Introduction
Methotrexate is a cell-cycle specific agent which
disrupts the metabolism of folic acid and DNA synthesis by
inhibiting the enzyme dihydrofolate reductase. It is a commonly
used antimetabolite in the treatment of adult and pediatric
cancers, including lymphomas, acute lymphoblastic leukemias and
osteosarcomas (1). The incidence of
acute MTX neurotoxicity is reportedly 3–10% and it depends on the
dose, frequency and route of administration of MTX as well as the
prophylactic use of leucovorin (2).
Acute encephalopathy usually develops within 5 to 14 days after HD
MTX, commonly presenting as nausea, headache, seizures, altered
mental status or stroke-like symptoms. Choreoathetosis is an
unusual and severe presentation of MTX neurotoxicity, and to our
knowledge, has not been reported in adults (3,4).
Case report
A 46 year old woman who presented with confusion and
lethargy of 3 weeks duration was diagnosed with an isolated relapse
of lymphoma involving the central nervous system (CNS). She had a
history of diffuse large B-cell lymphoma (DLBCL) of the breast 12
years ago and was treated then with six cycles of R-CHOP
chemotherapy (which included rituximab, cyclophosphamide,
doxorubicin, vincristine and prednisolone) and localized
radiotherapy to the breast. She did not receive CNS prophylaxis at
initial diagnosis. She remained in clinical remission for ten years
until she relapsed in the lumbosacral plexus. She received salvage
chemotherapy with 4 cycles of R-ESHAP (rituximab, etoposide,
methylprednisolone, cytarabine and cisplatin) and went into
complete remission.
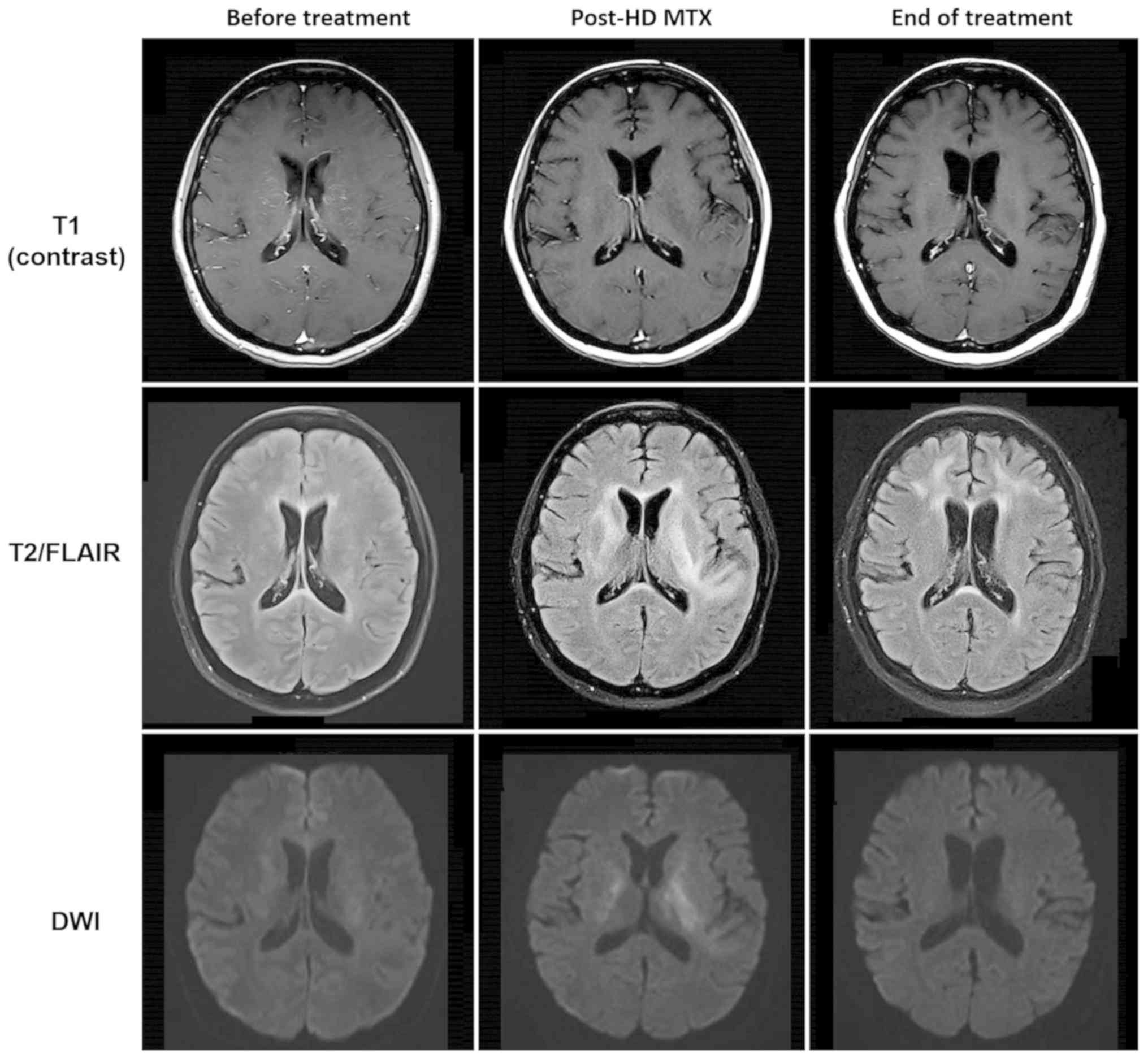
At the current presentation, gadolinium-enhanced
magnetic resonance imaging (MRI) of the brain revealed subcortical
white matter hyperintensities on fluid-attenuated inversion
recovery (FLAIR) sequence with associated vascular and
leptomeningeal enhancement consistent with lymphoma recurrence
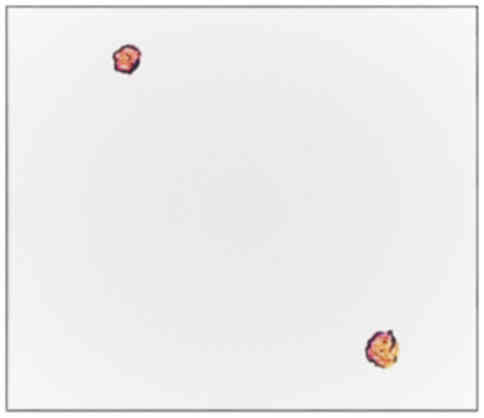
(Fig. 1). Diagnostic lumbar puncture
confirmed the presence of CD20-positive lymphomatous large B cells,
typical of leptomeningeal disease (Fig.
2). These large cells also intensely co-expressed CD79a with a
Ki-67 proliferation fraction in the region of 60–70% on
immunohistochemistry. Flow cytometry analysis was negative for
clonal B lymphocytic cells however, this might have been a false
negative result due to either limited CSF sample or rapid
degeneration of viable lymphocytes. There was no scintigraphic
evidence of lymphoma recurrence elsewhere on whole body 18F-FDG
PET/CT scan.
She was commenced on dexamethasone, intravenous
rituximab and HD MTX infusion at 3.5 g/m2 given over 3 h
based on Shah's protocol for treatment of newly-diagnosed primary
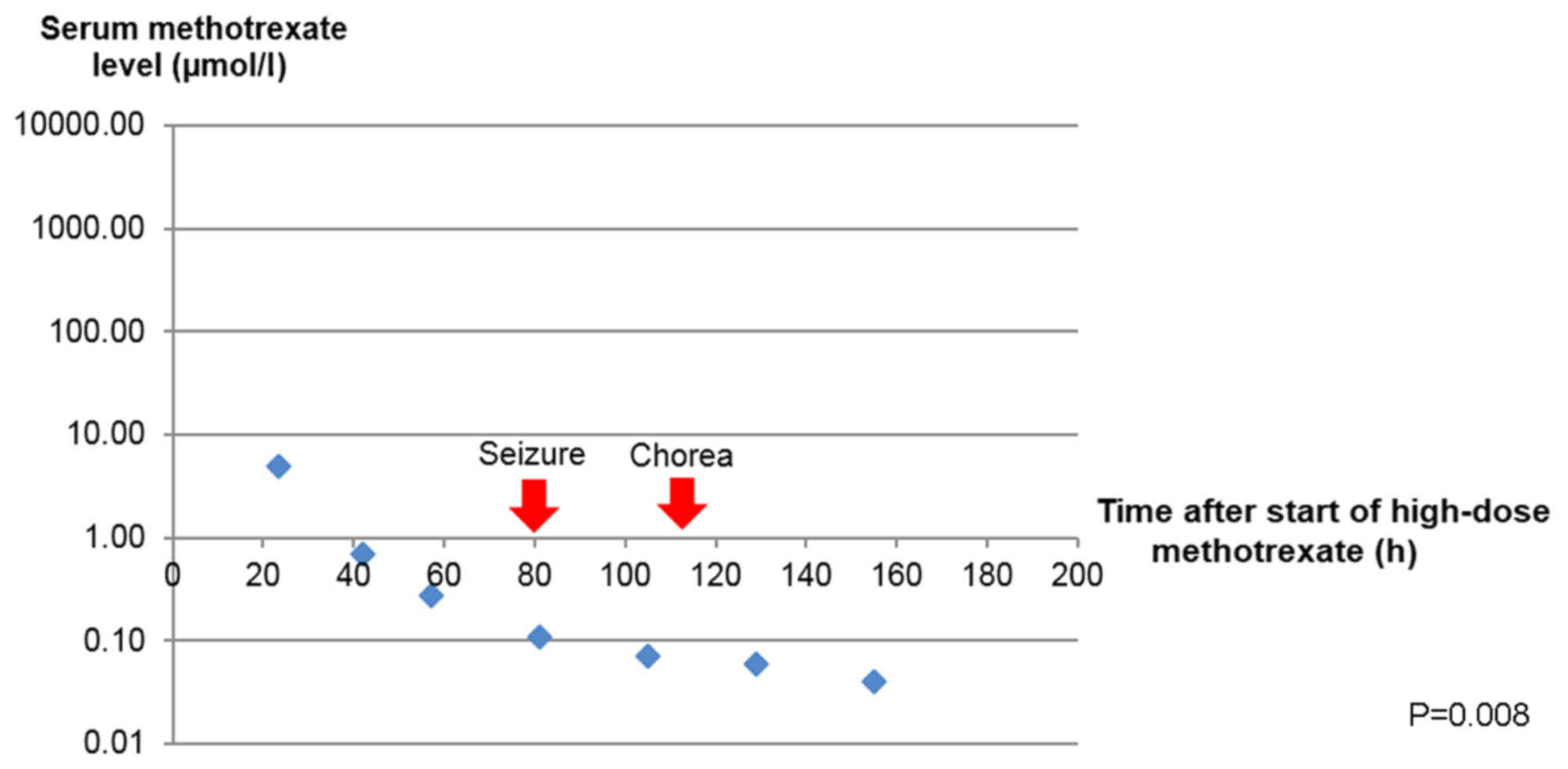
CNS lymphoma (5). IV folinic acid 30
mg 6-hourly was given 24 h after the start of HD MTX infusion until
MTX levels <0.05 µmol/l had been achieved (Fig. 3). There was no incidence of toxicity
observed on serial monitoring of plasma MTX concentrations. The
decrease in serum methotrexate level with time after the start of
HD MTX, compared to the baseline methotrexate level was analyzed
with Friedman test. All statistical analyses were performed using
SPSS17.0 software. A P-value <0.05 (two-tailed) was considered
to be of statistical significance.
Four days after HD MTX infusion, she developed
sudden jerking movements of the upper limbs with drooling of saliva
and extensor posturing of the body. She suffered another complex
partial seizure with secondary generalization a few hours later,
which aborted spontaneously. She did not have any fever,
hypoglycaemia or signs of meningism. Neurological examination was
otherwise normal. An urgent CT scan of the brain did not identify
any new intracranial lesions nor was there any epileptiform
activity on an electroencephalogram (EEG) performed the following
day. She was subsequently treated with levetiracetam and there had
been no recurrence of seizure since.
Two days later, she was observed to have prolonged
involuntary and irregular movements involving bilateral upper
extremities with intermittent writhing of the neck and trunk, which
would resolve when she slept but recurred when she was awake. A
repeat MRI of the brain showed extensive T2 and FLAIR
hyperintensities with bilateral and symmetrical involvement of the
basal ganglia and periventricular white matter, some of which
demonstrated restricted diffusion without any associated solid
enhancement. Notably, the previously seen vascular and
leptomeningeal enhancement have improved. Further investigations to
exclude other causes of choreoathetosis were performed: serum
ceruloplasmin, thyroid function, creatine kinase and ferritin were
normal, anti-streptolysin O titre (ASOT) and autoimmune workup were
negative; as well as a peripheral blood film which did not yield
any acanthocytes. A neurologist was consulted for her movement
disorder and she was started on tetrabenazine 12.5 mg bd with
complete resolution of her symptoms thereafter.
She was successfully rechallenged with HD MTX at a
lower dose of 2.5 g/m2 at week 3 without any recurrence
of neurotoxicity, completing a total of 5 biweekly doses. In
addition, she received 2 doses of intrathecal MTX 12 mg at weeks 7
and 9 without any complications. MRI brain was repeated after two
months which had shown near complete resolution of white matter
changes in the basal ganglia while her lymphoma remained in
clinical and radiological remission.
Discussion
We described a case of acute, reversible
methotrexate neurotoxicity in an adult patient with lymphoma who
was successfully rechallenged with HD MTX. The differential
diagnoses of chorea are broad and can be caused by any structural,
metabolic, infectious, autoimmune or malignant involvement of the
basal ganglia (6). The bilateral and
symmetrical involvements of the basal ganglia in addition to the
periventricular white matter were severe and directly accounted for
the choreoathetosis observed (7).
The putamen and globus pallidus were high in metabolic activity due
to an abundance of vascular supply, mitochondria and
neurotransmitters compared with other regions of the brain
(8). Therefore, this was more
suggestive of a toxic-metabolic cause of acute leukoencephalopathy
rather than a unilateral neoplastic process.
The diagnosis of MTX-induced encephalopathy in our
patient was made based on transient symptoms with full recovery,
typical radiographic features and exclusion of other causes after
an extensive panel of investigations. We reviewed a series of case
reports whereby chorea was one of the main presenting symptoms and
summarized them in the tables below (Tables I and II). All the previously reported patients
were diagnosed with pediatric ALL on intrathecal MTX with or
without HD MTX prior to their neurotoxic symptoms (9–11). MRI
brain typically showed focal areas of restricted diffusion,
particularly in the basal ganglia and centrum semiovale, which
disappeared on follow up imaging. These radiographic findings of
transient restricted diffusion in the absence of vascular or
perfusion changes were consistent with reversible cytotoxic edema
of the white matter from acute MTX leukoencephalopathy (12). All of them, except patient number 2
whom had completed treatment, had received further doses of
intrathecal or HD MTX subsequently without any recurrence of
neurotoxicity.
 | Table I.Clinical features of 5 patients with
acute methotrexate neurotoxicity and successful outcomes after
rechallenge with MTX. |
Table I.
Clinical features of 5 patients with
acute methotrexate neurotoxicity and successful outcomes after
rechallenge with MTX.
| No. | Age (years) | Sex | Diagnosis | Route of MTX prior to
event | Time to event
(days) | Neurological
symptoms | Duration (days) |
|---|
| 1 | 12 | Male | ALL | HD and IT MTX | 9 | Hemiparesis,
bilateral weakness, dysphasia, confusion, emotionality and
chorea | 1 |
| 2 | 7 | Female | ALL | HD and IT MTX | 8 | Hemiparesis,
confusion, emotionality and chorea | 6 |
| 3 | 6 | Female | ALL | IT MTX only | 4 | Hypotonia in all
limbs and chorea | 7 |
| 4 | 17 | Male | ALL | IT MTX only | Unknown | Nausea, headache,
confusion, right hemiparesis and chorea | <10 |
| 5a | 46 | Female | DLBCL | HD MTX only | 4 | Seizure, confusion
and chorea | 5 |
| Table II.MRI imaging features and successful
outcomes of 5 patients after rechallenge with MTX. |
Table II.
MRI imaging features and successful
outcomes of 5 patients after rechallenge with MTX.
| Author, year | No. | MRI imaging features
at initial presentation | MRI imaging features
on follow-up (duration) | Treatment | Subsequent doses of
MTX given | Recurrence of
neurotoxicity | (Refs.) |
|---|
| Inaba et al,
2008 | 1 | Restricted diffusion
in the bilateral centrum semiovale, corona radiata and internal
capsules | Normal diffusion with
persistent T2 and FLAIR signal increase (7 days) | Aminophylline | HD and IT MTX | No | 9 |
| Inaba et al,
2008 | 2 | Restricted diffusion
in the bilateral basal ganglia, putamina and caudate heads | Increased diffusion
with residual small left periatrial white matter signal on T2 and
FLAIR (5 months) | Aminophylline | Nonea | No | 9 |
|
|
|
|
| Lorazepam,
clonazepam |
|
|
|
|
|
|
|
| Diphenhydramine |
|
|
|
| Necioğlu et
al, 2009 | 3 | No signal
abnormalities | NA | Haloperidol | IT MTX | No | 10 |
| Bota and Dafer,
2009 | 4 | Restricted diffusion
in the bilateral centrum semiovale | Normal diffusion with
persistent T2 and FLAIR signal increase (2 months) | Folinic acid
Dexamethasone | IT MTX | No | 11 |
| NA | 5b | Restricted diffusion
in the bilateral basal ganglia and periventricular white
matter | Normal diffusion with
persistent T2 and FLAIR signal increase (2 months) | Folinic acid
Tetrabenazine | HD and IT MTX | No | NA |
There are differences in the treatments used in
managing acute MTX neurotoxicity, probably because the exact
pathophysiology is still not well understood. The plasma MTX level
does not correlate with the incidence of acute neurotoxicity and
this relationship is not well-established compared to other adverse
effects of MTX such as nephrotoxicity (13). Observations from our patient and case
reports from Hong Kong have illustrated that there are no instances
of delayed elimination of MTX preceding the neurological symptoms
(14). It is widely believed that
MTX can cause direct toxic damage to the CNS, potentially by the
accumulation of adenosine after MTX inhibition on purine synthesis
(15). Methylxanthines have
therefore been used in some cases based on their ability to
displace adenosine from the central receptors (16). We did not employ methylxanthines in
the treatment of our patient but we had continued on folinic acid
for another week. Importantly, the patient went on to receive both
HD MTX and intrathecal MTX successfully.
Prompt recognition of an acute toxic
leukoencephalopathy is important in the management of patients
presenting with neurological symptoms and known recent exposure to
MTX. This would prevent unnecessary investigations and a delay in
the diagnosis of acute MTX neurotoxicity. Diffusion-weighted MRI is
a useful imaging modality to detect early changes of cytotoxic
edema, which are often transient and reversible (17). It is safe to persist with MTX and
that a prior episode of MTX-induced neurotoxicity does not preclude
its future use as MTX remains an effective drug in the management
of CNS lymphoma.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
LC and JC contributed to the conception of the study
and wrote the manuscript. LC, EW, SS, EP, NS, MF, TT, VS, MT, JC
and SL provided clinical assistance and contributed to the
acquisition of clinical data. CC, LT, DC and CO reviewed the slides
and contributed to pathological data acquisition and
interpretation. JK analyzed the images, and interpreted and
acquired the radiological data. All the authors read and approved
the final version of this manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient provided written informed consent for
the publication of any associated data and accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Howard SC, McCormick J, Pui CH, Buddington
RK and Harvey RD: Preventing and managing toxicities of high-dose
methotrexate. Oncologist. 21:1471–1482. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rollins N, Winick N, Bash R and Booth T:
Acute methotrexate neurotoxicity: Findings on diffusion-weighted
imaging and correlation with clinical outcome. AJNR AM J
Neuroradiol. 25:1688–1695. 2004.PubMed/NCBI
|
|
3
|
Vagace JM, de la Maya MD, Caceres-Marzal
C, Gonzalez de Murillo S and Gervasini G: Central nervous system
chemotoxicity during treatment of pediatric acute lymphoblastic
leukemia/lymphoma. Crit Rev Oncol Hematol. 84:274–286. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bhojwani D, Sabin ND, Pei D, Yang JJ, Khan
RB, Panetta JC, Krull KR, Inaba H, Rubnitz JE, Metzger ML, et al:
Methotrexate-induced neurotoxicity and leukoencephalopathy in
childhood acute lymphoblastic leukemia. J Clin Oncol. 32:949–959.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Shah GD, Yahalom J, Correa DD, Lai RK,
Raizer JJ, Schiff D, LaRocca R, Grant B, DeAngelis LM and Abrey LE:
Combined immunochemotherapy with reduced whole-brain radiotherapy
for newly diagnosed primary CNS lymphoma. J Clin Oncology.
25:4730–4735. 2007. View Article : Google Scholar
|
|
6
|
Walker RH: Differential diagnosis of
chorea. Curr Neurol Neurosci Rep. 11:385–395. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
McKinney AM, Kieffer SA, Paylor RT,
SantaCruz KS, Kendi A and Lucato L: Acute toxic
leukoencephalopathy: Potential for reversibility clinically and on
MRI with diffusion-weighted and FLAIR imaging. AJR AM J Roentgenol.
193:192–206. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hegde AN, Mohan S, Lath N and Lim CC:
Differential diagnosis for bilateral abnormalities of the basal
ganglia and thalamus. Radiographics. 31:5–30. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Inaba H, Khan RB, Laningham FH, Crews KR,
Pui CH and Daw NC: Clinical and radiological characteristics of
methotrexate-induced acute encephalopathy in pediatric patients
with cancer. Ann Oncol. 19:178–184. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Necioğlu Orken D, Yldrmak Y, Kenangil G,
Kandraloğlu N, Forta H and Celik M: Intrathecal
methotrexate-induced acute chorea. J Pediatr Hematol Oncol.
31:57–58. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bota DA and Dafer RM: Acute methotrexate
neurotoxicity with choreiform movements and focal neurological
deficits: A case report. South Med J. 102:1071–1074. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Valle DA, Kakehasi FM, Melo RM, Siqueira
CM, Soares TF and Rodrigues KE: Stroke-like encephalopathy
following high-dose intravenous methotrexate in an adolescent with
osteosarcoma: A case report. Rev Bras Hematol Hemoter. 38:364–367.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tsurusawa M, Gosho M, Mori T, Mitsui T,
Sunami S, Kobayashi R, Fukano R, Tanaka F, Fujita N, Inada H, et
al: Statistical analysis of relation between plasma methotrexate
concentration and toxicity in high-dose methotrexate therapy of
childhood nonHodgkin lymphoma. Pediatr Blood Cancer. 62:279–284.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lam DST, Khong PL, Chiang AKS, Ha SY, Lau
YL and Chan GCF: Reversible encephalopathy induced by systemic high
dose methotrexate. HK J Paediatr. 12:287–292. 2007.
|
|
15
|
Bernini JC, Fort DW, Griener JC, Kane BJ,
Chappell WB and Kamen BA: Aminophylline for methotrexate-induced
neurotoxicity. Lancet. 345:544–547. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fernández-Fernández FJ, Ameneiros-Lago E,
Lijó-Carballeda C and Sesma P: Dextromethorphan and methylxanthines
might be useful in the treatment of methotrexate-induced
neurotoxicity. Pediatr Emerg Care. 33:3802017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Salkade PR and Lim TA:
Methotrexate-induced acute toxic leukoencephalopathy. J Cancer Res
Ther. 8:292–296. 2012. View Article : Google Scholar : PubMed/NCBI
|