DCBM in breast cancer patients.
The cases of 4 patients with breast cancer in whom
DCBM was diagnosed between 2014 and 2016 at the Kyushu University
Beppu Hospital (Beppu, Japan) were retrospectively analyzed. All
information was collected retrospectively from the medical records.
The clinicopathological characteristics of the patients are
summarized in Table I.
All the patients had anemia and/or thrombocytopenia
during their treatment for advanced or metastatic breast cancer.
DCBM was diagnosed pathologically from a BM biopsy and systemic
therapies were selected based on the results of the BM biopsy. The
results of the BM assessments are listed in Table II. Notably, the immunohistochemical
characteristics of the primary breast cancers were discordant with
those of the metastatic BM lesions (Tables I and II). In one case, the BM metastatic lesion
was human epidermal growth factor receptor 2 (HER2)/neu-positive,
whereas the primary lesion was HER2/neu-negative. Based on the
HER2/neu status of the BM lesion, the chemotherapy regimen for that
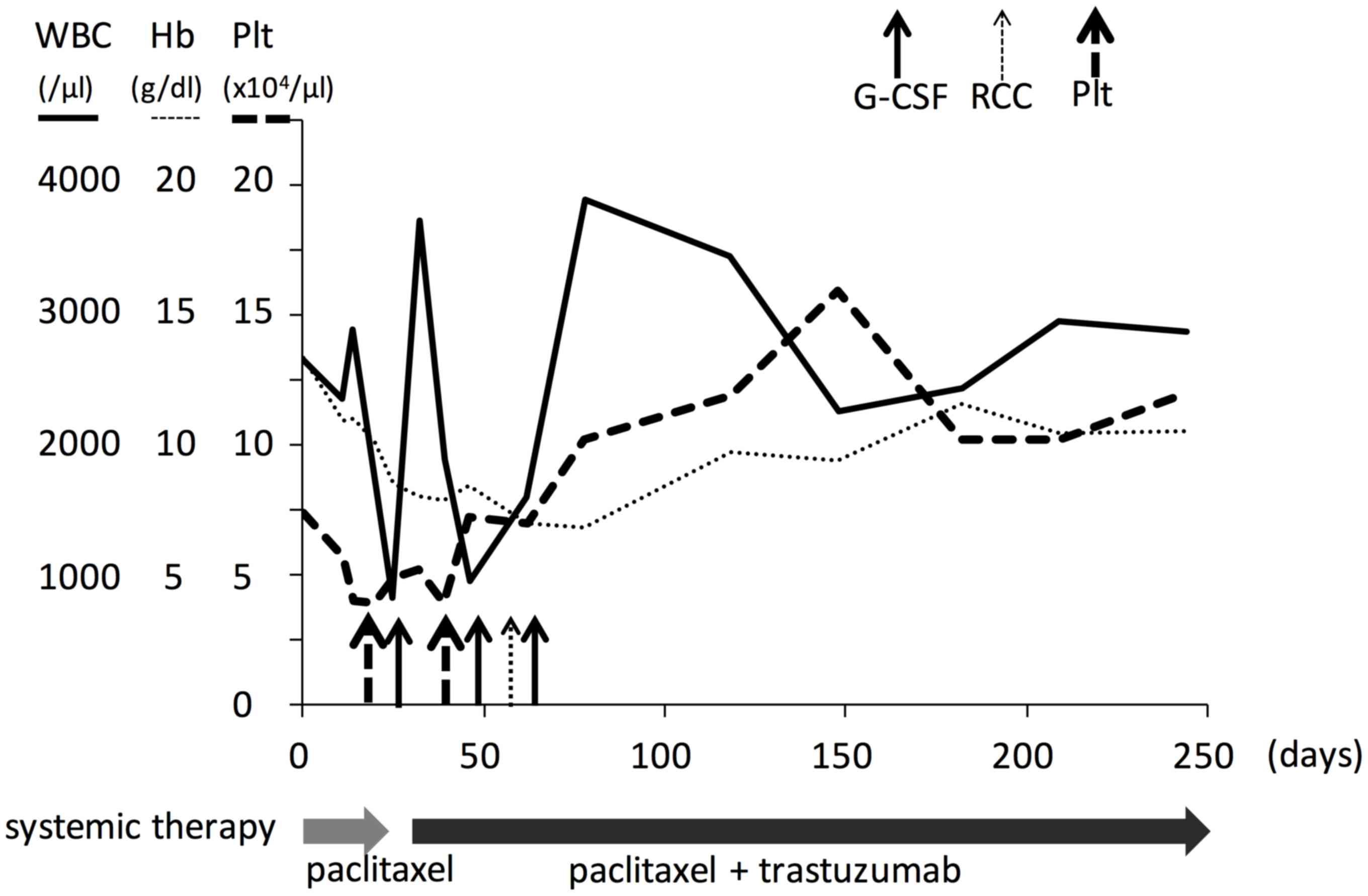
patient was changed after she was diagnosed with DCBM (Fig. 1), which led to an improved response
to treatment.
Two of the patients were treated with taxane and
trastuzumab, and their hematological disorders improved. Another
elderly patient was treated by endocrine monotherapy, and her
hematological disorder was in remission for 20 months (Table II). The clinical course of 1 of the
4 patients with DCBM is shown in Fig.
1 (case no. 1 in Tables I and
I). That patient developed
pancytopenia and was diagnosed with DCBM from breast cancer.
Following confirmation of DCBM, the patient was treated with
paclitaxel + trastuzumab. Although pancytopenia worsened as a
result of paclitaxel therapy, the hematological disorder went into
remission following administration of granulocyte
colony-stimulating factor and blood transfusions. A total of 3 of
the 4 patients who received systemic therapies, such as
chemotherapy and endocrine therapy, achieved remission of their
hematological disorders and survived for 12–30 months (Table II).
The clinicopathological data from two literature
reports and our breast cancer cases with DCBM were reviewed
(Table III) (3,4). To the
best of our knowledge, no clinicopathological characteristics of
breast cancer, apart from advanced clinical stage, have been
identified as risk factors for the development of DCBM in published
reports (3). Clinically, it is
important to suspect DCBM when a patient with advanced breast
cancer manifests a hematological disorder, such as anemia or
thrombocytopenia. Diagnostic tools, such as
18F-fluorodeoxyglucose positron emission
tomography/computed tomography and blood smear examination have
been proposed for the diagnosis of DCBM (18–20);
however, examination of a BM biopsy and/or aspirate remains the
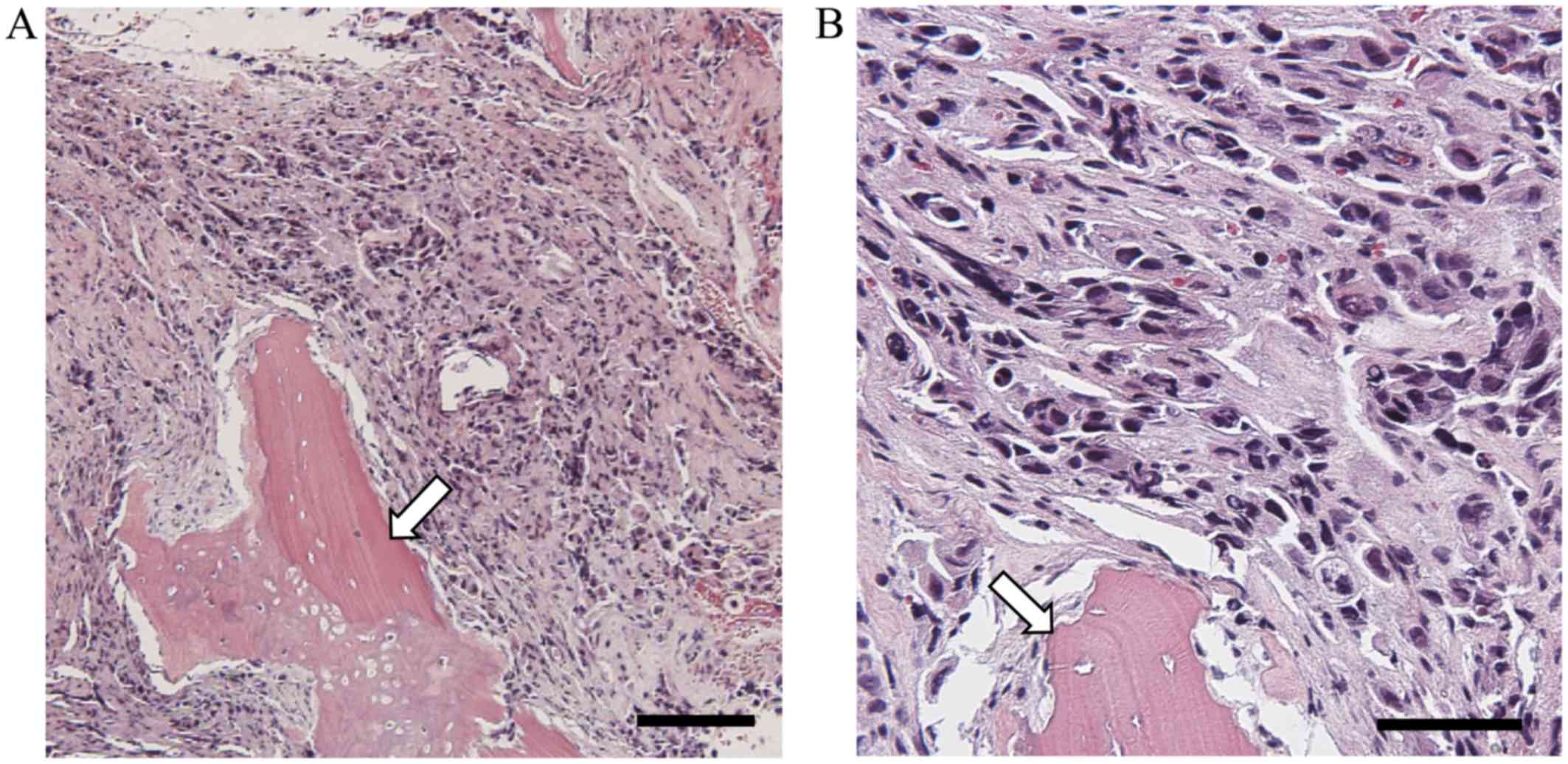
gold standard (3,14). Pathologically, DCBM is characterized
by the diffuse infiltrative growth of tumor cells in the BM, and
normal components, apart from bone trabeculae, are largely replaced
by the tumor infiltrate (Fig. 2). BM
biopsy is considered to be crucial for the accurate diagnosis of
DCBM, and is also very important for deciding on a treatment
regimen. Genetic heterogeneity of primary and metastatic tumors was
recently reported (21–23), and there have been several reports on
immunochemical discordance between primary breast cancer tumors and
metastatic lesions (24–27). Clinically, the histopathological
confirmation of metastatic tissue should be performed whenever
possible, due to the potential discordance between the expression
status of hormonal receptors and HER2/neu in primary and metastatic
breast tumors. Discordant results affect the treatment regimens
used for metastatic breast cancer patients (28).
Notably, in all 4 patients, the BM metastatic
lesions were negative for progesterone receptor (PgR) expression,
whereas the primary lesions of 2 patients (50%) were PgR-positive
(Tables I and II). PgR-negative patients with luminal
breast cancer are well-known to have a worse prognosis compared
with PgR-positive patients (29,30). The
PgR expression status has been reported to be frequently discordant
between primary and metastatic sites (31–35), and
the loss of PgR expression has been associated with worse prognosis
due to acquired resistance to hormonal therapy (26,32). The
effect of PgR status on DCBM progression is unknown, and additional
clinical reviews and molecular studies are warranted.
Prompt systemic treatment is needed for breast
cancer patients with DCBM, as DCBM is associated with hematological
abnormalities. Among the various treatment regimens for breast
cancer, the preferred regimen for DCBM from breast cancer remains
unknown. DCBM has been treated by various chemotherapy regimens
(Table III) (3,4).
Although the therapeutic effects of chemotherapy have not been
comprehensively reported, anthracycline and taxane regimens have
been more effective compared with other chemotherapy agents. Demir
et al reported disease control rates (complete response +
partial response + stable disease) of 83% (5/6), 75% (3/4) and 0%
(0/3) for anthracycline, taxane and other regimens, respectively
(3). Endocrine therapy was
administered to 1 patient, who achieved stable disease (3). Based on the patient response to therapy
reported previously and observed by us, systemic chemotherapy is
recommended for DCBM of breast cancer patients. Endocrine
(hormonal) therapy may be added in estrogen receptor-positive
cases. Due to myelotoxicity, chemotherapy appears to lead to
temporary exacerbation of the hematological disorder, and blood
transfusion is often required after the initiation of systemic
chemotherapy.
The molecular pathogenesis of DCBM in breast cancer
is not completely understood. We recently reported that the
inhibition of the F-box protein FBXW7 in BM promoted cancer
metastasis in mice (36).
FBXW7 is a gene that regulates the cell cycle, and it may
maintain cancer-initiating cells (37). Despite advances in the understanding
of the mechanism and significance of the dissemination of tumor
cells in BM, the molecular mechanism underlying the progression of
DCBM from a metastasis in the BM remains unknown. The BM
environment is considered to have unique biological properties for
the homing, survival and proliferation of circulating tumor cells
(38). DCBM is considered to
progress from BM micrometastases, but further studies are required
to elucidate the mechanism of DCBM development in breast cancer
patients.
In conclusion, DCBM is a type of metastasis that is
characterized by diffuse infiltrative growth, and is associated
with poor prognosis and hematological disorders in patients with
advanced breast cancer. A definitive diagnosis by BM biopsy and
prompt systematic therapy may prolong patient survival.
|
1
|
Jarcho S: Diffusely infiltrative
carcinoma. Arch Pathol. 22:674–696. 1936.
|
|
2
|
Hayashi H, Haruyama H, Emura Y, Kiazuka I
and Ozeki T: Disseminated carcinomatosis of the bone marrow. Jpn J
Cancer Clin. 25:329–343. 1979.(In Japanese).
|
|
3
|
Demir L, Akyol M, Bener S, Payzin KB,
Erten C, Somali I, Can A, Dirican A, Bayoglu V, Kucukzeybek Y, et
al: Prognostic evaluation of breast cancer patients with evident
bone marrow metastasis. Breast J. 20:279–287. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kopp HG, Krauss K, Fehm T, Staebler A,
Zahm J, Vogel W, Kanz L and Mayer F: Symptomatic bone marrow
involvement in breast cancer-clinical presentation, treatment, and
prognosis: A single institution review of 22 cases. Anticancer Res.
31:4025–4030. 2011.PubMed/NCBI
|
|
5
|
Yokoyama K: A clinical study of bone
marrow involvement in non-hematological malignancies. Tokyo
Jikeikai Med J. 98:1006–1019. 1983.(In Japanese).
|
|
6
|
Papac RJ: Bone marrow metastases. A
review. Cancer. 74:2403–2413. 1994.(In Japanese).
|
|
7
|
Moriwaki S, Mandai K, Okabe K, Yamauchi M,
Yamamoto A and Kamei T: Pathological analysis for the bone marrow
metastasis by aspiration and core needle biopsy. Jpn J Cancer Clin.
49:203–209. 2003.(In Japanese).
|
|
8
|
Diel IJ, Kaufmann M, Costa SD, Holle R,
von Minckwitz G, Solomayer EF, Kaul S and Bastert G:
Micrometastatic breast cancer cells in bone marrow at primary
surgery: Prognostic value in comparison with nodal status. J Natl
Cancer Inst. 88:1652–1658. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mansi JL, Gogas H, Bliss JM, Gazet JC,
Berger U and Coombes RC: Outcome of primary-breast-cancer patients
with micrometastases: A long-term follow-up study. Lancet.
354:197–202. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Braun S, Pantel K, Müller P, Janni W, Hepp
F, Kentenich CR, Gastroph S, Wischnik A, Dimpfl T, Kindermann G, et
al: Cytokeratin-positive cells in the bone marrow and survival of
patients with stage I II, or III breast cancer. N Engl J Med.
342:525–533. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bidard FC, Vincent-Salomon A, Gomme S, Nos
C, de Rycke Y, Thiery JP, Sigal-Zafrani B, Mignot L, Sastre-Garau X
and Pierga JY; Institut Curie Breast Cancer Study Group, :
Disseminated tumor cells of breast cancer patients: A strong
prognostic factor for distant and local relapse. Clin Cancer Res.
14:3306–3311. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Langer I, Guller U, Worni M, Berclaz G,
Singer G, Schaer G, Fehr MK, Hess T, Viehl C, Bronz L, et al: Bone
marrow micrometastases do not impact disease-free and overall
survival in early stage sentinel lymph node-negative breast cancer
patients. Ann Surg Oncol. 21:401–407. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hartkopf AD, Taran FA, Wallwiener M, Hahn
M, Becker S, Solomayer EF, Brucker SY, Fehm TN and Wallwiener D:
Prognostic relevance of disseminated tumour cells from the bone
marrow of early stage breast cancer patients-results from a large
single-centre analysis. Eur J Cancer. 50:2550–2559. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kamby C, Guldhammer B, Vejborg I, Rossing
N, Dirksen H, Daugaard S and Mouridsen HT: The presence of tumor
cells in bone marrow at the time of first recurrence of breast
cancer. Cancer. 60:1306–1312. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mukaiyama T, Ogawa M, Horikoshi N, Inoue
K, Inagaki J, Egaki K, et al: Analysis of metstatic behaviors and
causes of death in 100 autopsied patients with breast cancer. Jpn J
Breast Cancer. 4:121–126. 1989.(In Japanese).
|
|
16
|
Koida T, Kimura M, Ogawa A and Sugihara S:
A study of bone marrow on autopsied cases of breast
cancer-correlated to the hormone receptor. Jpn J Breast cancer.
6:567–570. 1991.(In Japanese).
|
|
17
|
Moriwaki S, Mandai K, Ohsumi S and Doihara
H: Metastasis to bone marrow in autopsy cases of breast
cancer-focal reactions to metastasis. Jpn J Cancer Clin.
47:389–400. 2001.(In Japanese).
|
|
18
|
Evangelista L, Panunzio A, Polverosi R,
Ferretti A, Chondrogiannis S, Pomerri F, Rubello D and Muzzio PC:
Early bone marrow metastasis detection: The additional value of
FDG-PET/CT vs. CT imaging. Biomed Pharmacother. 66:448–453. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lin CY, Chen YW, Chang CC, Yang WC, Huang
CJ and Hou MF: Bone metastasis versus bone marrow metastasis?
Integration of diagnosis by (18)F-fluorodeoxyglucose positron
emission/computed tomography in advanced malignancy with super bone
scan: Two case reports and literature review. Kaohsiung J Med Sci.
29:229–233. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Delsol G, Guiu-Godfrin B, Guiu M, Pris J,
Corberand J and Fabre J: Leukoerythroblastosis and cancer
frequency, prognosis, and physiopathologic significance. Cancer.
44:1009–1013. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yachida S, Jones S, Bozic I, Antal T,
Leary R, Fu B, Kamiyama M, Hruban RH, Eshleman JR, Nowak MA, et al:
Distant metastasis occurs late during the genetic evolution of
pancreatic cancer. Nature. 467:1114–1117. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Meric-Bernstam F, Frampton GM,
Ferrer-Lozano J, Yelensky R, Pérez-Fidalgo JA, Wang Y, Palmer GA,
Ross JS, Miller VA, Su X, et al: Concordance of genomic alterations
between primary and recurrent breast cancer. Mol Cancer Ther.
13:1382–1389. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Swanton C: Intratumor heterogeneity:
Evolution through space and time. Cancer Res. 72:4875–4882. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hilton JF, Amir E, Hopkins S, Nabavi M,
DiPrimio G, Sheikh A, Done SJ, Gianfelice D, Kanji F, Dent S, et
al: Acquisition of metastatic tissue from patients with bone
metastases from breast cancer. Breast Cancer Res Treat.
129:761–765. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bogina G, Bortesi L, Marconi M, Venturini
M, Lunardi G, Coati F, Massocco A, Manfrin E, Pegoraro C and
Zamboni G: Comparison of hormonal receptor and HER-2 status between
breast primary tumours and relapsing tumours: Clinical implications
of progesterone receptor loss. Virchows Arch. 459:1–10. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lindström LS, Karlsson E, Wilking UM,
Johansson U, Hartman J, Lidbrink EK, Hatschek T, Skoog L and Bergh
J: Clinically used breast cancer markers such as estrogen receptor,
progesterone receptor, and human epidermal growth factor receptor 2
are unstable throughout tumor progression. J Clin Oncol.
30:2601–2608. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Castaneda CA, Andrés E, Barcena C, Gómez
HL, Cortés-Funés H and Ciruelos E: Behaviour of breast cancer
molecular subtypes through tumour progression. Clin Transl Oncol.
14:481–485. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Simmons C, Miller N, Geddie W, Gianfelice
D, Oldfield M, Dranitsaris G and Clemons MJ: Does confirmatory
tumor biopsy alter the management of breast cancer patients with
distant metastases? Ann Oncol. 20:1499–1504. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Goldhirsch A, Winer EP, Coates AS, Gelber
RD, Piccart-Gebhart M, Thürlimann B and Senn HJ; Panel members, :
Personalizing the treatment of women with early breast cancer:
Highlights of the st gallen international expert consensus on the
primary therapy of early breast cancer 2013. Ann Oncol.
24:2206–2223. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Prat A, Cheang MC, Martín M, Parker JS,
Carrasco E, Caballero R, Tyldesley S, Gelmon K, Bernard PS, Nielsen
TO and Perou CM: Prognostic significance of progesterone
receptor-positive tumor cells within immunohistochemically defined
luminal A breast cancer. J Clin Oncol. 31:203–209. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lower EE, Glass EL, Bradley DA, Blau R and
Heffelfinger S: Impact of metastatic estrogen receptor and
progesterone receptor status on survival. Breast Cancer Res Treat.
90:65–70. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Guarneri V, Giovannelli S, Ficarra G,
Bettelli S, Maiorana A, Piacentini F, Barbieri E, Dieci MV, D'Amico
R, Jovic G and Conte P: Comparison of HER-2 and hormone receptor
expression in primary breast cancers and asynchronous paired
metastases: Impact on patient management. Oncologist. 13:838–844.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Broom RJ, Tang PA, Simmons C, Bordeleau L,
Mulligan AM, O'Malley FP, Miller N, Andrulis IL, Brenner DM and
Clemons MJ: Changes in estrogen receptor, progesterone receptor and
Her-2/neu status with time: Discordance rates between primary and
metastatic breast cancer. Anticancer Res. 29:1557–1562.
2009.PubMed/NCBI
|
|
34
|
Idirisinghe PK, Thike AA, Cheok PY, Tse
GM, Lui PC, Fook-Chong S, Wong NS and Tan PH: Hormone receptor and
c-ERBB2 status in distant metastatic and locally recurrent breast
cancer. Pathologic correlations and clinical significance. Am J
Clin Pathol. 133:416–429. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Sari E, Guler G, Hayran M, Gullu I,
Altundag K and Ozisik Y: Comparative study of the
immunohistochemical detection of hormone receptor status and HER-2
expression in primary and paired recurrent/metastatic lesions of
patients with breast cancer. Med Oncol. 28:57–63. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Yumimoto K, Akiyoshi S, Ueo H, Sagara Y,
Onoyama I, Ueo H, Ohno S, Mori M, Mimori K and Nakayama KI: F-box
protein FBXW7 inhibits cancer metastasis in a non-cell-autonomous
manner. J Clin Invest. 125:621–635. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Takeishi S and Nakayama KI: Role of Fbxw7
in the maintenance of normal stem cells and cancer-initiating
cells. Br J Cancer. 111:1054–1059. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Rahim F, Hajizamani S, Mortaz E,
Ahmadzadeh A, Shahjahani M, Shahrabi S and Saki N: Molecular
regulation of bone marrow metastasis in prostate and breast cancer.
Bone Marrow Res. 2014:4059202014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Greene FL: Breast tumoursTNM
classification of malignant tumours. 7th. Sobin LH, Gospodarowicz
MK and Wittekind C: Wiley-Blackwell; Oxford: pp. 181–193. 2009
|