Introduction
Mucinous adenocarcinoma of the prostate is a rare
morphological variant of prostate cancer, which is defined by the
presence of extravasated mucin in >25% of the tumor volume
(1,2). Of all prostate cancer types, the
incidence of this rare malignancy is ~0.2% (3). The overall incidence of prostate cancer
diagnosis following transurethral resection of the prostate (TURP)
has sharply decreased following introduction of PSA screening
(4). Mucinous carcinoma of the
prostate differs from secondary prostatic involvement by mucinous
adenocarcinomas arising in other sites, such as the rectum or
bladder, in terms of typical morphology and cytological
characteristics (5). However, the
primary origin of less well-differentiated tumors may be difficult
to identify. Negative staining for PSA may help differentiate
between primary and secondary tumors; however, PSA staining in
undifferentiated prostatic cancer may also be negative (6), and is therefore unreliable.
To the best of our knowledge, mucinous
adenocarcinoma of the prostate incidentally identified in specimens
obtained via TURP has not yet been reported in any previous study.
The present study reported two cases of mucinous adenocarcinoma
that were incidentally identified following TURP. The clinical
progression of the disease, in addition to the treatment options
and prognostic factors, were also reviewed.
Case studies
Case 1
A 67-year-old man was admitted to Zhongda Hospital
(Nanjing, China) with edema of the bilateral lower extremities for
a total of 6months in July, 2015. In the local hospital (Muyang
County Hospital, Suqian, China), the patient was diagnosed with
bilateral hydronephrosis and bilateral ureteral colic on urologic
ultrasound examination. A pelvic computed tomography (CT) scan
revealed an enlarged prostate and a focal thickening of the bladder
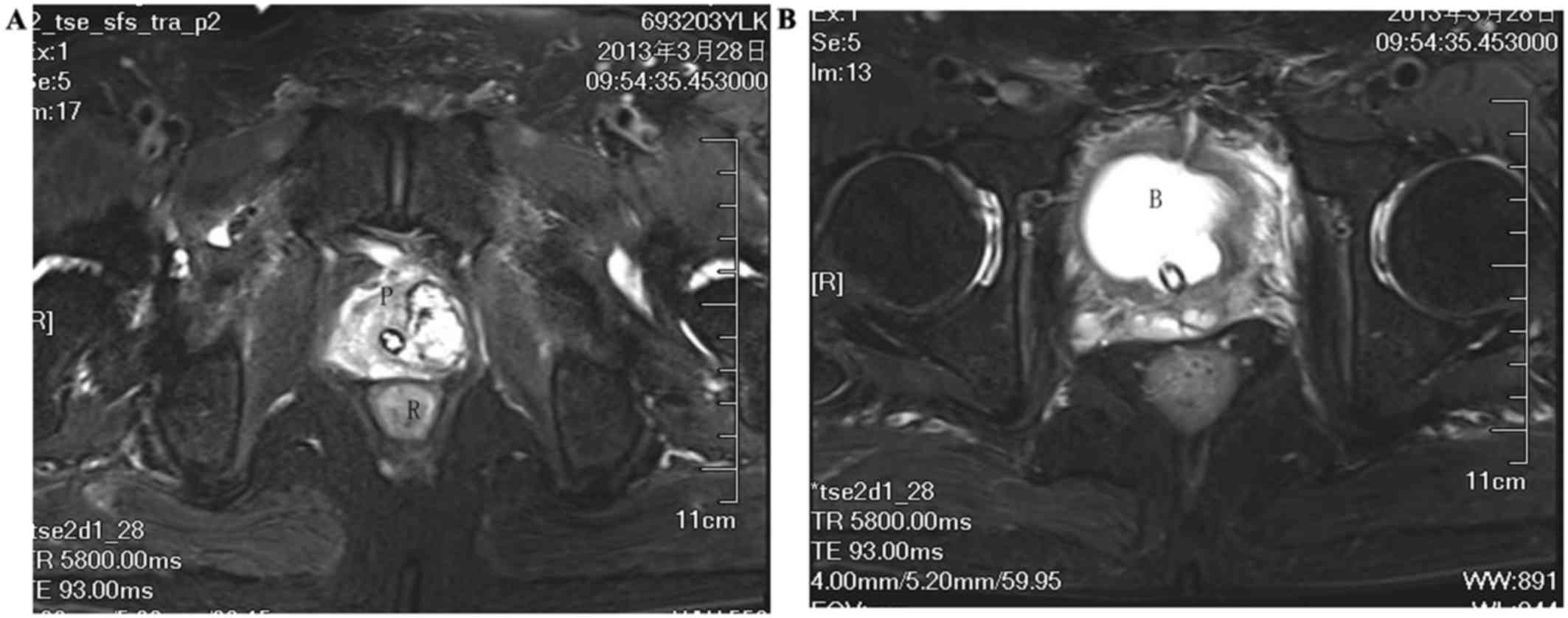
wall. Magnetic resonance imaging examination revealed that the
tumor had invaded the prostatic capsule (Fig. 1A), with possible bladder wall
invasion (Fig. 1B). The results of
the laboratory tests were as follows: Blood urea nitrogen, 21.7
mmol/l; creatinine, 634 µmol/l; carcinoembryonic antigen (CEA), 8.3
ng/ml; and prostate-specific antigen (PSA), 4.2 mg/ml. The patient
underwent cystoscopy to evaluate the focal thickening of the
bladder wall, and TURP for the enlarged prostate, in addition to an
ultrasound-guided bilateral percutaneous nephrostomy to decompress
the upper urinary system and relieve the hydronephrosis. On
histological examination of the TURP specimen, prostatic
adenocarcinoma and mucinous adenocarcinoma were identified. The
biopsy of the bladder wall thickening was inconclusive. A
radionuclide bone scan was negative for metastasis. Three weeks
later, the patient underwent radical cystoprostatectomy with
bilateral pelvic lymphadenectomy and bilateral ureterostomy.
Pathological examination of the surgically obtained specimen
confirmed the diagnosis of prostatic adenocarcinoma with a Gleason
score of 4+5=9/10,which was the same as the Gleason score of the
TURP sample. The mucinous carcinomatous component comprised 25% of
the tumor. Tumor invasion was observed in the peri-prostatic
adipose tissue, bilateral seminal vesicles, all layers of the
bladder wall and the surgical margins of the prostate-bladder neck.
All pelvic lymph nodes were negative for tumor involvement (6 lymph
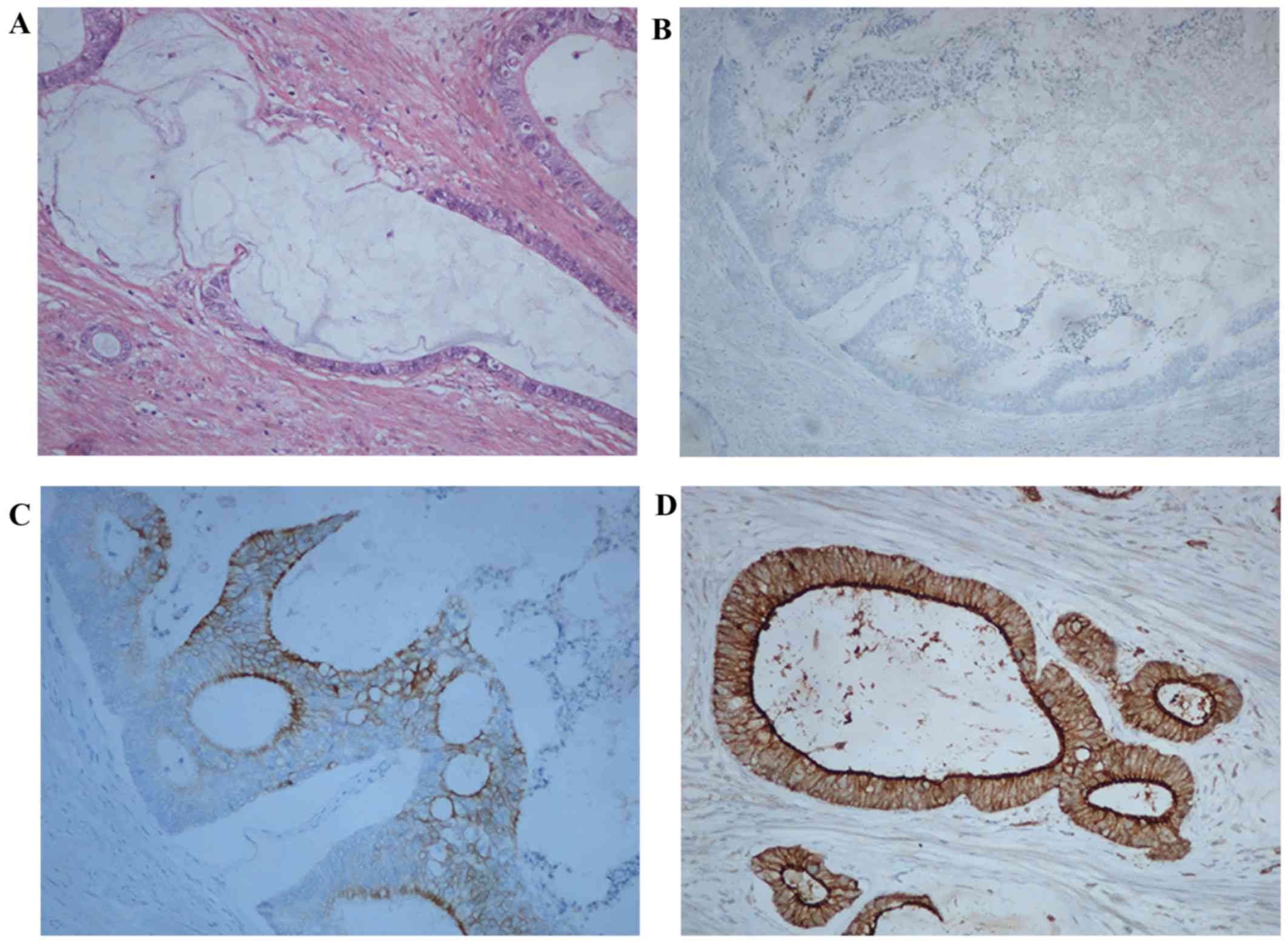
nodes on the left and 9 on the right side). On immunohistochemical
examination, the tumor stained positive for cytokeratin (CK)20,
CEA, Ki-67 (20%) and β-catenin, and negative for CK7, androgen
receptor (AR), prostate-specific membrane antigen (PSMA) and PSA
(Fig. 2). Postoperatively, the
patient underwent adjuvant androgen deprivation therapy (ADT) with
bicalutamide 150 mg per day and goserelin 3.6 mg every 4 weeks for
1 year, and the total PSA level remained constant at <0.003
ng/ml during that time. The follow-up bone scan was negative for
tumor metastasis. At 1.5 years after surgery, an abdominal CT scan
revealed multiple metastatic lesions in the peritoneum and a
positron emission tomography (PET) scan revealed metastatic lesions
to the pelvic bones and the right femur. The serum CEA levels had
increased to 221.6 ng/ml and total PSA remained at <0.003 ng/ml.
The serum testosterone levels were <5 ng/dl. The patient
subsequently underwent localized radiotherapy for bone metastasis.
The total dose of the radiotherapy was 20 Gy (40 Gy/fraction) and
the metastatic lesions reduced in size following the treatment.
Chemotherapy was not considered to be an option due to the
patient's underlying congestive cardiac failure. The patient has
been on palliative care with pain control. The last follow-up of
the patient was in December 2017, and the patient was in a stable
condition.
Case 2
A 70-year-old man who underwent TURP at a local
hospital 6 weeks earlier was admitted to Zhongda Hospital in
September 2014. The patient's preoperative serum PSA level was 0.95
ng/ml. A pathological examination of the TURP specimen revealed
mucinous adenocarcinoma of the prostate, with a Gleason score of
4+4=8/10. A total of 100% of the tumor mass was mucinous carcinoma.
A PET scan revealed no bone metastases. Subsequently, the patient
underwent radical prostatectomy and bilateral pelvic
lymphadenectomy. Histological examination of the surgical specimens
revealed mucinous adenocarcinoma in the left lobe of the prostate,
with a Gleason score of 8. The surgical margins, seminal vesicles
and pelvic lymph nodes (7 lymph nodes on the left and 3 on the
right side) were all negative for tumor involvement.
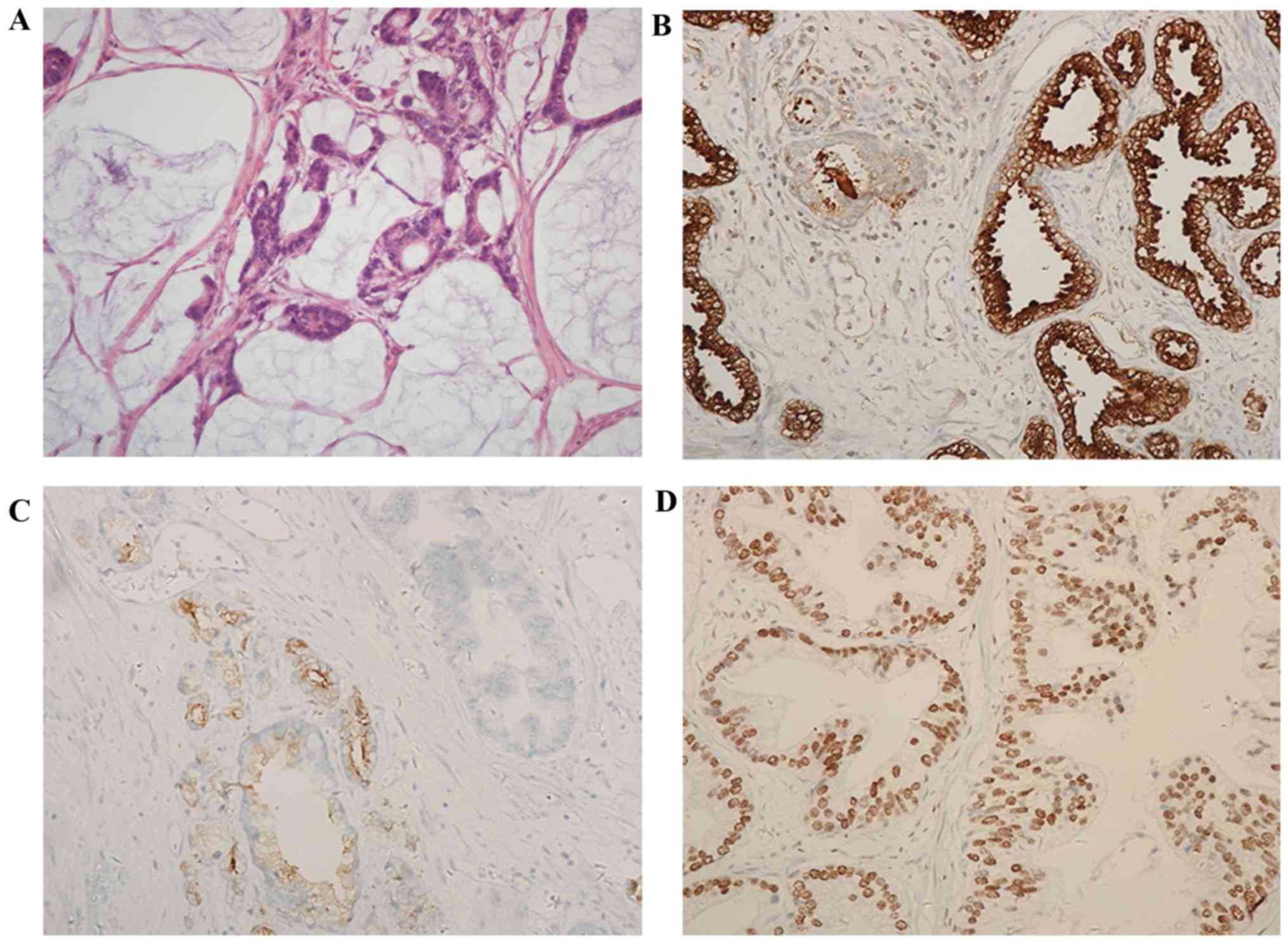
Immunohistochemical examination revealed positive staining for PSA,
PSMA, CK7 (weakly positive), Ki-67 (2%), tumor protein p53, human
epidermal growth factor receptor 2 (HER2), AR, epidermal growth
factor receptor (EGFR), multiple drug resistance (MDR), CD34, D2-40
and S-100, whereas the tumor was negative for CEA, estrogen
receptor, progesterone receptor, p63 and B-cell lymphoma 2
(Fig. 3). Postoperatively, the
patient received ADT with bicalutamide 150 mg per day and goserelin
3.6 mg every 4 weeks for 1.5 years; he was then followed up for 3
years and exhibited no signs of tumor recurrence or metastasis
during that time. On the most recent follow-up in January 2018, the
serum PSA level was<0.003 ng/ml and the serum testosterone level
was<0.1 ng/dl. The patient has a follow-up every 6 months with
no further treatment at present.
Discussion
The incidence of prostate cancer diagnosis following
TURP ranged between 8 and 18% prior to the introduction of PSA
screening, and decreased to 8% thereafter (4). Mucinous carcinoma in TURP specimens is
extremely rare and, to the best of our knowledge, has not been
previously reported. We herein report two cases of mucinous
carcinoma of the prostate diagnosed following TURP, with totally
different clinical courses.
Mucinous carcinoma of the prostate is distinctly
different from the secondary prostatic involvement by mucinous
adenocarcinomas arising elsewhere (usually the rectum or bladder).
The presence of typical acinar prostatic adenocarcinoma morphology
and the cytological characteristics of the tumor often distinguish
it from other malignancies in the majority of the cases (5). However, for less well-differentiated or
undifferentiated tumors, the identification of their primary origin
may be difficult. It has been proposed that negative staining for
PSA in the tumor cells may help differentiate between primary and
secondary tumors; however, PSA staining in undifferentiated
prostatic cancer may also be negative (6), which makes this criterion unreliable. A
number of alternative tumor markers have also been used in an
attempt to distinguish the origin of the mucinous cancer of the
prostate. Bassily et al (7)
reported that the double-positive staining for CK7 and CK20 in the
tumor cells may help distinguish urothelial from prostatic cancer;
however, single-positive or double-negative staining for these two
markers is of limited value. Furuta et al (8) reviewed 32 cases of mucinous
adenocarcinoma of the prostate, and concluded that there were two
subtypes: One that stains positive for PSA, which is a subtype of
conventional adenocarcinoma, and another that stains positive for
CEA and negative for PSA, which is derived from intestinal
metaplasia with atypia of the prostatic urethra. In the present
study, the surgical specimen from the first patient was negative
for PSA and CK7, but positive for CK20 and CEA, and was confirmed
to be a primary prostatic adenocarcinoma with bladder metastasis.
However, in the second case, which was confirmed to be an
organ-confined adenocarcinoma, the tumor stained positive for PSA
and CK7, in addition to several other tumor markers, including
Ki-67, p53, HER2, AR, EGFR and MDR. In the present study, PSA and
CK7 staining alone are not considered reliable for the
identification of the origin of mucinous adenocarcinoma of the
prostate.
It was previously reported that the PSA levels in
mucinous adenocarcinoma are comparable to those in non-mucinous
tumor types (1,3). However, in the present study, the PSA
levels were substantially lower in patients with mucinous
carcinoma: In the first case, a cT4 prostate cancer with bladder
metastasis, the serum total PSA levels were 4.2 ng/ml, whereas in
the second case, a pT2 prostate cancer, the PSA levels were 0.75
ng/ml. Taking into consideration the fact that mucinous carcinoma
comprised 25% of the tumor mass in the first case and 100% in the
second case, it may be hypothesized that a higher percentage of
mucinous content in the tumor may be associated with a lower level
of serum PSA. In clinical practice, an elevated PSA level is
currently one of the major indicators for a prostate biopsy.
Therefore, a normal or only slight increase in PSA levels in
patients with mucinous carcinoma may result in omitting biopsy,
thereby not diagnosing the tumor at an early stage.
The prognosis of mucinous carcinoma of the prostate
remains controversial. It has been reported that the
characteristics of mucinous adenocarcinoma of the prostate do not
differ significantly from those of normal acinar adenocarcinoma in
the clinical setting (9). The two
types of tumors display similar biological behaviors, including PSA
production and a propensity to develop bone metastases with
advanced disease. In a series of 47 cases, the prognosis for
mucinous adenocarcinoma of the prostate treated by radical
prostatectomy is similar or better compared with nonmucinous
adenocarcinoma (10). However, a
more aggressive clinical course and a worse prognosis have also
been reported in other previous studies (10,11). In
the present study, the two patients exhibited low levels of PSA
during the course of ADT, which indicated a hormone responsiveness
similar to conventional prostate adenocarcinoma; whereas worse
outcome, in terms of recurrence and aggression, was associated with
a higher Gleason score and positive surgical margins. In the
organ-confined prostate cancer, mucinous adenocarcinoma treated by
radical prostatectomy is potentially less aggressive compared with
non-mucinous adenocarcinoma. However, routine adjuvant ADT may be
problematic, as patients with mucinous adenocarcinoma of the
prostate may have a variable outcome in terms of hormone
responsiveness and recurrence (2). A
negative expression of PSA in the surgical specimens may also
predict a poor response to ADT; however, this hypothesis requires
further confirmation through a well-designed prospective study with
a larger patient population.
In conclusion, the clinical progression of mucinous
adenocarcinoma of the prostate following TURP is similar to that of
acinar prostate adenocarcinoma, depending on the Gleason score,
focal involvement and surgical margins. The quantity of mucin
present in the prostatectomy specimen appears to be inversely
correlated with PSA levels, which may result in a delayed prostatic
biopsy and diagnosis of this disease. Absence of PSA staining in
the surgical specimen may be associated with poor response to
ADT.
Acknowledgements
The authors would like to thank the staff of the
Departments of Urology and Pathology at Zhongda Hospital for the
technical support of this study.
Funding
No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
QF and MC designed the study. LijZ and LihZ
collected the data. QF wrote the manuscript and approved the final
version of the manuscript to be published.
Ethics approval and consent to
participate
All procedures performed were in accordance with the
ethical standards of the authors' Institutional Research
Committee.
Patient consent for publication
Informed consent was obtained from the patients
involved in the study regarding the publication of the case details
and associated images.
Competing interests
All authors declare that they have no competing
interests regarding the design or conduct of the present study.
References
|
1
|
Epstein JI and Lieberman PH: Mucinous
adenocarcinoma of the prostate gland. Am J Surg Pathol. 9:299–308.
1985. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Osunkoya AO and Epstein JI: Primary
mucin-producing urothelial-type adenocarcinoma of prostate: Report
of 15 cases. Am J Surg Pathol. 31:1323–1329. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ro JY, Grignon DJ, Ayala AG, Fernandez PL,
Ordonez NG and Wishnow KI: Mucinous adenocarcinoma of the prostate:
Histochemical and immunohistochemical studies. Hum Pathol.
21:593–600. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tombal B, De Visccher L, Cosyns JP, Lorge
F, Opsomer R, Wese FX and Van Cangh PJ: Assessing the risk of
unsuspected prostate cancer in patients with benign prostatic
hypertrophy: A 13-year retrospective study of the incidence and
natural history of T1a-T1b prostate cancers. BJU Int. 84:1015–1020.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tran TA, Jennings TA, Ross JS and Nazeer
T: Pseudomyxoma ovariilike posttherapeutic alteration in prostatic
adenocarcinoma: A distinctive pattern in patients receiving
neoadjuvant androgen ablation therapy. Am J Surg Pathol.
22:347–354. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Helpap B and Köllermann J:
Undifferentiated carcinoma of the prostate with small cell
features: Immunohistochemical subtyping and reflections on
histogenesis. Virchows Arch. 434:385–391. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bassily NH, Vallorosi CJ, Akdas G, Montie
JE and Rubin MA: Coordinate expression of cytokeratins 7 and 20 in
prostate adenocarcinoma and bladder urothelial carcinoma. Am J Clin
Pathol. 113:383–388. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Furuta A, Naruoka T, Hasegawa N, Suzuki Y,
Ikemoto I and Oishi Y: Mucinous adenocarcinoma of the prostate: A
case report and review of 32 cases on immunohistochemical study of
both PSA and CEA. Nippon Hinyokika Gakkai Zasshi. 94:570–573.
2003.(In Chinese). PubMed/NCBI
|
|
9
|
Rhee AC, Olgac S, Ohori M and Russo P:
Mucinous adenocarcinoma of the prostate: A case report of long-term
disease-free survival and a review of the literature. Urology.
63:779–780. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Osunkoya AO, Nielsen ME and Epstein JI:
Prognosis of mucinous adenocarcinoma of the prostate treated by
radical prostatectomy: A study of 47 cases. Am J Surg Pathol.
32:468–472. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Manne RK and Haddad FS: Mucinous
adenocarcinoma of prostate. Urology. 33:247–249. 1989. View Article : Google Scholar : PubMed/NCBI
|