Introduction
Pancreatic cancer is a highly lethal malignancy with
short-term survival rates (1) and is
associated with a high mortality rate that closely parallels its
incidence (2). It is generally
considered as a ‘silent disease’ (3)
as there are no signs and symptoms in its early stages, and is
generally diagnosed at an advanced stage (2,3). The
number of new cases of pancreatic cancer were 12.6 per 100,000 men
and women per year according to the National Cancer Institute
Surveillance, Epidemiology, and End Results Program (NCI SEER) data
from 2011–2015 (4). In India, the
incidence of pancreatic cancer is comparatively low at 0.5–2.4 per
100,000 men and 0.2–1.8 per 100,000 women (5). Squamous cell carcinoma (SCC) of
pancreas is a subtype of ductal carcinoma, a non-endocrine part
(6). Primary pancreatic SCC is a
rare malignancy, accounting for 0.5–2% of all malignant pancreatic
tumors (7) and is considered as an
aggressive subtype with a poor prognosis (8). The diagnosis and optimal management of
SCC of pancreas remains poorly defined (9). Furthermore, there is no standard
treatment or guidelines available for the management of SCC of
pancreas owing to the rarity of this malignancy (10,11).
We report here, a case of locally advanced SCC of
the pancreatic tail. The patient was treated with neoadjuvant
nanosomal paclitaxel lipid suspension (NPLS) and gemcitabine
chemotherapy followed by surgery.
Case report
A 60-year-old man, a known case of diabetes,
presented at the Department of Oncology, All India Institute of
Medical Sciences (AIIMS), Bhubaneswar, Odisha, India, in February
2017, with complaints of abdominal pain (epigastric pain radiating
to back), vomiting, weight loss (10 kg over the last 6 months) and
weakness. He was a non-smoker and non-alcoholic. Investigations
revealed that his baseline serum amylase (17.49 IU/l), lipase
(16.76 U/l) and CA 19-9 (29.9 U/ml) levels were within normal
limits. An upper gastrointestinal endoscopy (UGIE) showed a
submucosal swelling which measured 10×10 cm. A computed tomography
(CT) scan of the abdomen revealed a heterogeneously enhancing
cystic and necrotic mass lesion, measuring 8.1×6.8×6.4 cm in the
pancreatic tail, with chronic calcific pancreatitis, diffuse
parenchymal calcification and multiple studded intraductal calculi;
the pancreatic tail region was lobulated near the hilum with
splenic vessel encasement, and a secondary splenic parenchymal
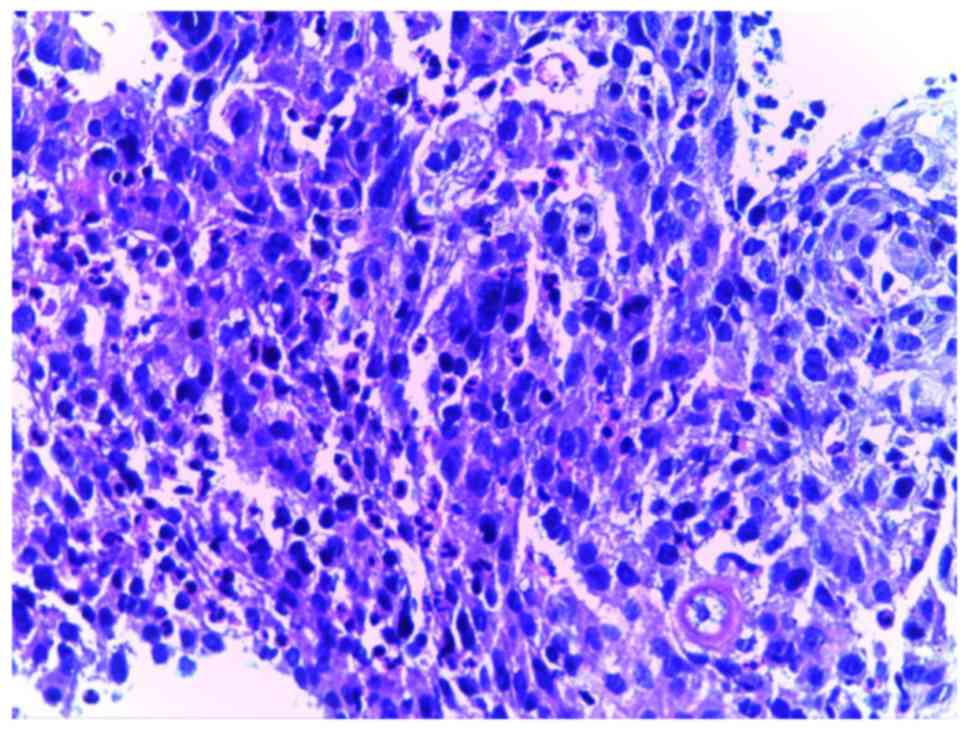
infarct (images not available). A CT guided core needle biopsy of
the pancreatic mass was performed, and histologic examination
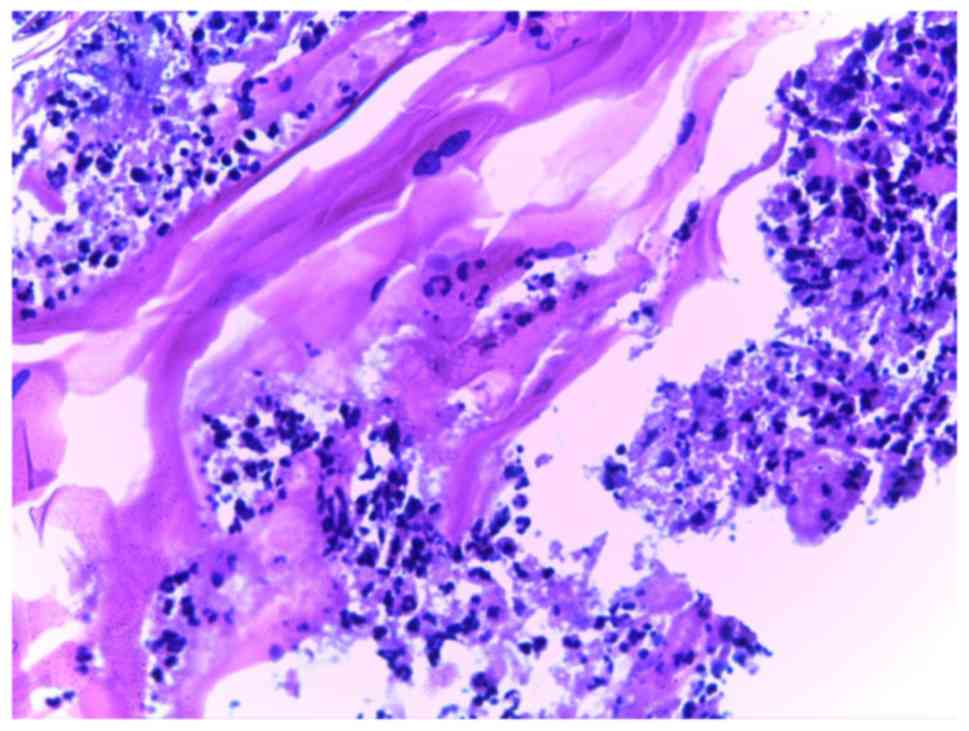
revealed markedly pleomorphic tumor cells in diffuse sheets
(Fig. 1) and large areas of
keratinization and necrosis (Fig.
2). The patient was diagnosed as a case of primary SCC of
pancreas, a rare entity, which arises from the pancreatic duct in
the background of chronic calcific pancreatitis or a pre-existing
pancreatic stone. The staging was confirmed as Stage III (T4N1M0).
Extensive workup performed to evaluate other primary sources and
metastatic disease did not reveal any head and neck malignancy. The
final diagnosis was confirmed as primary SCC of pancreatic
tail.
The Eastern Cooperative Oncology Group (ECOG)
performance status was 1, and neoadjuvant chemotherapy with a
combination of NPLS 120 mg (70 mg/m2) and gemcitabine
1400 mg (800 mg/m2) intravenously (IV) was initiated on
days 1, 8 and 15 every 4 weeks. Premedication with IV ranitidine
(50 mg), dexamethasone (8 mg), chlorpheniramine maleate (10 mg),
and ondansetron (8 mg) was given. On day 1 of the 1st cycle, NPLS
120 mg was reconstituted in 250 ml of 5% dextrose solution and was
administered over 1.5 h; gemcitabine 1.4 was reconstituted in 250
ml normal saline and was administered over 45 min. The patient
complained of nausea and was administered ranitidine 50 mg IV and
ondansetron 8 mg IV. The patient received the same premedications
and chemotherapy on days 8 and 15 of Cycle 1. The patient tolerated
the treatment well; vital signs, liver and renal functions were
normal, and the patient was hemodynamically stable. Similarly, the
second cycle of NPLS-gemcitabine chemotherapy was administered on
days 1, 8 and 15. On day 1 of the second cycle, the patient's
random blood sugar (RBS) level was found to be high (517 mg/dl),
which was managed with insulin. On day 15 of the second cycle, the
patient's hemoglobin (Hb) levels became low (8.6 gm%) and he was
administered 1 unit of packed red blood cells.
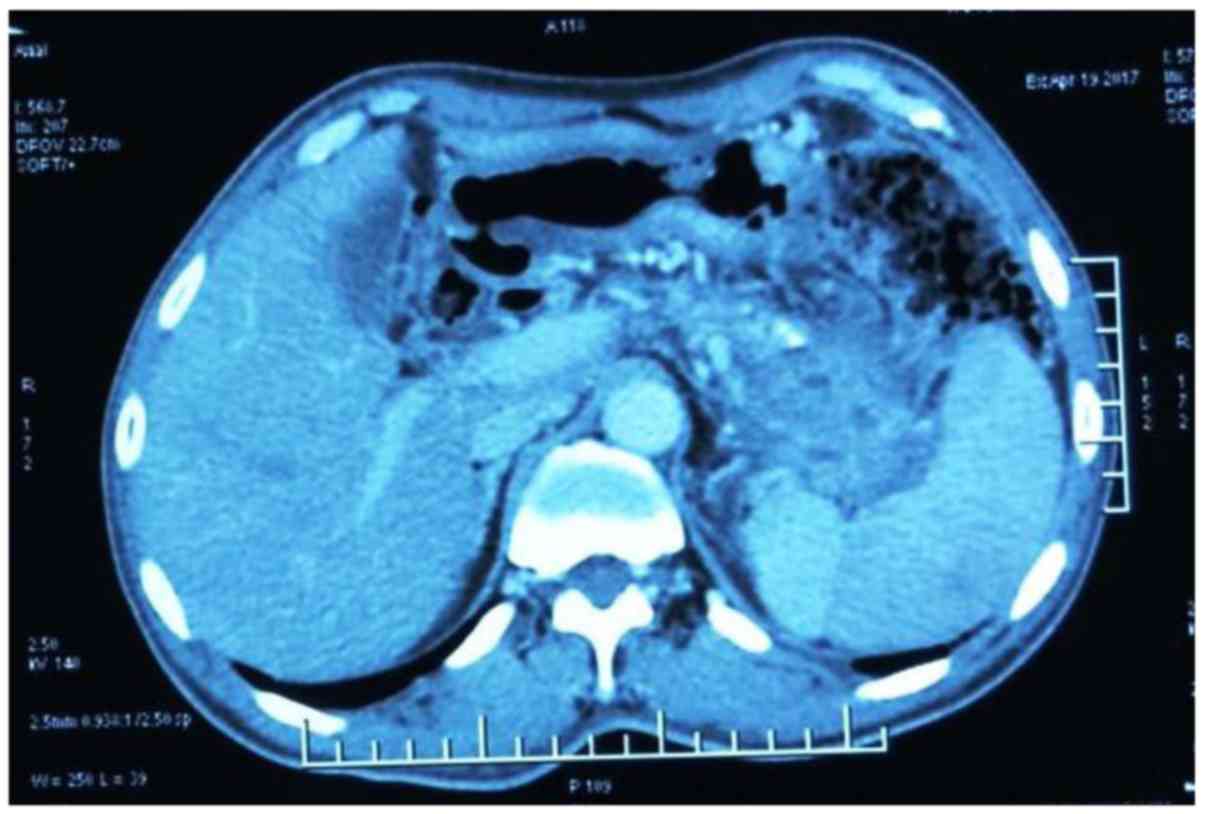
Post completion of 2 cycles of chemotherapy, a
positron emission tomography-CT (PET CT) performed in April 2017
showed hypodense areas in the region of the splenic hilum and
pancreatic tail, along with diffuse peritoneal stranding
(2.3×1.5×2.1 cm), and with standardized uptake values (SUV) of 4.2,
suggestive of a good tumoral response with the regression of tumor
mass (Fig. 3). There was no
hypermetabolic abdominal or retroperitoneal lymphadenopathy, and no
definite abnormal hypermetabolic distant metastases were observed.
The treatment was well-tolerated, and the patient received a third
cycle of NPLS-gemcitabine combination therapy in May 2017 without
any new complaints.
Post 3 cycles of chemotherapy, the patient was
asymptomatic and tolerated the treatment with NPLS and gemcitabine
well with normal complete blood counts (CBC), liver and renal
function tests. Peripheral neuropathy (grade II) and anemia (grade
III) were the adverse events reported in this patient.
Based on the tumoral response on the PET-CT, the
patient was offered surgical exploration. He underwent distal
pancreatico-splenectomy with enblock resection of the involved
stomach and colon in June 2017 and R0 resection was achieved.
Biopsy specimens from the pancreatic margin, celiac lymph node and
right common hepatic lymph node confirmed a well-differentiated SCC
of the tail of pancreas infiltrating into the wall of stomach and
colon. The staging was confirmed as Stage IIA (pT3N0Mx) within the
limitations of metastatic work-up, and the patient was discharged
in stable condition.
Post-surgery, the patient received 2 cycles of
gemcitabine 1 gm IV (day 1, 8 and 15 of each cycle) in combination
with capecitabine 1,000 mg orally (day 1 to 21) as adjuvant
therapy. The patient became asymptomatic and tolerated the
treatment well.
Outcome and follow-up. Seven months post completion
of NPLS and gemcitabine therapy, an ultrasound (USG) performed in
December 2017 revealed multiple metastatic lesions in the liver, a
segment 5 lesion causing infiltration of the common bile duct and
resultant bilobar intrahepatic biliary radical dilatation (IHBRD)
and minimal ascites. The patient underwent percutaneous
transhepatic biliary drainage (PTBD) with stenting, but succumbed
after 2 months, leading to an overall survival (OS) of
approximately 1 year after having started NPLS treatment.
Discussion
Pancreatic cancer is one of the deadliest
malignancies, and is associated with a poor prognosis (12). The symptoms can vary depending upon
the anatomic location of the tumor. The head of the pancreas (78%)
is most commonly affected, followed by the body (11%) and tail
(11%) (3). Cancers of the pancreatic
head are located near the common bile duct, may cause jaundice even
if they are small, and can be diagnosed at an early stage. However,
cancers of the pancreatic body or tail don't impinge on the duct
until they have spread through the pancreas and are at an advanced
stage (13). The survival rates are
also lower in patients with pancreatic cancers of the body and tail
as compared with head lesions (14).
Primary SCC of pancreas is an extremely rare entity, with an
incidence of 0.5 to 2% of all exocrine pancreatic neoplasms
(15). The clinical presentation of
SCC of pancreas is similar to that of adenocarcinoma; it may arise
from chronic inflammation leading to malignant transformation of
squamous metaplasia, or from mixed adenosquamous carcinoma in which
the glandular components have disappeared, or from an
adenocarcinoma with squamous metaplasia where the tumor has a
potential to drift into both adenocarcinoma or SCC (16). The correct diagnosis of SCC of
pancreas requires a thorough workup to exclude another possible
primary metastatic SCC (10).
There is no standard therapy established for the
management of pancreatic SCC (10).
These tumors generally do not respond to chemotherapy or
radiotherapy and are very aggressive. Majority of the tumors may
not be resectable due to a delay in diagnosis (15). Published literature is available only
as case reports, and comprehensive clinical trials are not
available (17).
The cure rate for pancreatic cancer is very low at
7%, which makes the disease a vexing treatment challenge (18). Surgical resection is regarded as the
only potentially curative treatment and Stage I, IIA and IIB
pancreatic cancers are considered resectable (19). Neoadjuvant chemotherapy followed by
surgical exploration has been studied in patients with locally
advanced pancreatic cancer (20).
Gemcitabine is considered as the standard of care despite its
limited activity and modest treatment outcomes (12). It was shown to be effective in a
49-year-old patient with a metastatic SCC of the pancreas. Given as
a second line therapy after radiotherapy plus 5 FU and cisplatin,
gemcitabine improved the patient's health leading to an OS of 8
months (21). In an inoperable
patient, first-line therapy with gemcitabine and cisplatin followed
by second-line 5-FU and leucovorin showed a good survival rate
(22). Reports have shown improved
outcomes in patients with pancreatic cancer with a taxane and
gemcitabine combination (12,18). The
novel formulations of taxanes penetrate tumor cell mass at higher
concentrations due to their unique structure and may exert better
activity than conventional taxanes (12). Nab-paclitaxel, an albumin bound
formulation of paclitaxel, has been studied in pancreatic
adenocarcinoma (23,24) but no data is available on its use in
SCC. Kataoka et al demonstrated that nab-paclitaxel plus
gemcitabine combination therapy was effective in a 60-year-old
patient with adenosquamous carcinoma of the pancreas. However,
disease progression was noted after the completion of 4 cycles,
with an OS of 7 months (25).
Previous reports have shown a median OS of 7 months
in 8 patients with pancreatic SCC undergoing curative resection
(26,27). Brown et al (28) demonstrated a median OS of 7 months
(range 6–16 months) for patients who underwent curative resection.
A recent systematic review and pooled survival analysis conducted
by Ntanasis-Stathopoulos et al showed a median OS of 7
months in 54 patients with pancreatic SCC. This is the largest pool
of data regarding pancreatic SCC available in public domain till
date (29). The median age of
patients at diagnosis was 63 years (range 33–80 years); majority
(61.1%) of them were males; pain (77.8%) and weight loss (57.4%)
were the most common presenting symptoms. Most of the patients were
nonsmokers (77.8%) and most did not consume alcohol (70.4%).
Majority of the tumors were in the head of the pancreas (52.9%)
followed by tail (21.6%) and body (5.9%) . Resectable cases had
significantly better OS when compared with non-resectable cases (10
months versus 4 months, respectively) (29). OS without any treatment has been
dismal and has been reported as 3 months (22). Furthermore, there were 11 cases of
SCC of pancreatic tail in the pooled analysis, and the OS ranged
from 2 to 8 months. In comparison, our patient initially presented
with abdominal pain and weight loss, was a non-smoker and
non-alcoholic and showed a higher OS of 1 year. This is the first
case report on the use of NPLS in the treatment of primary SCC of
pancreatic tail. In the current report, the patient had a locally
advanced SCC of the pancreatic tail and was treated with an NPLS
and gemcitabine combination therapy followed by surgery, thereby
achieving a partial response. Overall, the treatment was
well-tolerated, and no serious adverse events (SAEs) were reported.
Neuropathy and anemia were observed, which resolved with
appropriate treatment.
PacliAqualip is an albumin-free NPLS formulation,
which is made from Lipids Generally Regarded As Safe (GRAS) by the
US Food and Drug Administration (30). NPLS has been formulated based on
‘Aqualip Technology’, which is patented in Europe, Japan and
Canada, while the filed US patent is under review. The Aqualip
technology results in the drug particles being nano-sized (~100 nm)
that allows the drug to penetrate the tumor tissue through leaky
vasculature without being attacked by the immune system. NPLS is
devoid of cremophor EL and ethanol, thus potentially reducing the
toxicities associated with cremophor for example severe
anaphylactoid hypersensitivity reactions, hyperlipidemia, abnormal
lipoprotein patterns, aggregation of erythrocytes and peripheral
neuropathy (31). Furthermore,
corticosteroid premedication is also not required. NPLS has been
shown to be effective in the treatment of metastatic breast cancer
(30). It is approved for the
treatment of metastatic or node-positive breast cancer, metastatic
ovarian cancer, metastatic non-small cell lung cancer, and
AIDS-related Kaposi's sarcoma.
In our case, the patient with locally advanced SCC
of pancreatic tail was treated with a novel nanosomal formulation
of paclitaxel, NPLS, in combination with gemcitabine in a
neoadjuvant setting followed by surgery. Overall, the current
report highlights the potential efficacy and safety of NPLS in the
treatment of SCC of pancreatic tail.
Presently, there is no definitive treatment
available for squamous cell carcinoma of pancreas. This case report
shows that NPLS, a novel albumin-free nanosomal paclitaxel
formulation devoid of cremophor EL and ethanol, can be a potential
treatment option for the treatment of locally advanced squamous
cell carcinoma of pancreatic tail.
Acknowledgements
The authors would like to thank Mr. Shreekant Sharma
(Lambda Therapeutic Research, Gujarat, India) for his support in
developing the concept/medical writing, and follow-up with the
journal/publisher, and Dr Venugopal Madhusudhana (Lambda
Therapeutic Research) for the additional editorial assistance.
Funding
The publication of this case report was supported by
a research grant from Intas Pharmaceuticals Ltd.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
SKDM, DKM, SM and CRRM planned and conducted the
study, performed the procedures, acquired the data and wrote the
manuscript. SKDM, DKM, SM, CRRM, DB and MAK conceived and designed
the case report. SKDM, DKM, SM, CRRM, DB and MAK reviewed the
manuscript, and SKDM served as the guarantor.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient's next of kin for the publication of this report as the
patient was deceased.
Competing interests
Drs. Deepak Bunger and Mujtaba A. Khan are employees
of Intas Pharmaceuticals Ltd.
References
|
1
|
Pourhoseingholi MA, Ashtari S, Hajizadeh
N, Fazeli Z and Zali MR: Systematic review of pancreatic cancer
epidemiology in Asia-Pacific Region: Major patterns in GLOBACON
2012. Gastroenterol Hepatol Bed Bench. 10:245–257. 2017.PubMed/NCBI
|
|
2
|
Kamisawa T, Wood LD, Itoi T and Takaori K:
Pancreatic cancer. Lancet. 388:73–85. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lin HL, Kuo LC, Chen CW, Lin YK and Lee
WC: Pancreatic tail cancer with sole manifestation of left flank
pain: A very rare presentation. Kaohsiung J Med Sci. 24:324–327.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
National Cancer Institute: Surveillance,
epidemiology, and end results program. Cancer stat facts, .
Pancreatic cancer. https://seer.cancer.gov/statfacts/html/pancreas.htmlJune
29–2018
|
|
5
|
Dhir V and Mohandas KM: Epidemiology of
digestive tract cancers in India IV. Gall bladder and pancreas.
Indian J Gastroenterol. 18:24–28. 1999.
|
|
6
|
Al-Shehri A, Silverman S and King KM:
Squamous cell carcinoma of the pancreas. Curr Oncol. 15:293–297.
2008.PubMed/NCBI
|
|
7
|
Schultheis AM, Nguyen GP, Ortmann M, Kruis
W, Büttner R, Schildhaus HU and Markiefka B: Squamous cell
carcinoma of the pancreas in a patient with germline BRCA2
mutation-response to neoadjuvant radiochemotherapy. Case Rep Oncol
Med. 2014:8605322014.PubMed/NCBI
|
|
8
|
Makarova-Rusher OV, Ulahannan S, Greten TF
and Duffy A: Pancreatic squamous cell carcinoma: A population-based
study of epidemiology, clinicopathologic characteristics and
outcomes. Pancreas. 45:1432–1437. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kodavatiganti R, Campbell F, Hashmi A and
Gollins SW: Primary squamous cell carcinoma of the pancreas: A case
report and review of the literature. J Med Case Reports. 6:295.
2012. View Article : Google Scholar
|
|
10
|
Mehta M, Sinha J, Ogawa M, Ganguly A,
Xiang D and Poddar N: Unusual Case of Squamous Cell Carcinoma of
Pancreas with Review of Literature. J Gastrointest Cancer.
46:426–429. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
NCCN Clinical Practice Guidelines in
Oncology. Pancreatic Adenocarcinoma. V1:2016, https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdfJune
30–2018
|
|
12
|
Belli C, Cereda S and Reni M: Role of
taxanes in pancreatic cancer. World J Gastroenterol. 18:4457–4465.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
American Cancer Society: Signs and
symptoms of pancreatic cancer. https://www.cancer.org/cancer/pancreatic-cancer/detection-diagnosis-staging/signs-and-symptoms.html28–February.
2018
|
|
14
|
Artinyan A, Soriano PA, Prendergast C, Low
T, Ellenhorn JD and Kim J: The anatomic location of pancreatic
cancer is a prognostic factor for survival. HPB (Oxford).
10:371–376. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gunjan D, Rana S, Chhabra P, Parghane R,
Kumar R, Dhalaria L, Mittal B and Bhasin D: Primary squamous cell
carcinoma of pancreas mimicking walled-off pancreatic necrosis. J
Dig Endosc. 7:17–19. 2016. View Article : Google Scholar
|
|
16
|
Ben Kridis W, Khanfir A, Toumi N, Ben Amar
M, Boudawara T and Frikha M: Primary squamous cell carcinoma of the
pancreas: A report of two cases and review of the literature.
Intern Med. 54:1357–1359. 2015. View Article : Google Scholar
|
|
17
|
Terada T: Adenosquamous Carcinoma and Pure
Squamous Cell Carcinoma of the Pancreas: Report of two Cases. Case
Rep Gastroenterol. 4:369–373. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Tempero MA: Multidisciplinary management
of pancreatic cancer. J Natl Compr Canc Netw. 13 Suppl 5:700–702.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chakraborty S and Singh S: Surgical
resection improves survival in pancreatic cancer patients without
vascular invasion- a population based study. Ann Gastroenterol.
26:346–352. 2013.PubMed/NCBI
|
|
20
|
Hackert T, Sachsenmaier M, Hinz U,
Schneider L, Michalski CW, Springfeld C, Strobel O, Jäger D, Ulrich
A and Büchler MW: Locally advanced pancreatic cancer: Neoadjuvant
therapy with folfirinox results in resectability in 60% of the
patients. Ann Surg. 264:457–463. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bideau K, Metges JP, Bayle S, André M,
Robaszkiewicz M, Lagarde N and Labat JP: Treatment of squamous cell
carcinoma of the pancreas with gemcitabine. Gastroenterol Clin
Biol. 30:1217–1220. 2006.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
22
|
De Souza AL and Saif MW: Squamous cell
carcinoma of the pancreas. JOP. 15:630–631. 2014.PubMed/NCBI
|
|
23
|
Von Hoff DD, Ervin T, Arena FP, Chiorean
EG, Infante J, Moore M, Seay T, Tjulandin SA, Ma WW, Saleh MN, et
al: Increased survival in pancreatic cancer with nab-paclitaxel
plus gemcitabine. N Engl J Med. 369:1691–1703. 2013. View Article : Google Scholar
|
|
24
|
Von Hoff DD, Ramanathan RK, Borad MJ,
Laheru DA, Smith LS, Wood TE, Korn RL, Desai N, Trieu V, Iglesias
JL, et al: Gemcitabine plus nab-paclitaxel is an active regimen in
patients with advanced pancreatic cancer: A phase I/II trial. J
Clin Oncol. 29:4548–4554. 2011. View Article : Google Scholar
|
|
25
|
Kataoka K, Matsubara H, Urano F, Okamura S
and Maeda M: Nab-paclitaxel+gemcitabine therapy for adenosquamous
carcinoma of the pancreas: An autopsy case. Nihon Shokakibyo Gakkai
Zasshi. 113:1777–1784. 2016.(In Japanese). PubMed/NCBI
|
|
26
|
Brijbassie A, Stelow E and Shami VM:
Squamous cell carcinoma of the pancreas: A case report and review
of literature. Gastroenterol Res. 7:102–104. 2014.
|
|
27
|
Serafini F, Rosemurgy AS II and Carey LC:
Squamous cell carcinoma of the pancreas. Am J Gastroenterol.
91:2621–2622. 1996.PubMed/NCBI
|
|
28
|
Brown HA, Dotto J, Robert M and Salem RR:
Squamous cell carcinoma of the pancreas. J Clin Gastroenterol.
39:915–919. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ntanasis-Stathopoulos I, Tsilimigras DI,
Georgiadou D, Kanavidis P, Riccioni O, Salla C, Psaltopoulou T and
Sergentanis TN: Squamous cell carcinoma of the pancreas: A
systematic review and pooled survival analysis. Eur J Cancer.
79:193–204. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ahmad A, Sheikh S, Ali SM, Paithankar M,
Mehta A and Nagarkar R: Nanosomal paclitaxel lipid suspension
demonstrates higher response rates compared to paclitaxel in
patients with metastatic breast cancer. J Cancer Sci Ther.
07:116–120. 2015.
|
|
31
|
Gelderblom H, Verweij J, Nooter K and
Sparreboom A: Cremophor EL: The drawbacks and advantages of vehicle
selection for drug formulation. Eur J Cancer. 37:1590–1598. 2001.
View Article : Google Scholar : PubMed/NCBI
|