Introduction
Oral mucositis (OM) is a common and potentially
dangerous complication of anticancer treatment. Inflammation and
ulcerations of the oral mucosa make swallowing and, thereby, eating
and drinking, difficult or even impossible, leading to anorexia and
weight loss (1). There is a serious
risk of infections and even sepsis, particularly in
immunocompromised patients (2,3). OM is
associated with severe pain, affects the quality of life, and often
requires reduction or suspension of chemotherapy and/or
radiotherapy, thereby decreasing the relative dose intensity, which
may worsen prognosis (2,3).
The risk and severity of mucositis depend on the
type of therapy. It is diagnosed in 60–100% of patients receiving
myeloablative therapy and in almost all patients on combined
chemotherapy and radiotherapy (1,4). OM
initially manifests with erythematous spots on the oral mucosa or
tongue, which subsequently develop into painful ulcers (1,2).
Xerostomia is common and represents one of the most troublesome
symptoms of OM (1,2). Ulcers, xerostomia and restricted diet
lead to microbiome disruption and colonization by opportunistic or
pathogenic microorganisms (2).
Dental caries, periodontal disease, ill-fitting dentures and other
such problems must be resolved prior to the initiation of
anticancer therapy and further treatment as needed (1). Poor oral hygiene, smoking and alcohol
use exacerbate OM symptoms and trigger oral infections (2). Approximately 1 in 10 patients on
radiotherapy or chemoradiotherapy will develop severe OM and may
require hospitalization and treatment rescheduling (2).
The first clinical signs of OM usually appear 4–5
days after initiation of chemotherapy, with development of
ulcerations after 7–10 days; the ulcers tend to grow in number and
size and merge to form large ulcerated areas (2,3). These
ulcers are very painful, cause difficulty in swallowing and may
necessitate the administration of opioid analgesics. They require
~2 weeks to heal once chemotherapy has been suspended (2,3).
Since there are currently few therapeutic options
for OM, there is a need to identify novel approaches to its
management and prevention. Oncoxin (ONCX), a nutritional supplement
enriched with amino acids, vitamins, minerals and naturally
occurring antioxidants, has been previously demonstrated to improve
appetite, quality of life and overall survival in patients with
end-stage hepatocellular carcinoma (5). The aim of the present study was to
evaluate the efficacy of ONCX in cancer patients with OM who
receive chemotherapy, radiotherapy or a combination of the two.
Materials and methods
Study population
The eligibility criteria for inclusion in the study
were as follows: Male and female patients who had signed an
informed consent, aged 45–75 years, with malignant neoplasms and
who had been prescribed radiotherapy, chemotherapy or a combination
of the two, with an Eastern Cooperative Oncology Group performance
status score of ≤3, with grade 2–3 OM according to the World Health
Organization (WHO) Oral Toxicity Scale. The exclusion criteria were
as follows: Severe concomitant diseases or conditions that may
complicate or make impossible the patient's participation in the
study, or make it difficult to interpret the clinical data
(including mental disorders, severe infectious and parasitic
diseases and intolerability to any of the ONCX components), the
patient's family or official relations with a member of staff of
the study center, the patient's failure to assess his/her physical
and/or emotional condition, the patient's failure to comply with
the study requirements, the patient's refusal to participate in the
study and pregnancy or lactation.
The present study was approved by the Ethics
Committee of The Loginov Moscow Clinical Scientific Centre,
protocol 3/2017 4.17.17. The inclusion period was between November
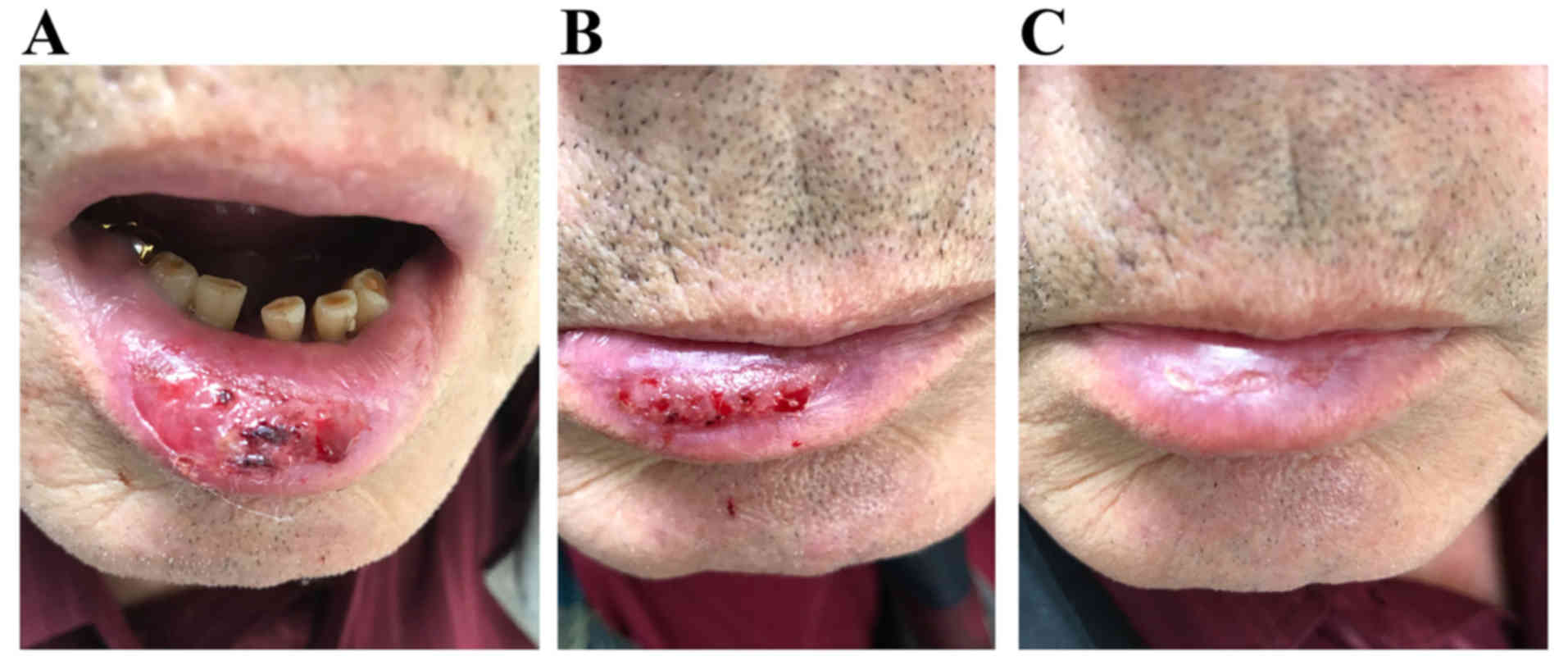
2017 and March 2018. In accordance with the Declaration of
Helsinki, all patients provided written informed consent to
participate in the study and to publish the results and anonymized
photos. The study was retrospectively registered under the study
registration number NCT03577535.
Study design and treatment
The present study was a pilot study conducted to
verify the hypothesis that ONCX can improve the symptoms of OM. The
primary objective of the study was to evaluate the efficacy of ONCX
in patients with grade 2–3 OM based on the WHO Oral Toxicity Scale.
The following outcome measures were used: Mean WHO Oral Toxicity
Scale grade (primary endpoint), body mass, days with regular food
intake, days with normal appetite, adverse events and the Common
Toxicity Criteria (ver. 2) of the National Cancer Institute
(https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcv20_4-30-992.pdf)
using the blood, hepatic and infection scales. The study regimen is
shown in Fig. 1. This study was a
single-center, open-label, randomized trial in two parallel groups
with a 20-day treatment period. No follow-up period was intended.
The study was conducted at a stomatological clinic (Medical
Scientific Centre of Professor Shumsky, Samara, Russian
Federation). Patients were randomly allocated in 2:1 comparison
groups for the ONCX and control groups, respectively. A total of 15
patients were enrolled in the study; 10 in the ONCX group and 5 as
controls. Sequentially numbered opaque sealed envelopes were used
as the method for randomization. The study center was provided with
excess amount of ONCX and excess number of envelopes.
Treatment
Patients from both groups were allowed to use any
anticancer treatment and any OM care prior to the present study. In
addition to their current treatment, patients in the ONCX group
used 25 ml of the ONCX nutritional supplement twice daily for 20
days. ONCX contains microelements, vitamins, amino acids and
certain naturally occurring, biologically active substances; the
composition of ONCX is presented in Table I. The next course of chemotherapy or
chemoradiotherapy was withheld until the full resolution of OM
symptoms. Oral cavity and dental treatment were provided to all
patients as the standard procedure before the start of
chemotherapy. Caries and dental deposits were treated if necessary
during the study. As a part of oral care, patients used oral washes
containing antiseptics including octenidine dihydrochloride and
phenoxyethanol or myramistin. To accelerate the regeneration
process, Solcoseryl dental adhesive paste and Actovegin tablets
were used. Patients were advised to use soft or very soft
toothbrushes and non-abrasive toothpaste with a foaming effect. In
case of moderate or severe pain, patients were advised to use
nimesulide tablets and local application of lidocaine gel.
 | Table I.Composition of Oncoxin per 100 ml. |
Table I.
Composition of Oncoxin per 100 ml.
| Components | Quantity |
|---|
| Glycine | 2,000 mg |
| Glucosamine | 2,000 mg |
| Malic acid | 1,200 mg |
| Arginine | 640 mg |
| Cysteine | 204 mg |
| Mono-ammonium
glycyrrhizinate | 200 mg |
| Ascorbic acid | 200 mg |
| Sodium
methylparaben | 120 mg |
| Zinc sulfate | 100 mg |
| Green tea
extract | 80 mg |
| Calcium
pantothenate | 25 mg |
| Pyridoxine | 12 mg |
| Manganese
sulfate | 4 mg |
| Cinnamon extract | 3 mg |
| Folic acid | 400 µg |
| Cyanocobalamin | 2 µg |
Statistical analysis
Statistical analysis was performed using StatSoft
Statistica 10.0 software (http://statsoft.ru/). Baseline characteristics are
presented as mean ± standard deviation; when comparisons between
groups or within a group were made, the data were presented as mean
(95% confidence interval). The differences between the ONCX and
control groups were compared using Mann-Whitney U test and the
differences within each group were compared using sign test;
P<0.05 was considered to indicate a statistically significant
difference.
Results
Patient characteristics
The baseline characteristic of the patients are
presented in Table II. There were
no statistically significant differences between the groups at the
baseline. It should be noted that no underweight patients were
included in the present study. No patients required administration
of opioid analgesics throughout the study.
| Table II.Patient baseline characteristics
according to group allocation. |
Table II.
Patient baseline characteristics
according to group allocation.
|
| Groups (mean ±
standard deviation) |
|
|---|
|
|
|
|
|---|
| Characteristics | Oncoxin (n=10) | Control (n=5) |
|---|
| Age, years | 62.0±7.9 | 64.0±10.3 |
| Height, cm | 170.7±6.7 | 170.8±5.6 |
| Body mass, kg | 68.0±8.2 | 73.6±6.5 |
| Mean WHO Oral
Toxicity | 2.6±0.52 | 3.0±0.0 |
| Scale grade |
| Chemotherapy, n | 4 | 1 |
| Chemoradiotherapy,
n | 6 | 4 |
Efficacy
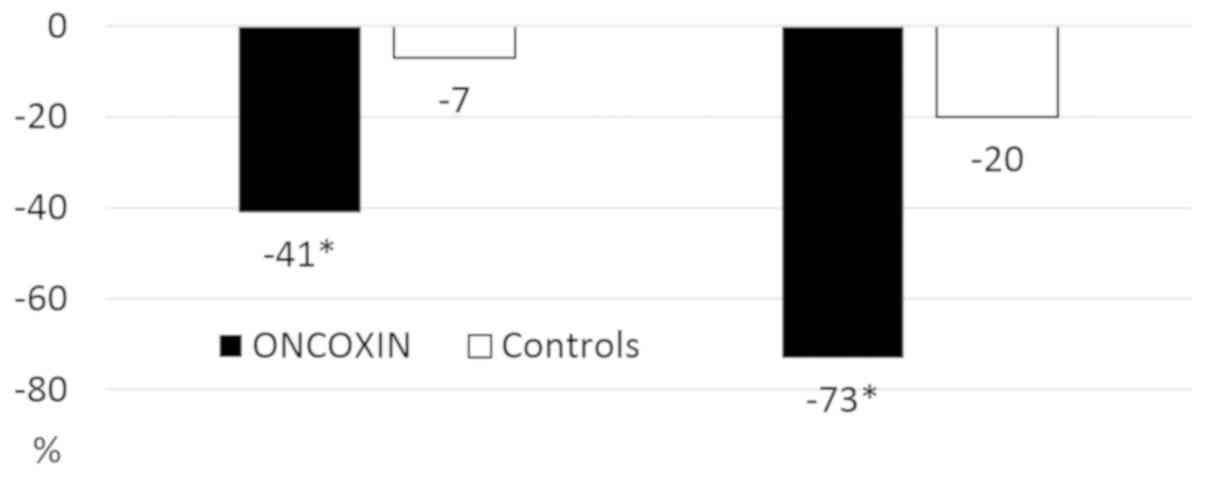
The changes in efficacy outcomes during the study
are listed in Table III. The WHO
Oral Toxicity Scale grade had decreased by 41% in the ONCX group at
~7 days from the start of the study (Visit 2) compared with a
minimal change in the control group. At the end of the study, the
difference was even more prominent, with a 73 and 20% decrease from
the baseline in the ONCX and control groups, respectively (Figs. 2 and 3).
| Table III.Efficacy outcome changes during the
study. |
Table III.
Efficacy outcome changes during the
study.
|
| Groups [mean (95%
confidence interval)] |
|
|---|
|
|
|
|
|---|
| Efficacy
outcomes | Oncoxin (n=10) | Controls (n=5) | P-value |
|---|
| Mean WHO Oral
Toxicity Scale grade |
|
Baseline | 2.60 (2.23–2.97) | 3.0 | 0.25 |
| Visit
2 | 1.56
(0.88–2.23) | 2.80
(2.24–3.36) | 0.02 |
| Visit
3 | 0.70
(0.35–1.05) | 2.40
(1.72–3.08) | <0.001 |
| Body mass |
|
Baseline | 68.0 (62.2–73.8) | 73.6 (65.5–81.7) | 0.31 |
| Visit
2 | 68.1 (62.7–73.5) | 72.2 (63.7–80.7) | 0.51 |
| Visit
3 | 69.6 (63.6–75.6) | 71.6 (63.1–80.0) | 0.86 |
| Days with intake of
regular food |
| Visit
1-Visit 2 | 3.90
(3.19–4.61) | 1.6
(−0.66–3.86) | 0.03 |
| Visit
2-Visit 3 | 9.70
(5.78–13.62) | 4.4
(−1.26–10.06) | 0.09 |
| Visit
1-Visit 3 | 13.6
(9.43–17.76) | 6.00
(−1.90–13.90) | 0.04 |
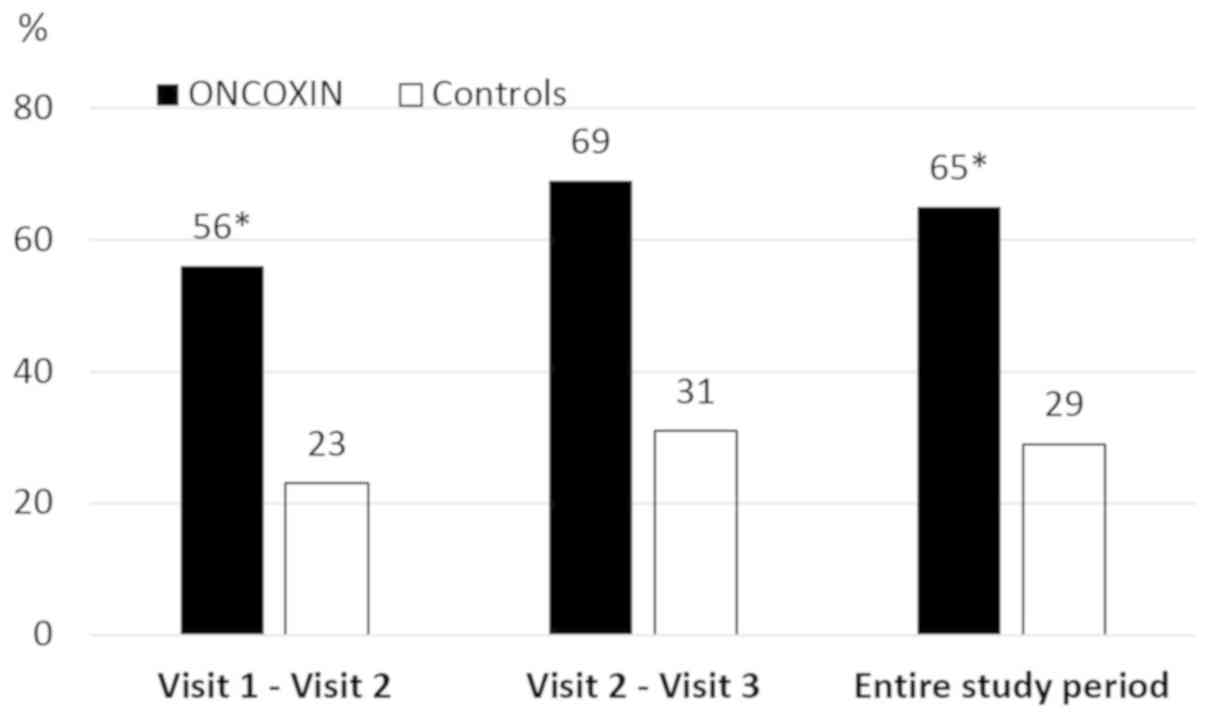
A significant difference in number of days with
regular food intake was observed. Over the entire testing period,
patients in the ONCX group were able to eat normally during 65% of
the days, in contrast to only 29% of the days in the control group
(Fig. 4).
There were no statistically significant changes in
absolute body mass between groups or even within each group,
although there were clear positive and negative tendencies in the
ONCX and control groups, respectively. Thus, mean change from the
body mass baseline was calculated and it was found that ONCX caused
a weight gain of 2.5 kg (−1.86 to 6.86) over 20 days, whereas the
control group exhibited loss of 2.8 kg (−4.96 to −0.55) (P=0.03).
No statistically relevant differences in the number of days with
normal appetite were observed. In the control group there were no
days with normal appetite throughout the whole study, while in the
ONCX group there were 4.80 (0.59–9.01) days with normal appetite
between Visits 2 and 3 (P=0.13 vs. controls).
Toxicity
In addition to efficacy outcomes, some differences
in treatment toxicity were also observed (Table IV). The decrease of liver toxicity
is of a special interest. The alanine aminotransferase and
aspartate aminotransferase levels had decreased 4- to 7-fold at the
end of the treatment in the ONCX group, whereas no changes were
observed in the control group. The leukocyte count and incidence of
infections were also in favour of the ONCX group. Therefore, ONCX
was found to be well-tolerated, without associated adverse
events.
| Table IV.Individual toxicity grades according
to grading criteria of the National Cancer Institute Common
Toxicity Criteria (ver. 2). |
Table IV.
Individual toxicity grades according
to grading criteria of the National Cancer Institute Common
Toxicity Criteria (ver. 2).
|
| Groups [mean (95%
confidence interval)] |
|
|---|
|
|
|
|
|---|
| Efficacy
outcomes | Oncoxin (n=10) | Controls (n=5) | P-value |
|---|
| Leukocytes |
|
Baseline | 1.30 (0.95–1.65) | 1.00 | 0.37 |
| Visit
2 | 0.60 (0.23–0.97) | 1.00 | 0.25 |
| Visit
3 | 0.11
(−0.15–0.37) | 0.80
(0.24–1.36) | 0.04 |
| Infections |
|
Baseline | 1.70 (1.35–2.05) | 1.80 (1.24–2.36) | 0.77 |
| Visit
2 | 1.00
(0.66–1.34) | 1.40
(0.29–2.51) | 0.31 |
|
Visit 3 | 0.11
(−0.15–0.37) | 1.20
(0.64–1.76) |
<0.005 |
| Alanine
aminotransferase |
|
Baseline | 1.50
(0.99–2.01) | 1.00 | 0.13 |
| Visit
2 | 0.70
(0.22–1.18) | 1.00 | 0.37 |
|
Visit 3 | 0.33
(−0.05–0.72) | 1.00 | 0.04 |
| Aspartate
aminotransferase |
|
Baseline | 1.50
(0.99–2.01) | 1.00 | 0.13 |
| Visit
2 | 0.40
(0.03–0.77) | 1.00 | 0.08 |
|
Visit 3 | 0.22
(−0.12–0.56) | 1.00 | 0.012 |
Discussion
Different treatment options and drugs have been
tested in OM, only some of which exhibited clinical relevance such
as oral cryotherapy, keratinocyte growth factor and amino acids
enriched diets. Therefore, there is a clear requirement for new
approaches to the prevention and effective treatment of OM. ONCX is
a multicomponent nutritional supplement that contains vitamins,
amino acids, microelements and macromolecular biologically active
substances. These substances have broad-spectrum antioxidant,
anti-inflammatory and antimicrobial activities (6).
Glycine, cysteine, zinc, vitamin C and
epigallocatechin gallate (EGCG) are potent antioxidants (6). EGCG is a naturally occurring polyphenol
and the main component of green tea extract. A high effectiveness
of EGCG in acute esophagitis induced by radiotherapy or
chemoradiotherapy was reported in clinical trials (7,8).
Another component of ONCX is glucosamine. As shown
in clinical studies, glucosamine decreases the systemic levels of
C-reactive protein and prostaglandin E2 (9), whereas in murine models of colitis,
glucosamine intake led to decreased expression of tumor necrosis
factor (TNF)-α and interleukin-1 in the colonic mucosa, effects
which were mediated by downregulation of nuclear factor (NF)-κB
(10). Dietary zinc also suppresses
systemic inflammation, as shown by the substantial decrease in
TNF-α production in elderly patients (11). Glycyrrhizinic acid (GA) is a
well-known substance with hepatoprotective activity and
broad-spectrum anti-inflammatory properties, mediated via NF-κB and
cyclooxygenase-2 (6). GA can
markedly decrease liver damage in patients who receive the MMF
chemotherapeutic regimen for breast cancer, or FOLFOX/XELOX for
gastrointestinal tumors (12,13). It
is hypothesized that these effects of GA are due to its antioxidant
and anti-inflammatory properties.
The antimicrobial properties of ONCX are also
notable. Infectious complications of OM are common, and markedly
contribute to clinical deterioration. Additional zinc intake is
accompanied by decreased frequency of infections in elderly
patients, as well as in children and adolescents with acute
leukemia (11,14).
Vitamins that regulate one-carbon metabolism pathway
(pyridoxine, folate and cobalamin) play a crucial role in DNA
structure stabilization and repair. Their deficiency is associated
with single- and double-strand DNA breaks, which are similar to the
effects of ionizing radiation (15).
Taken together, these properties may be responsible
for the efficacy of ONCX in decreasing OM symptoms, and in
improving the ability to ingest solid foods and maintain body
weight. In addition, ONCX components help control infectious
complications and decrease the toxicity of therapy with regards to
leukocyte count and liver damage. The trend of improvement in body
mass and appetite and the lack of statistically meaningful
differences are hypothesized to be due to the insufficient number
of patients included in the present study. Another possible reason
is that the baseline body mass index of all included patients was
>19, and there were no underweight patients, whereas some were
overweight.
In conclusion, this was a pilot study conducted to
demonstrate the benefits of ONCX nutritional supplement in OM. It
was observed that ONCX rapidly improved the symptoms of OM,
maintained body mass and decreased the toxicity of anticancer
therapy. Although the number of participants was small, the results
appear to be promising. However, further large-scale studies are
required to confirm the value of ONCX in the management of OM.
Acknowledgements
Not applicable.
Funding
Catalysis S.L. provided Oncoxin nutritional
supplement for the purposes of this study. No other funding was
received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
AS was responsible for patient selection, treatment
and interpretation of final results. EB was involved in study
design, protocol and procedure development and interpretation of
final results. ES was involved in study design, protocol and
procedures development and manuscript preparation. FP performed
statistical analysis and was a major contributor in writing the
manuscript. All authors have read and approved the final version of
this manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
The Loginov Moscow Clinical Scientific Center, protocol 3/2017
4.17.17. The inclusion period was between November 2017 and March
2018.
Patient consent for publication
In accordance with the Declaration of Helsinki, all
patients provided written informed consent to participate in the
study and to publish its results and anonymized photos.
Competing interests
Dr Eduardo Sanz is a Scientific Department Managing
Director of Catalysis S.L., the manufacturer and provider of
Oncoxin for the purposes of the study. All other authors declare
that they have no competing interests to disclose.
Glossary
Abbreviations
Abbreviations:
|
OM
|
oral mucositis
|
|
ONCX
|
Oncoxin
|
References
|
1
|
Shumsky AV: Pathology of oral cavity
induced by chemotherapy and radiotherapy in oncology patients.
Oncology for Dentists. Stomatology for Oncologists. Vse pravilno:
Moscow: pp. 234–246. 2016
|
|
2
|
Lalla RV, Sonis ST and Peterson DE:
Management of oral mucositis in patients who have cancer. Dent Clin
North Am. 5261–77. (viii)2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Campos MI, Campos CN, Aarestrup FM and
Aarestrup BJ: Oral mucositis in cancer treatment: Natural history,
prevention and treatment. Mol Clin Oncol. 2:337–340. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wardley AM, Jayson GC, Swindell R,
Morgenstern GR, Chang J, Bloor R, Fraser CJ and Scarffe JH:
Prospective evaluation of oral mucositis in patients receiving
myeloablative conditioning regimens and haemopoietic progenitor
rescue. Br J Haematol. 110:292–299. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Al-Mahtab M, Akbar SM, Khan MS and Rahman
S: Increased survival of patients with end-stage hepatocellular
carcinoma due to intake of ONCOXIN®, a dietary
supplement. Indian J Cancer. 52:443–446. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dzhugashvili M, Pokrovsky VS and Snegovoy
AV: Novel approaches for the correction of micronutrient deficiency
in patients with malignant tumors. Malignant Tumours. 2:55–65.
2016.
|
|
7
|
Zhao H, Zhu W, Xie P, Li H, Zhang X, Sun
X, Yu J and Xing L: A phase I study of concurrent chemotherapy and
thoracic radiotherapy with oral epigallocatechin-3-gallate
protection in patients with locally advanced stage III
non-small-cell lung cancer. Radiother Oncol. 110:132–136. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhao H, Xie P, Li X, Zhu W, Sun X, Sun X,
Chen X, Xing L and Yu J: A prospective phase II trial of EGCG in
treatment of acute radiation-induced esophagitis for stage III lung
cancer. Radiother Oncol. 114:351–356. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kantor ED, Lampe JW, Navarro SL, Song X,
Milne GL and White E: Associations between glucosamine and
chondroitin supplement use and biomarkers of systemic inflammation.
J Altern Complement Med. 20:479–485. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bak YK, Lampe JW and Sung MK: Effects of
dietary supplementation of glucosamine sulfate on intestinal
inflammation in a mouse model of experimental colitis. J
Gastroenterol Hepatol. 29:957–963. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Prasad AS, Beck FWJ, Bao B, Fitzgerald JT,
Snell DC, Steinberg JD and Cardozo LJ: Zinc supplementation
decreases incidence of infections in the elderly: Effect of zinc on
generation of cytokines and oxidative stress. Am J Clin Nutr.
85:837–844. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Akimoto M, Kimura M, Sawano A, Iwasaki H,
Nakajima Y, Matano S and Kasai M: Prevention of cancer
chemotherapeutic agent-induced toxicity in postoperative breast
cancer patients with glycyrrhizin (SNMC). Gan No Rinsho.
32:869–872. 1986.(In Japanese). PubMed/NCBI
|
|
13
|
Yan Y, Mo Y and Zhang D: Magnesium
isoglycyrrhizinate prevention of chemotherapy-induced liver damage
during initial treatment of patients with gastrointestinal tumors.
Zhonghua Gan Zang Bing Za Zhi. 23:204–208. 2015.(In Chinese).
PubMed/NCBI
|
|
14
|
Consolo LZ, Melnikov P, Cônsolo FZ,
Nascimento VA and Pontes JC: Zinc supplementation in children and
adolescents with acute leukemia. Eur J Clin Nutr. 67:1056–1059.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ames BN: DNA damage from micronutrient
deficiencies is likely to be a major cause of cancer. Mutat Res.
475:7–20. 2001. View Article : Google Scholar : PubMed/NCBI
|