Introduction
von Hippel Lindau (VHL) disease is caused by
inactivation of the VHL tumor suppressor gene, and subsequent
dysregulation of hypoxia-inducible factor expression, which leads
to multiple tumors commonly arising in the retina, cerebellum,
spinal cord, and kidney (1). Tumors
with different histopathologies can spatio-temporally occur in
various organs such as the central nervous system and pancreas
(2). Retinal hemangiomas in patients
with VHL disease are sight-threatening tumors in the young
(3). If the tumors are localized in
the peripheral retina, treatment options are basically retinal
photocoagulation, cryopexy, and radiotherapy as well as
photodynamic therapy (PDT) (4). In
addition, vitrectomy and local tumor resection are important
treatments, which can contribute to the preservation of patients'
vision (5). However, when a tumor
occurs at a juxtapapillary site, called a juxtapapillary retinal
capillary hemangioma (JRCH), treatment modalities may be more
sight-threatening than for a non-growing tumor without
complications (6), and a
watch-and-wait strategy may initially be chosen. JRCH, one of the
representative ocular manifestations in VHL disease (7), may cause various complications such as
macular edema, retinal exudation, exudative retinal detachment,
epiretinal membrane formation, and tractional retinal detachment
(8). Two percent of patients with
VHL disease and no retinal hemangiomas at the initial presentation
eventually develop isolated JRCH (9). There is a risk of blindness caused by
proliferative vitreoretinopathy and neovascular glaucoma (5) unless optimal treatments are conducted
in a timely manner to treat active retinal tumors. Although
ophthalmologists can conduct a number of primary treatments for
adult patients with JRCH, little is known about the clinical course
following retinal photocoagulation in JRCH of children. Indeed, it
is likely that JRCH can occur in patients with VHL disease at an
age of around 25 years, being earlier than in patients with
sporadic tumors (10,11). Herein, we report a young patient with
suspected VHL disease presenting with JRCH.
Case report
A 6-year-old Japanese girl with suspected VHL
disease was referred for the management of JRCH in her right eye.
Her father died of renal cancer due to VHL disease at the age of
40. Her paternal grandfather had been diagnosed with VHL disease.
Because it is highly penetrant, as 95% of patients with
characterized mutations in the VHL gene manifest clinical disorders
related to VHL disease by the age 60 years (12), we and the related clinical physicians
have observed the child patient as suspected VHL disease. Visual
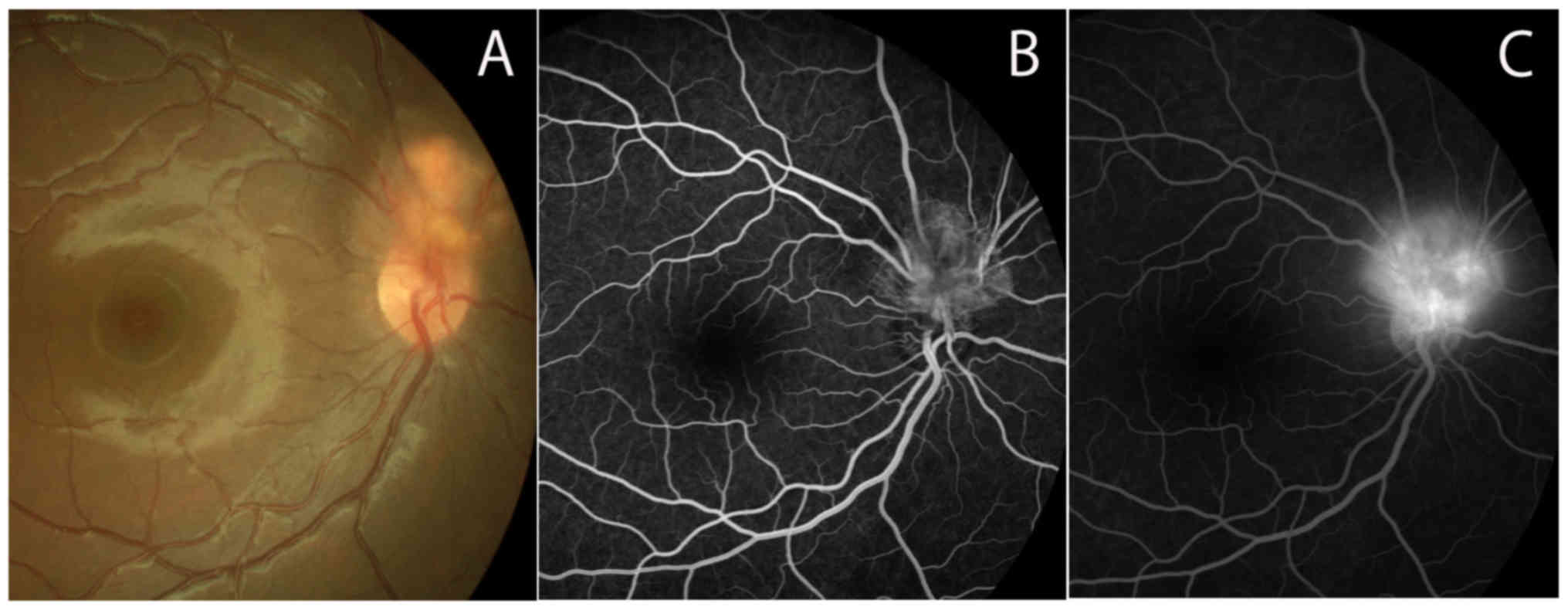
acuity was 20/20 in both eyes. The fundus showed an orange-colored
endophytic tumor located adjacent to the optic disc, measuring
about 2.5 mm, in the right eye (Fig.
1A). Fluorescein angiography (FA) revealed hyperfluorescence in
the tumor in an early phase (Fig.
1B), where marked dye leakage was noted in a late phase
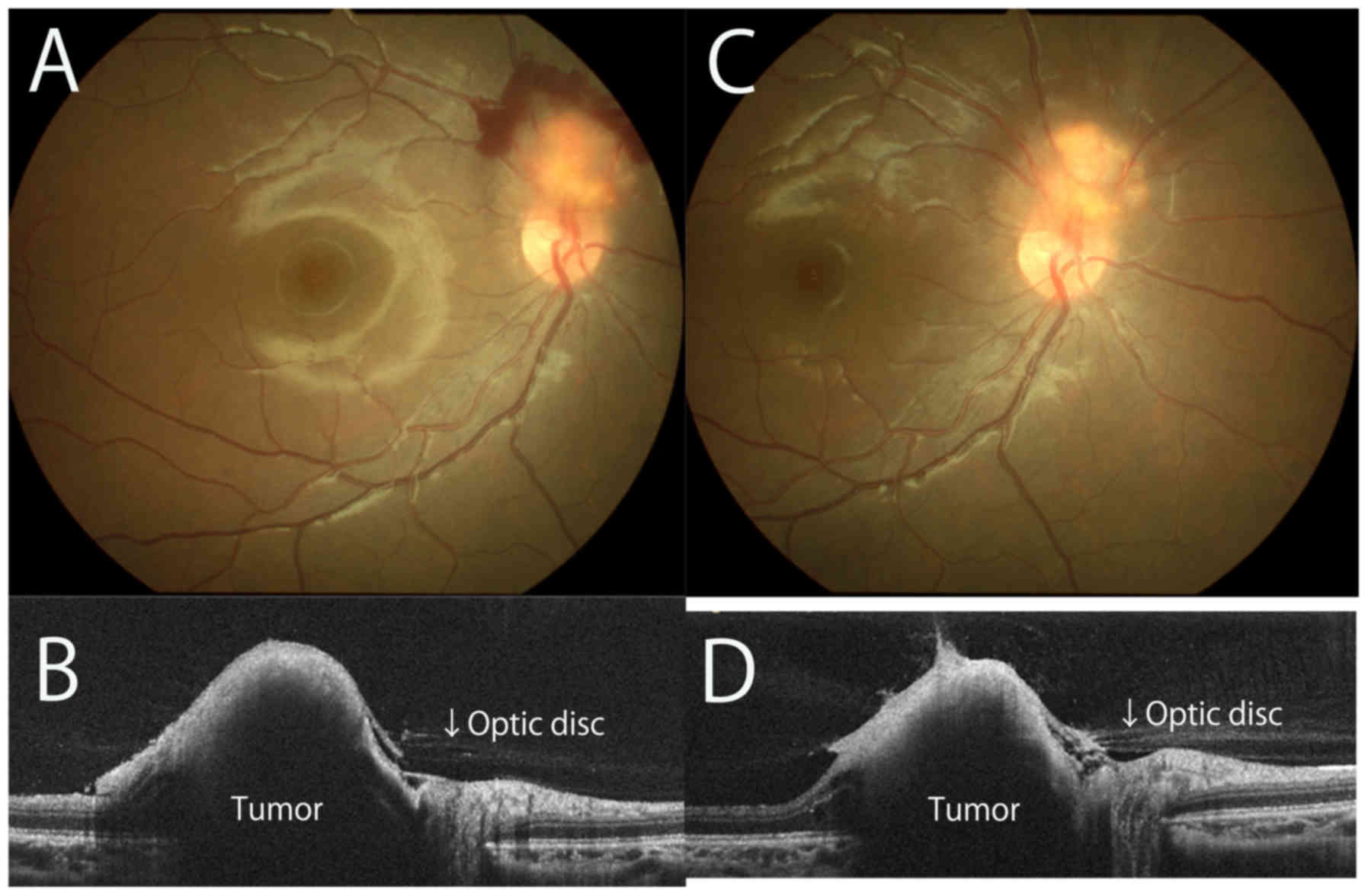
(Fig. 1C). Retinal hemorrhage,
however, occurred around JRCH, with a reddish appearance, 7 months
later (Fig. 2A). Optical coherence
tomography (OCT) demonstrated an elevated lesion in the superior
site of the optic disc (Fig. 2B).
Since these results suggested potential tumor activity, primary
treatments such as PDT, anti-vascular endothelial growth factor
(VEGF) therapy, and laser photocoagulation were considered. Indeed,
according to the previous report enrolling relatively large number
of the patients, laser photocoagulation is one of the mainstays in
treatments for retinal hemangioma (13). Moreover, this patient had undergone
fundus examination using a super field non-contact lens several
times. Therefore, direct photocoagulation of the tumor using the
non-contact lens was considered the possible first-line treatment
in this case. At the age of 7 years and 3 months, the patient
underwent direct yellow laser ablation of the tumor using a super
field non-contact lens (30 shots, 0.1 sec in duration, 200 µm spot
size, and 0.1–0.20 W power) after informed consent was obtained
from herself and her mother. The patient was orally asked to open
her eyes during ablation. She did not suffer from ocular pain
during treatment, and the ablation was safely completed. The
hemorrhage gradually resolved one month later. There was no
hemorrhage in the juxtapapillary region 6 months after
photocoagulation (Fig. 2C). The
tumor became paler than on initial presentation. OCT imaging showed
mild resolution of the elevated lesion with contraction of the
vitreoretinal interface over the tumor (Fig. 2D). Visual acuity remained 20/20 in
both eyes. There was no recurrence of the hemorrhage and no
enlargement of the tumor 9 months after the laser ablation.
Discussion
There are no established guidelines for the
treatment of JRCH (14). On the
other hand, eyes with de novo JRCH showed subsequent deterioration
of visual acuity compared with either eyes without retinal
involvement or eyes developing peripheral retinal hemangioma
without JRCH (9). Moreover,
multivariate logistic regression analyses verified the risk
factors: a younger age at the baseline visit, and a younger age at
the onset of ocular VHL disease (9).
Therefore, the therapeutic indication should be carefully and
strictly evaluated in a child with JRCH. Possible therapeutic
options are PDT, laser photocoagulation, anti-VEGF therapy,
radiotherapy, and cryopexy (6).
Since this case highlighted retinal hemorrhage
surrounding JRCH with a reddish color and marked dye leakage on FA,
treatments for the tumor were indicated because of the potential
for progression. PDT might be chosen as the first-line treatment
because it enables more selective vascular occlusion and reduces
damage to the optic disc (4).
However, PDT is a burdensome procedure for young patients. First of
all, general anesthesia is desirable to start the treatment for
children; however, the PDT procedure is quite complex under general
anesthesia. Second, PDT basically requires laser ablation with
contact lenses for 83 sec; however, wearing contact lenses under
local topical eye drop anesthesia is impossible for children. In
contrast, direct laser ablation is considered one of the
established ocular treatments for JRCH in VHL disease (7). In fact, clinical outcomes following
laser photocoagulation in children remain unknown, since this type
of hemangioma usually occurs in older age groups, such as
25-year-old patients (10,11). To the best of our knowledge, this
report describes the youngest patient with VHL disease treated with
direct laser ablation worldwide. Indeed, treatments for JRCH in VHL
disease are challenging because there are potential risks of
vision-related injury caused by the erroneous ablation of optic
disc tissues and papillo-macular bundles. Therefore, optimal
medical skills as well as the ability to establish favorable and
trusting relationships with young patients should be key to
overcome such complications. Therefore, the present results suggest
that conventional laser photocoagulation should be considered as
first-line treatment for JRCH.
It is debatable whether one session of laser
photocoagulation is sufficient to achieve satisfactory inactivation
and regression of the tumor, although this case was successfully
treated with one session of direct laser ablation. Indeed, there
will still be worries about optic disc injury, irreversible vision
loss, and visual field defects on conducting multiple sessions of
ablation. Therefore, careful observation was chosen after laser
photocoagulation in this case. If the tumor grows, the coloration
worsens, and retinal hemorrhage recurs, further laser ablation and
intravitreal anti-VEGF injection combined with sub-Tenon
triamcinolone acetonide injection (15) should be considered as second-line
treatment.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
SK and SI examined the patient, and SK wrote the
medical records and wrote the manuscript. SK was responsible for
surgical treatment. SI critically revised the paper. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
The Institutional Review Board at Hokkaido
University (Sapporo, Japan) waived ethical approval for the present
study, as it is a single case report.
Patient consent for publication
The patient provided consent for the publication of
the case details and associated images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lonser RR, Glenn GM, Walther M, Chew EY,
Libutti SK, Linehan WM and Oldfield EH: von Hippel-Lindau disease.
Lancet. 361:2059–2067. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Zou YU, Xu J and Zhang M: Long-term
follow-up and clinical course of a rare case of von Hippel-Lindau
disease: A case report and review of the literature. Oncol Lett.
11:3273–3278. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bastos-Carvalho A and Damato B: Images in
clinical medicine. Retinal hemangioblastoma in von Hippel-Lindau
disease. N Engl J Med. 363:6632010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schmidt-Erfurth UM, Kusserow C, Barbazetto
IA and Laqua H: Benefits and complications of photodynamic therapy
of papillary capillary hemangiomas. Ophthalmology. 109:1256–1266.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gaudric A, Krivosic V, Duguid G, Massin P,
Giraud S and Richard S: Vitreoretinal surgery for severe retinal
capillary hemangiomas in von hippel-lindau disease. Ophthalmology.
118:142–149. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kase S and Ishida S: Retinal capillary
hemangioma in von Hippel-Lindau disease: Current concept, diagnosis
and managements. J Transl Med Epidemiol. 2:10102014.
|
|
7
|
McCabe CM, Flynn HW Jr, Shields CL,
Shields JA, Regillo CD, McDonald HR, Berrocal MH, Gass JD and
Mieler WF: Juxtapapillary capillary hemangiomas. Clinical features
and visual acuity outcomes. Ophthalmology. 107:2240–2248. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Magee MA, Kroll AJ, Lou PL and Ryan EA:
Retinal capillary hemangiomas and von Hippel-Lindau disease. Semin
Ophthalmol. 21:143–150. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Toy BC, Agrón E, Nigam D, Chew EY and Wong
WT: Longitudinal analysis of retinal hemangioblastomatosis and
visual function in ocular von Hippel-Lindau disease. Ophthalmology.
119:2622–2630. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ridley M, Green J and Johnson G: Retinal
angiomatosis: the ocular manifestations of von Hippel-Lindau
disease. Can J Ophthalmol. 21:276–283. 1986.PubMed/NCBI
|
|
11
|
Wittebol-Post D, Hes FJ and Lips CJ: The
eye in von Hippel-Lindau disease. Long-term follow-up of screening
and treatment: recommendations. J Intern Med. 243:555–561. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Maher ER, Yates JR, Harries R, Benjamin C,
Harris R, Moore AT and Ferguson-Smith MA: Clinical features and
natural history of von Hippel-Lindau disease. Q J Med.
77:1151–1163. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Singh AD, Nouri M, Shields CL, Shields JA
and Perez N: Treatment of retinal capillary hemangioma.
Ophthalmology. 109:1799–1806. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Saitta A, Nicolai M, Giovannini A and
Mariotti C: Juxtapapillary retinal capillary hemangioma: new
therapeutic strategies. Med Hypothesis Discov Innov Ophthalmol.
3:71–75. 2014.PubMed/NCBI
|
|
15
|
Toyokawa N, Kimura H and Kuroda S:
Juxtapapillary capillary hemangioma treated by intravitreal
injection of bevacizumab combined with posterior subtenon injection
of triamcinolone acetonide. Jpn J Ophthalmol. 54:168–170. 2010.
View Article : Google Scholar : PubMed/NCBI
|