Introduction
Hepatopathy induced by vincristine, actinomycin D,
and cyclophosphamide (VAC) is a potentially lethal complication of
VAC chemotherapy for pediatric malignancy, including
rhabdomyosarcoma (RMS), empirically managed by conventional
anticoagulation therapy and liver-supporting agents. VAC-induced
hepatopathy is pathophysiologically similar to sinusoidal
obstruction syndrome/veno-occlusive disease (SOS/VOD) in the
transplant setting, in which the primary insult is injury to the
sinusoidal endothelial cells triggered by anticancer drug toxicity
and proinflammatory cytokine release (1). The incidence rate of VAC-induced
hepatopathy in RMS has been reported to be 1.2–15.4% (2–4). More
efficient management than the current empirical one is required to
avoid threat to life and minimize delays and dose reduction in
chemotherapy. Thrombomodulin is a thrombin receptor on the
endothelial cell surface. Recombinant thrombomodulin (rTM) consists
of the active extracellular domain of thrombomodulin, including the
N-terminal lectin-like domain with unique anti-inflammatory
properties (5,6). In particular, rTM administration exerts
beneficial effects on the control of transplantation-associated
thrombotic microangiopathy and SOS/VOD resulting from endothelial
damage, coagulability, and exaggerated cytokine production
(7). Nevertheless, the effect of rTM
in VAC-induced hepatopathy remains unknown owing to the absence of
reports.
We presented here a pediatric case of VAC-induced
hepatopathy associated with coagulopathy and inflammation that was
successfully controlled by the administration of rTM and
conventional dose of prednisolone. The pathogenesis and management
of VAC-induced hepatopathy with inflammatory cytokine profile were
discussed in concert with the treatment response and literature
review. Consent for publication of the case report was obtained
from the patient and his mother.
Case report
Fig. 1 shows the
timeline. A-15-year-old male with paratesticular RMS exhibiting no
evidence of metastasis to other organs, including the liver,
received adjuvant chemotherapy comprising four cycles of VAC (total
cumulative dose of cyclophosphamide, 4.8 g/m2) followed
by four cycles of vincristine and actinomycin D with a total
duration of 22 weeks with or without local radiation therapy
(8). He had no personal and family
history of injury or illness. During the 13th week of schedule for
adjuvant chemotherapy from which the first cycle of vincristine and
actinomycin D started after four cycles of VAC, he presented with
refractory thrombocytopenia, along with subsequent abdominal
tenderness and non-neutropenic fever. He was treated empirically
with broad-spectrum intravenous antibiotics (cefepime) and
continuously with platelet transfusion.
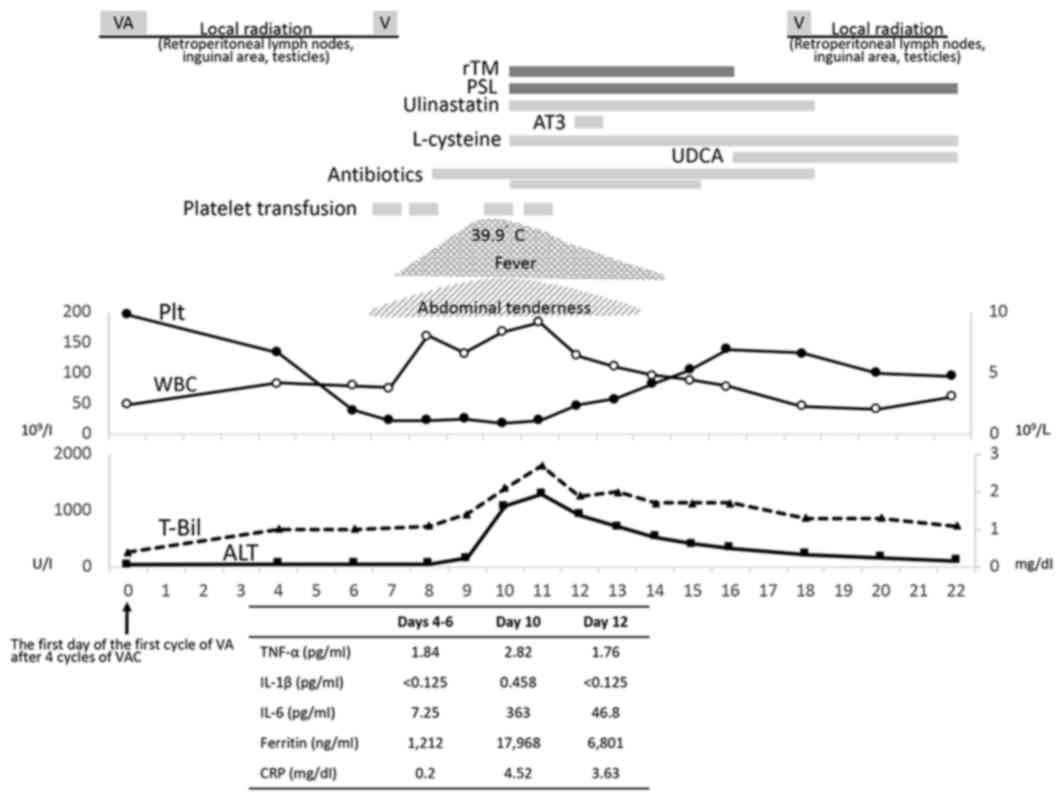 | Figure 1.Treatment course and cytokine levels
of the patient. AC, actinomycin D and cyclophosphamide; VA,
vincristine and actinomycin D; V, vincristine; Plt, platelet; WBC,
white blood cell; AST, aspartate transaminase; ALT, alanine
transaminase; T-Bil, total bilirubin; CRP, C-reactive protein;
TNFα, tumor necrosis factor-α; IL-1β, interleukin-1β; IL-6,
interleukin-6; rTM, recombinant thrombomodulin; PSL, prednisolone;
AT3, antithrombin III; UDCA, ursodeoxycholic acid. |
At day 3 of the 14th week (at 10 days after
administration of vincristine and actinomycin D or at 2 days after
administration of vincristine alone), full-blown hepatic
dysfunction and coagulopathy were noted, along with persistent
fever up to 39.6°C (leukocyte count, 8.37×109/l;
hemoglobin, 8.1 g/dl; platelet count, 18×109/l;
fibrinogen, 305 mg/dl; prothrombin time-international normalized
ratio, 1.82; antithrombin III, 73%; fibrin/fibrinogen degradation
products, 20.18 µg/ml; aspartate transaminase [AST], 1961 U/l;
alanine aminotransferase [ALT], 1084 U/l; total bilirubin [T-Bil],
2.1 mg/dl; C-reactive protein [CRP], 4.52 mg/dl; ferritin, 17,968
ng/ml). This condition fulfilled the diagnostic criteria for
disseminated intravascular coagulation (DIC) (9) and was strongly suggestive of
hemophagocytic lymphohistiocytosis (HLH) (four of eight items met
the Histiocyte Society HLH-2004 criteria, with highly elevated
ferritin level) (10,11). Furthermore, the diagnostic criteria
for ‘very severe’ SOS/VOD were met in accordance with the European
Society for Blood and Marrow Transplantation diagnostic criteria
for hepatic SOS/VOD in children (1).
At this stage, we initiated the administration of rTM (380
U/kg/day) to control DIC on the basis of absent hemorrhagic
diathesis and of prednisolone (PSL) (1.8 mg/kg/day) to control HLH,
with supportive therapies including blood transfusion;
administration of ulinastatin, antithrombin III, and L-cysteine;
and strengthened antibacterial therapy (to add amikacin
sulfate).
His condition improved after the therapy, with
defervescence and amelioration of abdominal pain. Levels of T-Bil,
AST, ALT, and CRP improved after peaking at 2.7 mg/dl, 1,963 U/l,
1,292 U/l, and 5.5 mg/dl, respectively, on the subsequent day of
rTM and PSL therapy. Furthermore, levels of coagulation markers and
serum ferritin rapidly improved. The first abdominal Doppler
ultrasonography performed at 2 days after rTM and PSL
administration revealed bidirectional blood flow of the left portal
vein. His body weight increased by 7% above the baseline value.
Results of hepatitis virus panel were negative, and blood cultures
were sterile. Liver biopsy for pathological confirmation was not
performed in consideration of thrombocytopenia and coagulopathy.
After day 7 of rTM therapy, the schedule for radio- and
chemotherapy was restarted at 1 week later with the dose of
vincristine in full and actinomycin D in half. Although the patient
had two episodes of isolated fever during vincristine
administration, severe hepatopathy with inflammation and
coagulopathy never recurred. PSL was started to be tapered and
finished at 1 month later. He is alive and well on disease-free
state of RMS at the age of 16 years and 6 months.
Serum concentrations of proinflammatory cytokines
were measured using an established method by LSI Medience
Corporation (Tokyo, Japan) with kits from R&D Systems, Inc.
(Minneapolis, MN, USA). The levels of tumor necrosis factor-α
(TNF-α) (QuantiGlo ELISA Human TNF-α Immunoassay with a lower
detection limit of 0.55 pg/ml: Non-detectable [ND] to 9.03 pg/ml in
healthy volunteers), interleukin-1β (IL-1β) (Quantikine HS ELISA
Human IL-1β/IL-1F2 Immunoassay with a lower detection limit of
0.125 pg/ml: ND to 0.606 pg/ml in healthy volunteers), and
interleukin-6 (IL-6) (QuantiGlo ELISA Human IL-6 Immunoassay with a
lower detection limit of 0.30 pg/ml: ND to 5.84 pg/ml in healthy
volunteers) were as follows: 1.84, <0.125, and 7.25 pg/ml at day
5 of the 13th week (before the event); 2.82, 0.458, and 363 pg/ml
at day 3 of the 14th week (day of rTM and PSL therapy initiation
before administration); and 1.76, <0.125, and 46.8 pg/ml at day
5 of the 14th week (2 days after rTM and PSL therapy initiation),
respectively. The cytokine profile showed an increase with
hepatopathy development and a decrease immediately after drug
initiation.
Discussion
SOS/VOD is a life-threatening complication of
anticancer drug administration that was originally identified as a
transplant-related endothelial disease. In the liver, recruited
monocytes/macrophages and resident Kupffer cells are thought to
play important roles on the insulted sinusoidal walls (12,13),
with activated Kupffer cells having been confirmed to secrete
IL-1β, IL-6, and TNF-α (14–16).
Particularly in children, SOS/VOD can also occur as
a complication of conventional radio- and chemotherapy outside of
the transplant setting with recurrent association with actinomycin
D, vincristine, cyclophosphamide, and 6-mercaptopurine (1). There was little recognition of the risk
of VAC-induced hepatopathy among children with RMS until the case
report of Kanwar et al (17).
Subsequently, a clinical trial performed by the Intergroup
Rhabdomyosarcoma Study Group reported an incidence rate of 5.3%
(4). Table I shows hepatopathy in conventional
chemotherapy regimen for RMS (2–4,18–22).
Most cases were supportively managed mainly by conventional
anticoagulation. Therapies targeting inflammation have scarcely
been reported to date. One case was reported to be treated with
high-dose methylprednisolone. Although the patient recovered, the
condition continued to worsen up to 4 days after therapy initiation
(22). Defibrotide, which protects
the endothelial cells from continued damage due to cytotoxic drugs
and TNF-α, was shown to be a feasible therapeutic option for both
transplant- and non-transplant-associated SOS/VOD (23). In a review, when defibrotide was
administered in two patients, one died, whereas the other recovered
after intensive care including ventilatory support (4,23).
Nonetheless, defibrotide is yet to be licensed for clinical use in
Japan.
 | Table I.VAC-induced hepatopathy in
rhabdomyosarcoma reviewed. |
Table I.
VAC-induced hepatopathy in
rhabdomyosarcoma reviewed.
| Age, year | Sex | Tumor site | Therapy for
hepatotherapy other than supportive carea | Duration of
hepatotherapy | Outcome of
hepatotherapy | Further therapy | Outcome of RMS | (Refs.) |
|---|
| 0.3 |
|
|
|
| R | VIC/VTC | NED | (4) |
| 1 | M | Thigh | Gabexate
mesilate | 1 month | R | VAC | NED | (19) |
| 1.1 |
|
| Defibrotide |
| Dead |
| Dead | (4) |
| 1.5 |
|
|
|
| R | VAC | NED | (4) |
| 1.7 |
|
|
|
| R | Off | NED | (4) |
| 1.7 |
|
| Ventilator |
| Dead |
| Dead | (4) |
| 1.8 |
|
|
|
| R | VIE | NED | (4) |
| 1.8 | M | Face | High-dose
methylprednisolone | 3–4 weeks | R | VECb | NED | (22) |
| 2 | M | Face | Abdominal
paracentesis | 2 weeks | R | VIE | NED | (21) |
| 2.3 |
|
| Ventilator |
| R | VTC/VIE | NED | (4) |
| 2.4 |
|
|
|
| R | Off | NED | (4) |
| 2.7 |
|
| Ventilator |
| R | VIE | NED | (4) |
| 2.7 |
|
|
|
| R | VIE | NED | (4) |
| 3.8 |
|
|
|
| R | VAC | NED | (4) |
| 3.8 | F | Head | Thoracentesis,
activated factor IX | >1 month | Left | VIE | NED | (17) |
|
|
|
| concentrate,
ventilator |
| ptosis |
| 4.0 |
|
| Ventilator |
| R | VIE | NED | (4) |
| 4.7 |
|
|
|
| Dead |
| Dead | (4) |
| 5.0 |
|
|
|
| Dead |
| Dead | (4) |
| 6.1 |
|
|
|
| R | Off | NED | (4) |
| 9 | F | Limb | Defibrotide,
abdominal paracentesis, |
| R | Off | NED | (23) |
|
|
|
| ventilator |
| 12.9 |
|
|
|
| R | VIE | Relapse | (4) |
| 14.3 |
|
|
|
| R | VAC | NED | (4) |
| 15.5 |
| Para | rTM, PSL | 1 week | R | VAC | NED | Index |
|
|
| testicular |
|
|
|
|
| case |
| 17.9 |
|
|
|
| R | VAC | NED |
|
Our case indicated the marked hyperferritinemia,
which was substantiated with hypercytokinemia, as severe
inflammation. We used a combination of rTM and PSL, and all of the
patient's symptoms and laboratory data, including pro-inflammatory
cytokine profile, immediately improved after the administration of
these drugs. rTM itself has been reported to have a unique
anti-inflammatory property by binding to high-mobility group box 1
protein (HMGB1), which is secreted by activated monocytes and
macrophages (6,24). However, the effect of systemic
corticosteroid treatment was observed to be confined to reduction
in extracellular HMGB1 expression, but not in intracellular
expression (25). Kurokohchi et
al (26) reported that rTM-but
not corticosteroid-for fulminant hepatic failure, which is also
characterized by severe liver inflammation, was sufficiently
effective. From the viewpoint of relatively long duration before
withdrawal and various side effects, corticosteroid use is best
avoided, if possible. In addition, although the in vitro
anti-inflammatory effect of ulinastatin has been shown (27), its effect on liver inflammation in
the clinical setting has not yet been reported.
We presume that rTM could ameliorate not only
coagulopathy but also excessive inflammation via suppression of
proinflammatory cytokines. As a novel treatment for VAC-associated
hepatopathy with inflammatory profile, rTM could become promising
for reducing treatment-related mortality and, more substantially,
minimizing delays and dose reduction in chemotherapy for RMS.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
TK analyzed the medical records of the patients,
measured cytokine levels of the patient and was the principal
writer primarily responsible for drafting the manuscript. MN, HN
and RF were responsible for the clinical management of the patient
with helpful discussion for the completion of the study. RF created
the high-resolution figure. HN supervised the project. SO
interpreted the data collected by TK, was involved in drafting the
manuscript critically for important intellectual content and
supervised the conduct of the present study.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
General consent for research including publication
of the case report was obtained from the patient and his
mother.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
VAC
|
vincristine, actinomycin D, and
cyclophospha-mide
|
|
SOS/VOD
|
sinusoidal obstruction
syndrome/veno-occlusive disease
|
|
rTM
|
recombinant thrombomodulin
|
|
AST
|
aspartate transaminase
|
|
ALT
|
alanine aminotransferase
|
|
T-Bil
|
total bilirubin
|
|
CRP
|
C-reactive protein
|
|
DIC
|
disseminated intravascular
coagulation
|
|
HLH
|
hemophagocytic lymphohistiocytosis
|
|
PSL
|
prednisolone
|
|
TNF-α
|
tumor necrosis factor-α
|
|
ND
|
non-detectable
|
|
IL-1β
|
interleukin-1β
|
|
IL-6
|
interleukin-6
|
|
HMGB1
|
high-mobility group box 1 protein
|
References
|
1
|
Corbacioglu S, Carreras E, Ansari M,
Balduzzi A, Cesaro S, Dalle JH, Dignan F, Gibson B, Guengoer T,
Gruhn B, et al: Diagnosis and severity criteria for sinusoidal
obstruction syndrome/veno-occlusive disease in pediatric patients:
A new classification from the European society for blood and marrow
transplantation. Bone Marrow Transplant. 53:138–145. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ortega JA, Donaldson SS, Ivy SP, Pappo A
and Maurer HM: Venoocclusive disease of the liver after
chemotherapy with vincristine, actinomycin D, and cyclophosphamide
for the treatment of rhabdomyosarcoma. A report of the intergroup
rhabdomyosarcoma study group. Childrens cancer group, the pediatric
oncoloy group, and the pediatric intergroup statistical center.
Cancer. 79:2435–2439. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sulis ML, Bessmertny O, Granowetter L,
Weiner M and Kelly KM: Veno-occlusive disease in pediatric patients
receiving actinomycin D and vincristine only for the treatment of
rhabdomyosarcoma. J Pediatr Hematol Oncol. 26:843–846.
2004.PubMed/NCBI
|
|
4
|
Arndt C, Hawkins D, Anderson JR, Breitfeld
P, Womer R and Meyer W: Age is a risk factor for
chemotherapy-induced hepatopathy with vincristine, dactinomycin,
and cyclophosphamide. J Clin Oncol. 22:1894–1901. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Saito H, Maruyama I, Shimazaki S, Yamamoto
Y, Aikawa N, Ohno R, Hirayama A, Matsuda T, Asakura H, Nakashima M
and Aoki N: Efficacy and safety of recombinant human soluble
thrombomodulin (ART-123) in disseminated intravascular coagulation:
Results of a phase III, randomized, double-blind clinical trial. J
Thromb Haemost. 5:31–41. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Abeyama K, Stern DM, Ito Y, Kawahara K,
Yoshimoto Y, Tanaka M, Uchimura T, Ida N, Yamazaki Y, Yamada S, et
al: The N-terminal domain of thrombomodulin sequesters
high-mobility group-B1 protein, a novel anti-inflammatory
mechanism. J Clin Invest. 115:1267–1274. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Loghmani H and Conway EM: Exploring
traditional and nontraditional roles for thrombomodulin. Blood.
132:148–158. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Walterhouse DO, Pappo AS, Meza JL,
Breneman JC, Hayes-Jordan AA, Parham DM, Cripe TP, Anderson JR,
Meyer WH and Hawkins DS: Shorter-duration therapy using
vincristine, dactinomycin, and lower-dose cyclophosphamide with or
without radiotherapy for patients with newly diagnosed low-risk
rhabdomyosarcoma: A report from the soft tissue sarcoma committee
of the children's oncology group. J Clin Oncol. 32:3547–3552. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wada H, Takahashi H, Uchiyama T, Eguchi Y,
Okamoto K, Kawasugi K, Madoiwa S and Asakura H; Diagnostic and
therapeutic guidelines for hemophagocytic lymphohistiocytosis, :
The approval of revised diagnostic criteria for DIC from the
Japanese Society on thrombosis and hemostasis. Thromb J. 15:172017.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Henter JI, Horne A, Aricó M, Egeler RM,
Filipovich AH, Imashuku S, Ladisch S, McClain K, Webb D, Winiarski
J and Janka G: HLH-2004: Diagnostic and therapeutic guidelines for
hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer.
48:124–131. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Allen CE, Yu X, Kozinetz CA and McClain
KL: Highly elevated ferritin levels and the diagnosis of
hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer.
50:1227–1235. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
DeLeve LD, Shulman HM and McDonald GB:
Toxic injury to hepatic sinusoids: Sinusoidal obstruction syndrome
(veno-occlusive disease). Semin Liver Dis. 22:27–42. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
DeLeve LD, Ito Y, Bethea NW, McCuskey MK,
Wang X and McCuskey RS: Embolization by sinusoidal lining cells
obstructs the microcirculation in rat sinusoidal obstruction
syndrome. Am J Physiol Gastrointest Liver Physiol. 284:G1045–G1052.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Szabo G and Petrasek J: Inflammasome
activation and function in liver disease. Nat Rev Gastroenterol
Hepatol. 12:387–400. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Schmidt-Arras D and Rose-John S: IL-6
pathway in the liver: From physiopathology to therapy. J Hepatol.
64:1403–1415. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sato K, Hall C, Glaser S, Francis H, Meng
F and Alpini G: Pathogenesis of kupffer cells in cholestatic liver
injury. Am J Pathol. 186:2238–2247. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kanwar VS, Albuquerque ML, Ribeiro RC,
Kauffman WM and Furman WL: Veno-occlusive disease of the liver
after chemotherapy for rhabdomyosarcoma: Case report with a review
of the literature. Med Pediatr Oncol. 24:334–340. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Adachi N and Matsuda I: Veno-occlusive
disease of the liver after combined adjuvant chemotherapy for a
1-year-old boy with rhabdomyosarcoma: Potential usefulness of the
gabexate mesylate (FOY). J Pediatr Gastroenterol Nutr. 14:314–318.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
D'Antiga L, Baker A, Pritchard J, Pryor D
and Mieli-Vergani G: Veno-occlusive disease with multi-organ
involvement following actinomycin-D. Eur J Cancer. 37:1141–1148.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Cecen E, Uysal KM, Ozguven A, Gunes D,
Irken G and Olgun N: Veno-occlusive disease in a child with
rhabdomyosarcoma after conventional chemotherapy: Report of a case
and review of the literature. Pediatr Hematol Oncol. 24:615–621.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chen IL, Yang SN, Hsiao CC, Wu KS and
Sheen JM: Treatment with high-dose methylprednisolone for hepatic
veno-occlusive disease in a child with rhabdomyosarcoma. Pediatr
Neonatol. 49:141–144. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Choi A, Kang YK, Lim S, Kim DH, Lim JS and
Lee JA: Severe hepatic sinusoidal obstruction syndrome in a child
receiving vincristine, actinomycin-D, and cyclophosphamide for
rhabdomyosarcoma: Successful treatment with defibrotide. Cancer Res
Treat. 48:1443–1447. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kernan NA, Richardson PG, Smith AR,
Triplett BM, Antin JH, Lehmann L, Messinger Y, Liang W, Hume R,
Tappe W, et al: Defibrotide for the treatment of hepatic
veno-occlusive disease/sinusoidal obstruction syndrome following
nontransplant-associated chemotherapy: Final results from a post
hoc analysis of data from an expanded-access program. Pediatr Blood
Cancer. 65:e272692018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Scaffidi P, Misteli T and Bianchi ME:
Release of chromatin protein HMGB1 by necrotic cells triggers
inflammation. Nature. 418:191–195. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ulfgren AK, Grundtman C, Borg K,
Alexanderson H, Andersson U, Harris HE and Lundberg IE:
Down-regulation of the aberrant expression of the inflammation
mediator high mobility group box chromosomal protein 1 in muscle
tissue of patients with polymyositis and dermatomyositis treated
with corticosteroids. Arthritis Rheum. 50:1586–1594. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kurokohchi K, Imataki O and Kubo F:
Anti-inflammatory effect of recombinant thrombomodulin for
fulminant hepatic failure. World J Gastroenterol. 21:8203–8207.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wei F, Liu S, Luo L, Gu N, Zeng Y, Chen X,
Xu S and Zhang D: Anti-inflammatory mechanism of ulinastatin:
Inhibiting the hyperpermeability of vascular endothelial cells
induced by TNF-α via the RhoA/ROCK signal pathway. Int
Immunopharmacol. 46:220–227. 2017. View Article : Google Scholar : PubMed/NCBI
|














