Introduction
Older men usually have a shorter life expectancy, a
higher risk of competing causes of mortality, and a greater risk of
potential harm from screening for prostate cancer (PCa) (1). It is evident that there is an
increasing proportion of individuals aged 70 years and older, as
well as an increasing life expectancy worldwide (2). The life expectancy of men aged 70 years
old in America is estimated to be 14 years compared with 15 years
in Japan (3). The American
Urological Association does not recommend routine prostate-specific
antigen (PSA) screening in men >70 years old or any man with
less than a 10–15 year life expectancy (4). In Japan, however, there is no clear
consensus among urologists on how to manage older men aged 70 years
and older with elevated PSA.
The classical risk factors for PCa include elevating
PSA and positive digital rectal examination (DRE). The current
standard of care practice for a diagnosis of PCa is a needle biopsy
of the prostate (PBx) (5). However,
a number of criticisms have been directed against PSA-based
screening for PCa, which lead to overdiagnosis and overtreatment in
certain cases (6). Recent screening
guidelines do not recommend PSA screening alone, especially in
older men (7). The risks of PBx
include pain, urinary retention, hematuria, hemospermia, and, most
significantly, urinary tract infection (UTI). The reported
incidence for UTIs is 2–6%, and for severe sepsis is 0.2–2%
(8). Therefore, other approaches may
be necessary to prevent unnecessary biopsies, especially for older
men.
Prediction methods were developed to reduce
unnecessary biopsies, to avoid false-negative biopsies while still
detecting most clinically important PCa cases before biopsy
(9). These are more accurate than
PSA screening alone. An ideal predictive tool would be a reliable
imaging method that excludes inter-observer variability such as in
DRE and transrectal ultrasound (TRUS) prostate images.
Multiparametric magnetic resonance imaging (mpMRI) is now widely
used in diagnosis, staging after diagnosis, and treatment planning
of PCa (10–12). We reported previously that MRI
positivity can independently predict biochemical recurrence after
radical prostatectomy (13).
Recently, the European Society of Urogenital Radiology (ESUR)
proposed the Prostate Imaging Reporting and Data System (PI-RADS)
to detect PCa (14). In addition to
imaging, we reported that PSA density is also useful for
distinguishing benign prostatic hypertrophy and PCa (13,15).
The aim of the present study was to evaluate the
role of PSA density after mpMRI before PBx, especially for older
men, to avoid overscreening, overdiagnosis, and overtreatment.
Patients and methods
Study design
The medical records of 241 patients aged >70
years who underwent mpMRI before PBx at our institution between
January 2012 and December 2016 were reviewed retrospectively in
this study. Exclusion criteria was serum PSA level >20 ng/ml.
Multiple variables were evaluated as predictors for the diagnosis
of PCa. The variables and indications for biopsy included serum PSA
level, DRE, size of region of interest (ROI) on mpMRI, prostate
volume, and PSA density.
Imaging
At our institution, the mpMRI system is a 3.0-Tesla
scanner (Signa Excite XI 1.5 and 3.0-Tesla, 32-channel torso-array
coil). T2-weighted fast spin-echo imaging (T2WI, 3000/120, 4 NEX, 4
min 36 sec, 3.4 mm slice, 0 mm space), diffused-weighted imaging
(DWI, single-shot diffusion echo plannar imaging, b=0, 2,000
sec/min2 for whole pelvic, 0, 1,500 sec/min2
for prostate, 4000/69.5 (pelvis), 4000/58.3 (prostate), 1 min 24
sec, 3 min 24 sec), and Gadolinium-dynamic contrast enhanced MRI
(DCE, liver imaging with Volume Acceleration-flexible (LAVA-Flex),
4/1.1/12°, 15 sec, 40, 60, and 180 sec after i.v.) were performed.
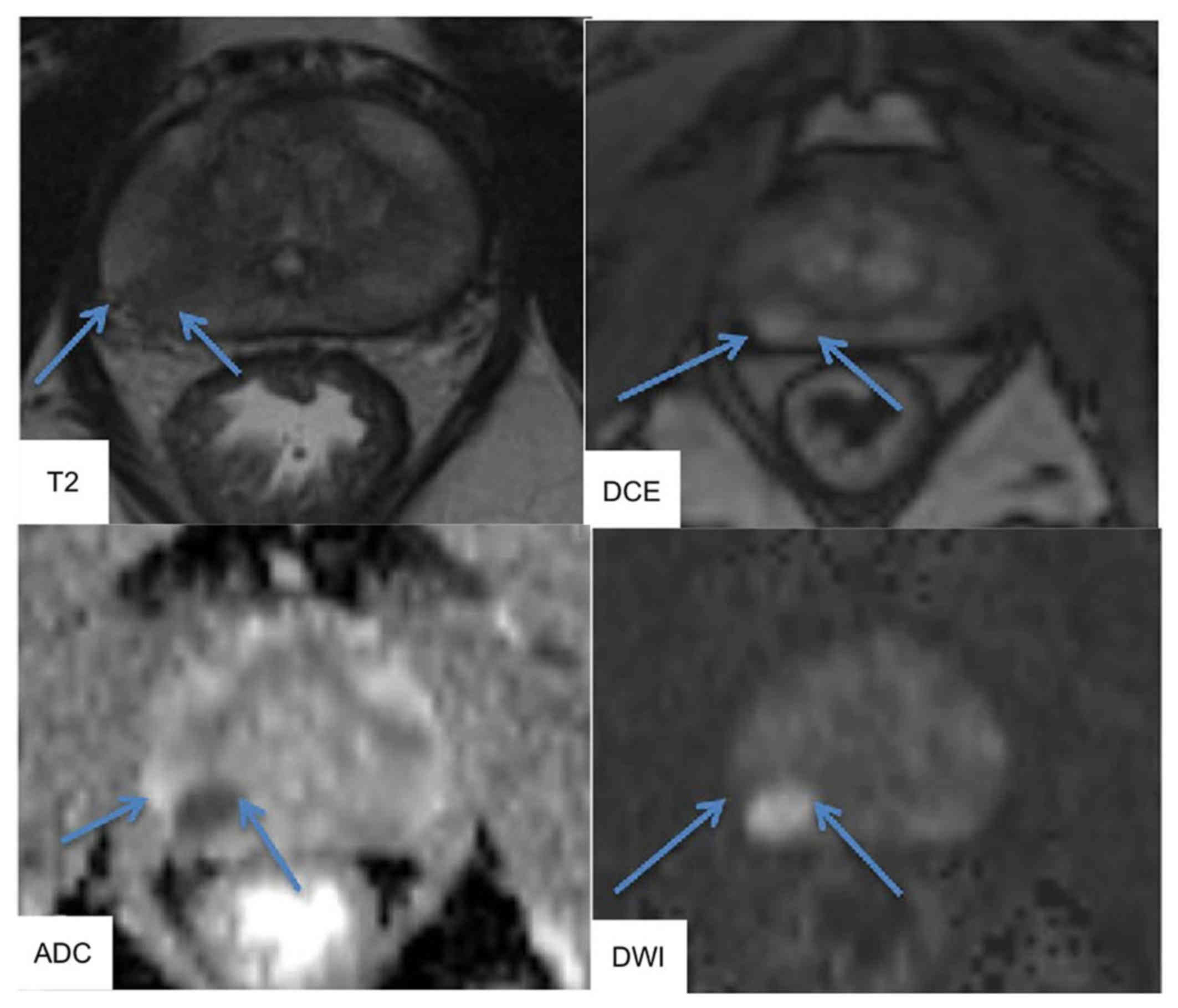
MRI could identify ROIs, and MR images were interpreted by
experienced radiologists in accordance with ESUR PI-RADS v2.0. The
typical images of mpMRI were shown in Fig. 1. T2WI was used for prostate cancer
detection, localization and imaging. T2WI alone was sensitive but
not specific for PCa and should be improved using DCE and DWI MRI.
DWI allowed apparent diffusion coefficient (ADC) maps to be
calculated, enabling qualitative and quantitative assessment of PCa
aggressiveness.
Biopsy
All patients underwent TRUS-guided systematic
biopsies of 12 cores that included lateral and mid lobar cores at
the base, middle, and apex of each prostate lobes. All biopsy
specimens were interpreted histopathologically by experienced
pathologists according to the recommendations of the International
Society of Urological Pathology (ISUP). Clinical significant PCa
was defined as Gleason score ≥4+3=7. We compared the MRI findings
with the pathological findings retrospectively. At least one
positive area on biopsy matched with each MRI lesion suspicious for
cancer and vice versa were defined as matched. The absence of areas
with pathological reports matching each MRI lesion was defined as
unmatched.
Data analysis
Prostate volume in this study was measured in axial
and sagittal images (height × width × depth/2) using both TRUS and
MRI. PSA density was calculated by dividing serum PSA levels by
prostate volume. Prostate volumes in TRUS were calculated by each
urologist. All prostate volumes in MRI were calculated by one
author. The factors evaluated for PBx included age, serum PSA
level, index tumor size of ROI on MRI, prostate volume, and PSA
density.
Statistical analysis
Statistical analyses were performed using the R
Statistical Language version 3.0.2 and the SPSS version 23.0
statistical software packages. Chi-squared test was used to test
the distribution of categorical variables, and the Mann-Whitney U
test was used for continuous variables. We calculated the best-fit
receiver operating characteristic (ROC) curve and the corresponding
area under the ROC curve (AUC) estimates and 95% confidence
interval (CI), then calculated the cut-off value of the PSA
density. Spearman's rank correlation and linear regression were
used to determine the relationship between TRUS based PSA density
and MRI based PSA density. All reported P-values were two-sided
with significance considered at P<0.05.
Results
Patient characteristics
The median age of patients was 76 (range, 70–85)
years, median serum PSA level was 7.2 (95% confidence interval
(CI), 4.0–15.5) ng/ml, median MRI ROI size was 10.0 (95% CI,
0.0–24.3) mm, median prostate volume was 35.1 (95% CI, 18.5–80.5)
cc, and PSA density was 0.20 (95% CI, 0.08–0.51) ng/ml/cc (Table I). The correlation between TRUS-PSA
density and MRI-PSA density was very strong (r=0.873) and
significant (P<0.001). There was no inter-observer error in the
measurement of PSA density using TRUS and MRI.
 | Table I.Characteristics of all patients who
underwent MRI before needle biopsy of the prostate. |
Table I.
Characteristics of all patients who
underwent MRI before needle biopsy of the prostate.
| Characteristic | Overall (N=241)
median ± SD (95% CI) |
|---|
| Age, years | 76±4.3 (70–85) |
| PSA, ng/ml | 7.2±3.6
(4.0–15.5) |
| MRI ROI size, mm | 10.0±7.1
(0.0–24.3) |
| Prostate volume,
cc | 35.1±18.3
(18.5–80.5) |
| PSA density,
ng/ml/cc | 0.20±0.14
(0.08–0.51) |
Prostate cancer detection on
mpMRI
In total, 221 patients had suspicious lesions for
cancer in mpMRI (Table II). The
median PSA density of these patients was 0.21 ng/ml/cc. Conversely,
20 patients did not have suspicious lesions for cancer in mpMRI,
and their median PSA density was 0.16 ng/ml/cc, which was
significantly lower (P=0.023).
| Table II.Clinical characteristics and
predictors analysis of patients among MRI lesions suspicious and
not suspicious for prostate cancer. |
Table II.
Clinical characteristics and
predictors analysis of patients among MRI lesions suspicious and
not suspicious for prostate cancer.
|
| Suspicious for
PCa | Not suspicious for
PCa |
|
|---|
|
|
|
|
|
|---|
| Characteristic | N=221 median ± SD
(95% CI) | N=20 median ± SD (95%
CI) | P-value |
|---|
| PSA, ng/ml | 7.4±3.7
(3.9–16.3) | 6.7±2.2
(4.6–12.0) | 0.216 |
| MRI ROI size, mm | 12.0±6.5
(5.0–25.0) | NA | NA |
| Prostate volume,
cc | 34.8±18.7
(17.2–81.8) | 45.8±14.5
(22.0–73.5) | 0.098 |
| PSA density,
ng/ml/cc | 0.21±0.14
(0.08–0.51) | 0.16±0.08
(0.09–0.42) | 0.023 |
Prostate cancer detection on
biopsy
PCa was detected on biopsy in 163 patients (Table III). The median PSA density of
these patients was 0.23 ng/ml/cc. Conversely, 78 patients showed no
evidence of malignancy on biopsy, and their median PSA density was
0.16 ng/ml/cc, which was significantly lower (P<0.001).
| Table III.Patients' pathological
characteristics. |
Table III.
Patients' pathological
characteristics.
|
| PCa negative | PCa positive |
|
|---|
|
|
|
|
|
|---|
| Characteristic | N=78 median ± SD (95%
CI) | N=163 median ± SD
(95% CI) | P-value |
|---|
| PSA, ng/ml | 7.5±3.7
(3.6–15.3) | 7.2±3.6
(4.1–16.4) | 0.858 |
| MRI ROI size, mm | 10.0±5.6
(0.0–20.0) | 10.9±7.5
(0.0–28.0) | 0.057 |
| Prostate volume,
cc | 46.0±19.6
(21.9–83.4) | 32.9±16.0
(15.3–71.9) | <0.001 |
| PSA density,
ng/ml/cc | 0.16±0.11
(0.07–0.43) | 0.23±0.15
(0.10–0.51) | <0.001 |
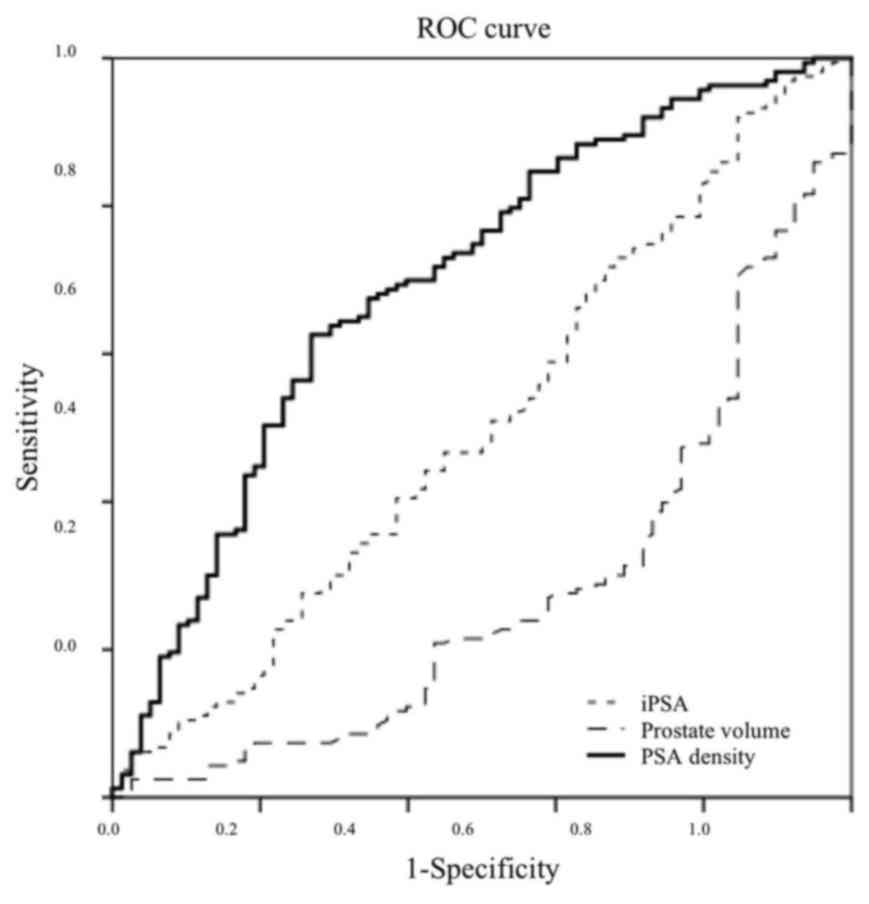
Usefulness of PSA density
The ROC curve analysis for predicting PCa using
mpMRI showed that the maximum AUC values of PSA, prostate volume,
and PSA density were 0.507, 0.280, and 0.698, respectively
(Fig. 2). These results indicated
that PSA density could be a useful parameter to predict PCa. The
PSA density of the maximum AUC value was 0.20 ng/ml/cc. The
sensitivity, specificity, positive predictive value, and negative
predictive value of PSA density threshold of 0.20 ng/ml/cc were 63,
71, 82, and 47%, respectively.
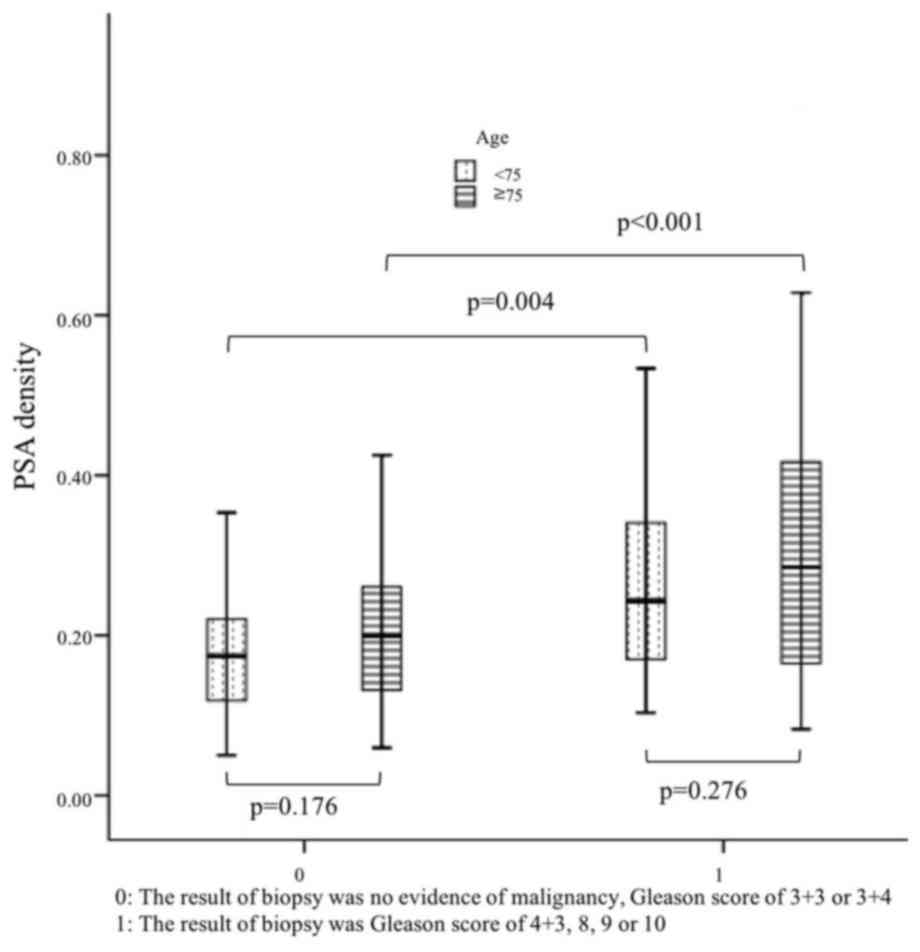
Subgroup analyses
Patients with or without significant PCa did not
differ significantly in their serum PSA level (P=0.089). Prostate
volume of patients with significant PCa was significantly smaller
(P<0.001). Calculated PSA density was significantly higher in
patients with significant PCa with a median of 0.27 ng/ml/cc vs.
0.18 ng/ml/cc (P<0.001). The median PSA density of patients with
and without significant PCa at the age of 70 to 75 years differed
significantly, at 0.24 and 0.17 ng/ml/cc, respectively (P=0.004).
The median PSA density of patients with and without significant PCa
over the age of 75 years also differed significantly, at 0.29 and
0.20 ng/ml/cc (P<0.001, Fig.
3).
Discussion
Although mpMRI is increasingly used for PCa
diagnosis, there is no consensus whether or not older men need a
biopsy and how follow-up should be managed. In the present study,
mpMRI combined with PSA density before biopsy for older men was
useful for the selection of prostate biopsy. Until recently,
previous reports have described the use of MRI before biopsy
combined with PSA density (16,17);
however, no reports have focused on age. Kosaka et al
reported that PSA density was a very effective predictor of
clinically significant PCa in men aged 50 years and younger
(18). Our results indicated that
PSA density could also help predict the presence of PCa and
significant PCa in men aged 70 years and older.
Compared with younger patients, older patients were
more likely to present with advanced diseases and had a greater
risk of death from PCa. However, older men have a shorter life
expectancy and a higher risk of competing causes of mortality
(19). In our study, 20 patients did
not have suspicious lesions for cancer in mpMRI but underwent PBx.
No significant PCa was detected in these 20 patients after PBx. Men
without suspicious lesions for cancer in mpMRI could have avoided a
biopsy. Men with lower PSA density have a lower risk of significant
cancer, and these men could have avoided a biopsy. The cut-off
value of PSA density was previously reported as 0.15 or 0.20
ng/ml/cc (16,20,21),
which was the PSA density of the maximum AUC values in our
study.
Our retrospective study has several limitations.
First, all elderly patients in the present study underwent PBx
after MRI. Patients without lesions suspicious for PCa on mpMRI had
already been excluded. Older men with lesions suspicious for PCa on
mpMRI, who were too sick to undergo PBx, were also excluded.
Second, with marked advances in mpMRI, further prospective studies
considering prognosis could be more precise in defining the role of
mpMRI combined with PSA density.
Despite these limitation, there are advantages in
the present study. First, we focused on older men aged 70 years and
older. Older men have a shorter life expectancy and prognosis can
be evaluated more easily than in younger men. An additional study
considering patient prognosis will be carried out in the future.
There is a possibility that cancer in smaller prostates was more
easily detected, and larger glands could be associated with
difficulty in detecting cancer. Discussion of data on the
correlation between prostate size and pathological features of PCa
will be examined in an upcoming study. Second, it has been
controversial whether to perform MRI before biopsy for men of all
ages because of cost-effectiveness. For older men with a shorter
life expectancy, however, the cost savings from avoiding
unnecessary biopsies will offset the cost of MRI.
In conclusion, PSA density combined with mpMRI
before PBx performed significantly better compared with mpMRI or
PSA density alone. The combination is a helpful method and can be a
decision-making model for the selection of PBx.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The analyzed data sets generated during the study
are available from the corresponding author on reasonable
request.
Authors' contributions
YY and TK collected the data and wrote the
manuscript. KM, RM and SM reviewed the slides and confirmed the
pathological diagnoses. TS and MJ reviewed the images and confirmed
the radiological diagnoses. YY and HH analyzed and interpreted the
patient data regarding the clinical outcomes. AM, EK and MO
provided the study concept and design, and revised the manuscript.
The final version of the manuscript was read and approved by all
authors.
Ethics approval and consent to
participate
The postoperative prognostic and clinicopathological
data were analyzed retrospectively in accordance with a protocol
approved by the Keio University Institutional Review Board.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Daskivich TJ, Fan KH, Koyama T, Albertsen
PC, Goodman M, Hamilton AS, Hoffman RM, Stanford JL, Stroup AM and
Litwin MS: Original research effect of age, tumor risk and
comorbidity on competing risks. Ann Intern Med. 158:709–717. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015. CA Cancer J Clin. 65:5–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Honorable T and Lew JJ: Social security.
Available via DIALOG. https://www.ssa.gov/OACT/population/longevity.htmlMarch
1–2018
|
|
4
|
Smith RA, Manassaram-Baptiste D, Brooks D,
Doroshenk M, Fedewa S, Saslow D, Brawley OW and Wender R: Cancer
screening in the United States, 2015: A review of current American
cancer society guidelines and current issues in cancer screening.
CA Cancer J Clin. 65:30–54. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Heidenreich A, Bastian PJ, Bellmunt J,
Bolla M, Joniau S, van der Kwast T, Mason M, Matveev V, Wiegel T,
Zattoni F, et al: EAU guidelines on prostate cancer. part 1:
Screening, diagnosis, and local treatment with curative
intent-update 2013. Eur Urol. 65:124–137. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lin K, Lipsitz R, Miller T and Janakiraman
S; U.S. Preventive Services Task Force, : Benefits and harms of
prostate-specific antigen screening for prostate cancer: An
evidence update for the U.S. Preventive Services Task Force. Ann
Intern Med. 149:192–199. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Carter HB, Albertsen PC, Barry MJ, Etzioni
R, Freedland SJ, Greene KL, Holmberg L, Kantoff P, Konety BR, Murad
MH, et al: Early detection of prostate cancer: AUA guideline. J
Urol. 190:419–426. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Williamson DA, Barrett LK, Rogers BA,
Freeman JT, Hadway P and Paterson DL: Infectious complications
following transrectal ultrasound-guided prostate biopsy: New
challenges in the era of multidrug-resistant Escherichia coli. Clin
Infect Dis. 57:267–274. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Schröder F and Kattan MW: The
comparability of models for predicting the risk of a positive
prostate biopsy with prostate-specific antigen alone: A systematic
review. Eur Urol. 54:274–290. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sonn GA, Chang E, Natarajan S, Margolis
DJ, Macairan M, Lieu P, Huang J, Dorey FJ, Reiter RE and Marks LS:
Value of targeted prostate biopsy using magnetic
resonance-ultrasound fusion in men with prior negative biopsy and
elevated prostate-specific antigen. Eur Urol. 65:809–815. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pokorny MR, de Rooij M, Duncan E, Schröder
FH, Parkinson R, Barentsz JO and Thompson LC: Prospective study of
diagnostic accuracy comparing prostate cancer detection by
transrectal ultrasound-guided biopsy versus magnetic resonance (MR)
imaging with subsequent MR-guided biopsy in men without previous
prostate biopsies. Eur Urol. 66:22–29. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hoeks CM, Schouten MG, Bomers JG,
Hoogendoorn SP, Hulsbergen-van de Kaa CA, Hambrock T, Vergunst H,
Sedelaar JP, Fütterer JJ and Barentsz JO: Three-Tesla magnetic
resonance-guided prostate biopsy in men with increased
prostate-specific antigen and repeated, negative, random,
systematic, transrectal ultrasound biopsies: Detection of
clinically significant prostate cancers. Eur Urol. 62:902–909.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hattori S, Kosaka T, Mizuno R, Kanao K,
Miyajima A, Yasumizu Y, Yazawa S, Nagata H, Kikuchi E, Mikami S, et
al: Prognostic value of preoperative multiparametric magnetic
resonance imaging (MRI) for predicting biochemical recurrence after
radical prostatectomy. BJU Int. 113:741–747. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Barentsz JO, Richenberg J, Clements R,
Choyke P, Verma S, Villeirs G, Rouviere O, Logager V and Fütterer
JJ; European Society of Urogenital Radiology, : ESUR prostate MR
guidelines 2012. Eur Radiol. 22:746–757. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kikuchi E, Nakashima J, Ishibashi M,
Ohigashi T, Asakura H, Tachibana M and Murai M: Prostate specific
antigen adjusted for transition zone volume: The most powerful
method for detecting prostate carcinoma. Cancer. 89:842–849. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Distler FA, Radtke JP, Bonekamp D, Kesch
C, Schlemmer HP, Wieczorek K, Kirchner M, Pahernik S, Hohenfellner
M and Hadaschik BA: The value of PSA density in combination with
PI-RADSTM for the accuracy of prostate cancer
prediction. J Urol. 198:575–582. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kubota Y, Kamei S, Nakano M, Ehara H,
Deguchi T and Tanaka O: The potential role of prebiopsy magnetic
resonance imaging combined with prostate-specific antigen density
in the detection of prostate cancer. Int J Urol. 15:322–327. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kosaka T, Mizuno R, Shinojima T, Miyajima
A, Kikuchi E, Tanaka N, Shinoda K, Morita S, Mikami S and Oya M:
The implications of prostate-specific antigen density to predict
clinically significant prostate cancer in men ≤50 years. Am J Clin
Exp Urol. 2:332–336. 2014.PubMed/NCBI
|
|
19
|
Daskivich TJ, Fan KH, Koyama T, Albertsen
PC, Goodman M, Hamilton AS, Hoffman RM, Stanford JL, Stroup AM,
Litwin MS and Penson DF: Effect of age, tumor risk, and comorbidity
on competing risks for survival in a U.S. population-based cohort
of men with prostate cancer. Ann Intern Med. 158:709–717. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
van den Bergh RC, Roemeling S, Roobol MJ,
Aus G, Hugosson J, Rannikko AS, Tammela TL, Bangma CH and Schröder
FH: Outcomes of men with screen-detected prostate cancer eligible
for active surveillance who were managed expectantly. Eur Urol.
55:1–8. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tosoian JJ, Trock BJ, Landis P, Feng Z,
Epstein JI, Partin AW, Walsh PC and Carter HB: Active surveillance
program for prostate cancer: An update of the Johns Hopkins
experience. J Clin Oncol. 29:2185–2190. 2011. View Article : Google Scholar : PubMed/NCBI
|