Introduction
Intra-articular primary soft tissue sarcomas are
extremely rare. In the few cases that have been published, it
mostly arose in the knee joint of adults, with the most common type
being synovial sarcoma (1–3). Synovial sarcoma accounts for 5 to 10%
of soft tissue sarcomas and typically occurs in patients between 15
and 35 years (4). Synovial sarcoma
is unrelated to the synovium, and less than 5% cases originate
within a joint (1,4), which mostly occurs in the knee joint
(1–3). Yet, other locations have been reported,
with three cases involving the elbow and one involving the hip
joint (1). Furthermore, one case of
intra-articular synovial sarcoma at the ankle joint was described
in a previous report in which the magnetic resonance imaging (MRI)
features of 12 synovial sarcomas were reviewed; however, this
report provided no detailed clinical information (5). In this report, we describe a case of
intra-articular synovial sarcoma of the right ankle joint in a
51-year-old man. The requirement for institutional review board
approval of our institute was waived owing to the anonymized and
retrospective nature of this report, but we obtained written
informed consent to perform future studies from the patient.
Case report
A 51-year-old man was referred to out hospital due
to swelling and progressive pain in the right ankle that was
present for 2 months. There was no history of trauma, and his
medical history was otherwise unremarkable. Physical examination of
his right ankle revealed a painful yet nearly full range of motion
as well as tenderness, particularly on the anterior part of the
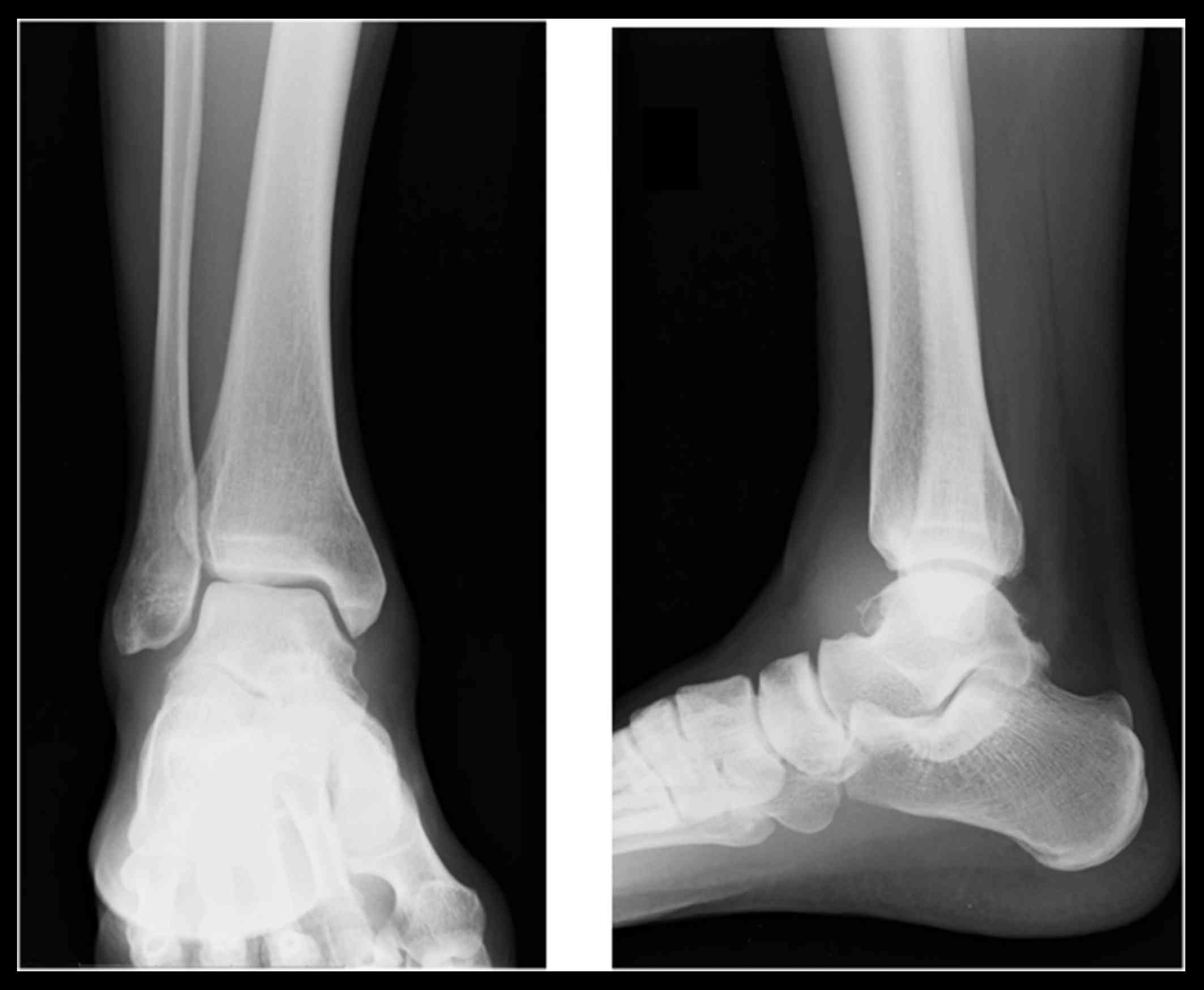
ankle joint. Lateral radiographs of the ankle revealed lytic change
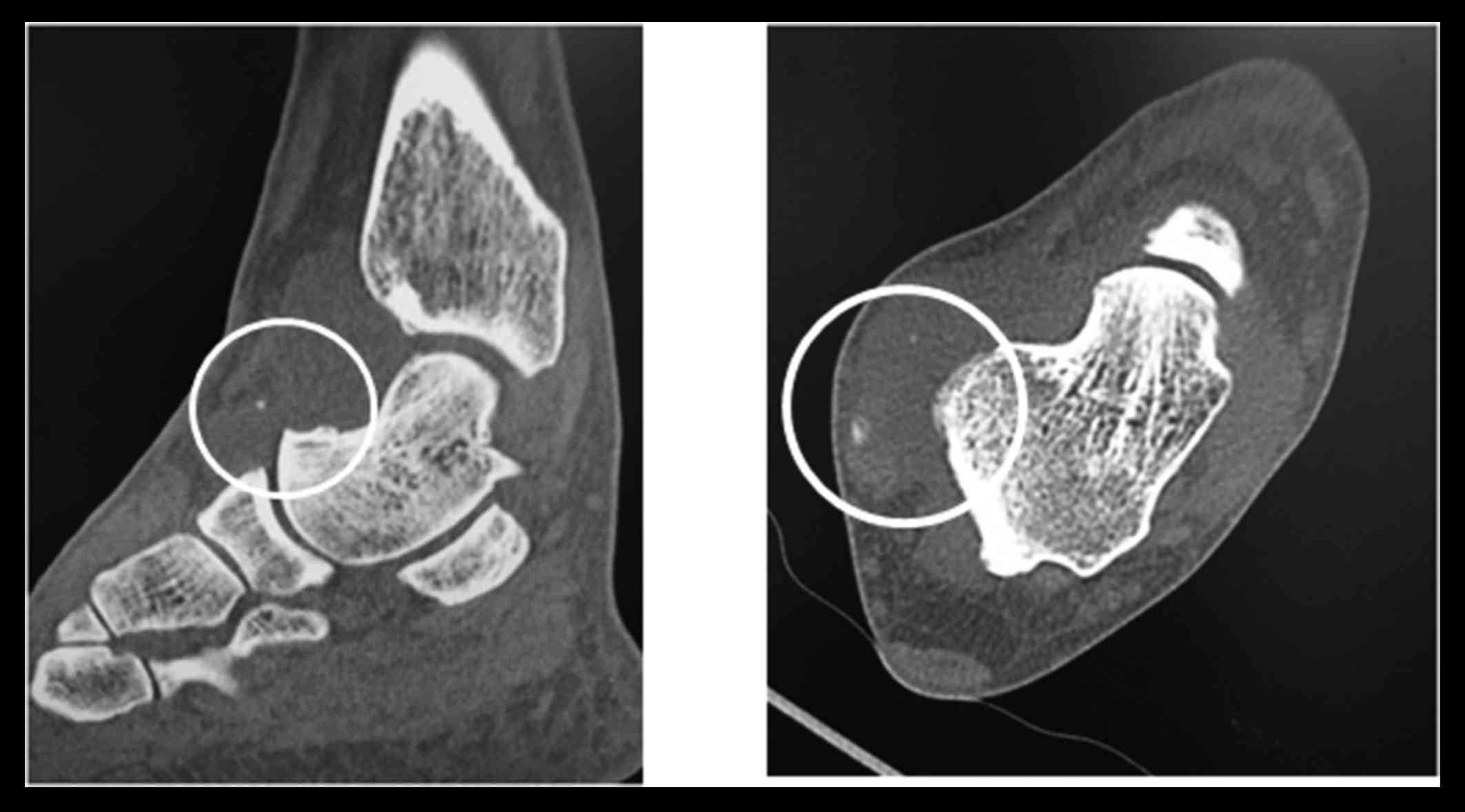
of the anterior and posterior parts of the talus (Fig. 1). Computed tomography (CT) imaging
revealed a low-density lesion with calcifications around the ankle
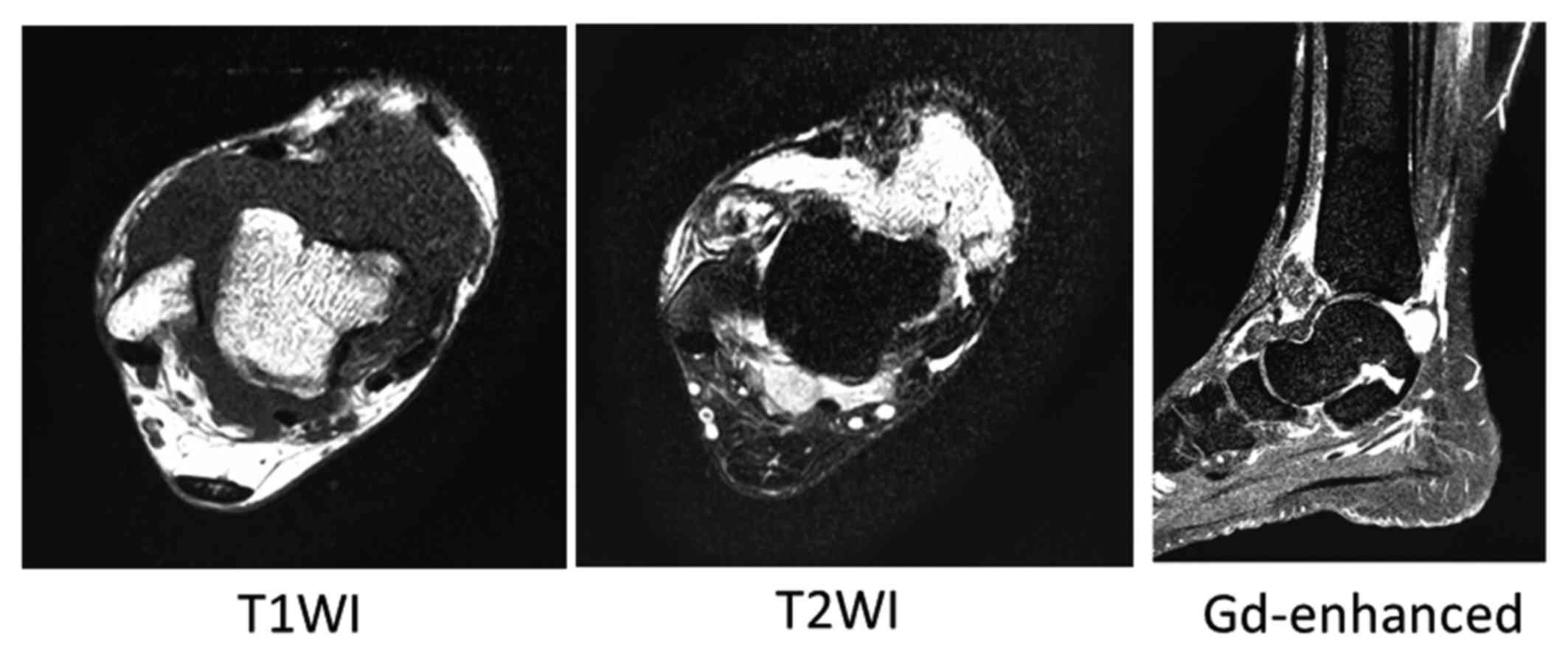
joint (Fig. 2). MRI indicated that
the diffuse lesion was isointense on T1-weighted images and
hypointense to hyperintense on T2-weighted images. After
administration of gadolinium-containing contrast medium, the tumor
revealed heterogeneous enhancement (Fig.
3). Open biopsy was performed. Histological findings revealed a
monophasic malignancy composed of spindle cells.
Immunohistochemically, the tumor was positive for BCL2 and
CD99/MIC2 and focally positive for epithelial membrane antigen and
α smooth muscle actin, but negative for desmin, CD34, and
cytokeratins. The aforementioned morphologic and
immunohistochemical findings were consistent with monophasic
synovial sarcoma. The foot could not be salvaged because the
sarcoma was diffusely spread throughout the ankle joint; thus, the
patient underwent below-knee amputation with neoadjuvant (three
courses) and adjuvant (two courses) chemotherapy using gemcitabine
and docetaxel. After rehabilitation, he used a below-the-knee
prosthesis and walked without any need for support. One year after
the initial treatment, lymph node metastasis at the popliteal
vasculature and thigh developed. Therefore, above-knee amputation
with adjuvant chemotherapy using adriamycin and ifosfamide was
performed. However, multiple lung metastases developed after 3
months. He had started chemotherapy using eribulin, but he suddenly
died from fatal arrhythmia, which were not related to eribulin, 2
years after the initial diagnosis.
Discussion
Synovial sarcoma accounts for 5 to 10% of all
primary soft tissue sarcomas (4).
Despite its name, whether synovial sarcoma develops directly from
synovial tissue is unclear (4).
Approximately 5% of cases have been estimated to be intra-articular
(1,4). However, previous reports concerning
synovial sarcoma suggest that intra-articular cases may be less
common than originally thought (1,6). Most
cases of intra-articular synovial sarcoma originate in the knee
joint. However, other locations have been reported, including one
previously reported case involving intra-articular synovial sarcoma
of the ankle (5), but no detailed
clinical characteristics, such as tumor size, patient age,
treatment method, and clinical course, were provided. Therefore,
our case is the first reported case of intra-articular synovial
sarcoma at the ankle whose clinical course has been described in
detail. When intra-articular tumors are found, benign soft-tissue
tumors, such as pigmented villonodular synovitis (PVNS) and
synovial osteochondromatosis, are more frequently considered as
differential diagnoses than synovial sarcoma. In our case,
calcification was observed during a CT scan. Calcification is an
extremely rare phenomenon in PVNS (3,7,8), whereas ~30% of cases involving synovial
sarcoma exhibit calcification (9).
On MRI, differentiating intra-articular synovial sarcoma from
benign tumors is difficult and no certain radiological features
have been established. Nordemar et al (3) reported that moderate and large amounts
of joint effusion were only found in PVNS when they compared PNVS
with synovial sarcoma. In the present case, the volume of joint
effusion was low. However, other findings, such as extra-articular
growth, low signal intensity in the synovia, and synovitis, were
not significant variables on predicting synovial sarcoma (3). Synovial osteochondromatosis is also a
rare joint disorder that is more rarely observed in the foot and
ankle (10,11). It is usually monoarticular and occurs
most commonly in larger joints, with >50% of the cases occurring
in the knee (10,11). Therefore, biopsy is often necessary
to diagnose the patient, as described in the present case. We
initially performed below-knee amputation, given the diffuse spread
of the sarcoma throughout the ankle joint, which indicated that the
foot could not be salvaged. We found five cases of intra-articular
ankle soft tissue sarcomas in the literature (12,13),
including one case of extraskeletal myxoid chondrosarcoma and four
cases of synovial chondrosarcomas. Amputation was performed in all
five cases. Although limb salvage tumor resection was performed in
patients with intra-articular soft tissue sarcoma at the knee joint
(1–3), amputation may be necessary to resect
the tumor completely due to widely diffused spread of the tumor. In
conclusion, we experienced a case of intra-articular synovial
sarcoma at the ankle joint. Although intra-articular primary soft
tissue sarcomas are extremely rare, the possibility of malignancy
should be considered. Moreover, when the tumor is widely spread,
amputation may be performed to establish a clear surgical
margin.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
TN conceived the study, treated the patients,
collected the data and wrote the manuscript. TH collected, analyzed
and interpreted the clinical data. KA performed surgery, and
analyzed and interpreted the clinical data. AS analyzed and
interpreted the clinical data, and reviewed the manuscript.
Ethics approval and consent to
participate
The requirement for institutional review board
approval from our institute was waived owing to the anonymized and
retrospective nature of this report; however, written informed
consent was obtained from the patient to perform further
studies.
Patient consent for publication
Written informed consent was obtained from the
patient to perform further studies.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Friedman MV, Kyriakos M, Matava MJ,
McDonald DJ, Jennings JW and Wessell DE: Intra-articular synovial
sarcoma. Skeletal Radiol. 42:859–867. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chebib I, Rosenberg AE, Fletcher CDM,
Rosenthal DI, Hornicek FJ and Nielsen GP: Primary intra-articular
sarcoma: A clinicopathological study of 15 cases. Histopathology.
69:614–623. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nordemar D, Öberg J, Brosjö O and Skorpil
M: Intra-articular synovial sarcomas: Incident and differentiating
features from localized pigmented villonodular synovitis. Sarcoma.
2015:9038732015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Weiss SW and Goldblum JR: Enzinger and
Weiss's soft tissue tumors. 5th. Elsevier; St Louis: pp. 1161–1182.
2008
|
|
5
|
Morton MJ, Berquist TH, McLeod RA, Unni KK
and Sim FH: MR imaging of synovial sarcoma. AJR Am J Roentgenol.
156:337–340. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cadman NL, Soule EH and Kelly PJ: Synovial
sarcoma: An analysis of 134 tumors. Cancer. 18:613–627. 1965.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Murphry MD, Rhee JH, Fanburg-Smith LJC,
Flemming DJ and Walker EA: From the archives of the AFIP pigmented
villonodular synovitis: Radiologic-pathologic correlation.
Radiographics. 28:1493–1518. 2009. View Article : Google Scholar
|
|
8
|
Oda Y, Izumi T, Harimaya K, Segawa Y,
Ishihara S, Komune S, Iwamoto Y and Tsuneyoshi M: Pigmented
villonodular synovitis with chondroid metaplasia, resembling
chondroblastoma of the bone: A report of three cases. Mod Pathol.
20:545–551. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bui-Mansfield LT and O'Brien SD: Magnetic
resonance appearance of intra-articular synovial sarcoma: Case
reports and review of the literature. J Comput Assist Tomogr.
32:640–644. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Saxena A and St Louis M: Synovial
chondromatosis of the ankle: Report of two cases with 23 and 126
loose bodies. J Foot Ankle Surg. 56:182–186. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Derek Stensby J, Fox MG, Kwon MS, Cavcedo
FJ and Rahimi A: Primary synovial chondromatosis of subtalar joint:
Case report and review of the literature. Skeletal Radiol.
47:391–396. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bhamra JS, Alorjani M, Skinner JA and
Saifuddin A: Intra-articular extraskeletal myxoid chondrosarcoma of
the ankle. Skeletal Radiol. 41:1017–1020. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Biazzo A and Confalonieri N: Synovial
chondrosarcoma. Ann Transl Med. 4:2802016. View Article : Google Scholar : PubMed/NCBI
|