Introduction
Lung cancer remains the leading cause of
cancer-related mortality amongst men and women in the United
Kingdom (1). The lack of symptoms in
the early disease means that three quarters of lung cancers are
diagnosed at a late stage, often disqualifying patients from
curative treatment (2). Screening
with early diagnosis and treatment has been shown to improve
survival (3).
Metastatic disease is responsible for most cancer
deaths and for this to occur tumour cells must separate from the
primary tumour and circulate in the bloodstream to distant sites
(4). Circulating tumour cells (CTCs)
are cancer cells of epithelial origin that are present in the
peripheral blood samples of cancer patients. They form a
subpopulation of tumour cells which intravasate to allow
haematogenous dissemination to other areas of the body,
contributing to metastatic spread (4). Their use includes early detection of
cancers, monitoring response to treatment and assessing for
reoccurrence (5).
Isolation of CTCs has been attempted by using
physical features such as their larger size and weight, antibody
based platforms, and microfluidic techniques, where spaces and
flows are commensurate with a scale of single cells, allowing CTCs
to be captured (6,7). ScreenCell detection of CTCs relies on
the size of the CTC and is not antibody dependent, removing the
antibody-bias we see with some other techniques.
We have investigated the use of ScreenCell in
operated patients with lung cancer in previous studies (8-12).
In this study we evaluate the value of CTC detection and
association with long term survival.
Our main outcome of interest was whether the
presence of CTCs would impact long term survival. Secondary
outcomes of interest included whether the presence of CTCs would
correlate with the stage of the cancer and if there was a
difference between histological subtype of tumour and the
proportion of patients with CTCs. In addition to evaluate for any
differences in the proportion of CTCs in patients undergoing a
thoracoscopic or open surgical approach.
Patients and methods
A total of 33 patients undergoing surgical treatment
with curative intent for non-small cell lung cancer (NSCLC) were
recruited from August, 2012 to June, 2015 at Harefield Hospital
(Uxbridge, UK). The median age of the patients was 66 years (range,
41-87 years) and 15 (45%) patients were male. Patients had a
confirmed diagnosis of NSCLC either pre-operatively or on an
intra-operative frozen section. Ethical approval was sought prior
(ethical approval no. 10/H0504/9), with consent obtained
pre-operatively. Patients who participated in this research had
complete clinical data. The signed informed consents were obtained
from the patients or the guardians. Surgery was performed under the
care of four thoracic surgeons at a tertiary thoracic centre.
Operations were performed via a thoracotomy or via video assisted
thoracotomy surgery (VATS) approach. One case was performed via a
sternotomy where there were bilateral lung lesions.
Patients were followed-up for a median time period
of 5 years post-operatively. Survival information was obtained by
contacting the patient's General Practitioner in January, 2018.
The detailed technique of CTC detection using the
ScreenCell device is described elsewhere (9). Briefly, three millilitres of blood was
collected from the peripheral vein of patients immediately prior to
surgery in EDTA tubes. Samples were incubated with a lysis and
formaldehyde fixation buffer provided by ScreenCell. Samples were
then filtered through the ScreenCell® device as per the
manufacturer's protocol.
Post-filtration filters were removed and stained
with haematoxylin and eosin (H&E) staining. Stained filters
were then mounted on to slides and viewed by a consultant
pathologist to assess for the presence of CTCs. All patient samples
were processed using the ScreenCell device and scored as being
either negative or positive for CTCs, based on the following
characteristics, large epithelioid cells with, nuclear enlargement
and an increased nuclear to cytoplasmic ratio.
All recruited patients were diagnosed with NSCLC, of
which 21 (64%) patients were diagnosed with adenocarcinoma and 12
(36%) patients with squamous cell carcinoma. The median age of the
patients was 64 years, with an interquartile range (IQR) of 13.7
years. Fifteen (45%) patients were male. Fifteen (45%) patients had
stage I lung cancer, eleven (33%) patients had stage II, 6 (15%)
patients had stage III and 1 (3%) patient had stage IV disease
(T3N2M1a) due to a metastatic pleural deposit at the time of
surgical resection.
Twenty-eight (85%) patients had a lobectomy, 1 (3%)
patient required pneumonectomy, and 4 (12%) patients who were not
fit enough for a lobectomy had a wedge resection. Surgery was
performed thoracoscopically in 7 (21%) patients and with an open
approach in 26 (79%) patients (25 thoracotomies, 1 sternotomy due
to bilateral lesions).
Statistical analysis was calculated on GraphPad
Prism version 5 (GraphPad Software, Inc.), and the survival
proportion was analysed as a Kaplan-Meier plot. Statistical
significance was calculated using a Chi-square test, and a hazard
ratio (HR) was calculated with a 95% confidence interval (CI). The
analysis between lung cancer stage and the proportion of patients
with positive CTCs was performed using Pearson's correlation.
Tumour node metastasis version 7 was used for staging patients.
Analysis between groups was performed using a two-sided Student's
t-test.
Results
CTCs were detected in 26 (79%) patients. At the end
of our follow-up period at a median of 5 years, 20 patients (61%)
were still alive (Table I). In
patients who were positive for CTCs 9 out of 26 patients (35%) had
succumbed to the disease, whereas in patients negative for CTCs 4
out of 7 (57%) patients had succumbed to the disease (P=0.29). Of
the 13 patients who succumbed to the disease 9 (69%) had CTCs
detected. Whereas in the 20 patients who were still alive 17 (85%)
had detected CTCs.
 | Table IMedian survival depending on histology
and CTC status. |
Table I
Median survival depending on histology
and CTC status.
| | | CTC status | Median survival
(months) |
|---|
| Histology | Total | Detected | Not detected | Total | CTCs detected | CTCs not
detected |
|---|
| Adenocarcinoma | 21 (64%) | 17 (81%) | 4 (19%) | 38 | 38 | 31 |
| SqCC | 12 (36%) | 9 (75%) | 3 (25%) | 53 | 60 | 34 |
| Total | 33 | 26 (79%) | 7 (21%) | 39 | 47a | 34a |
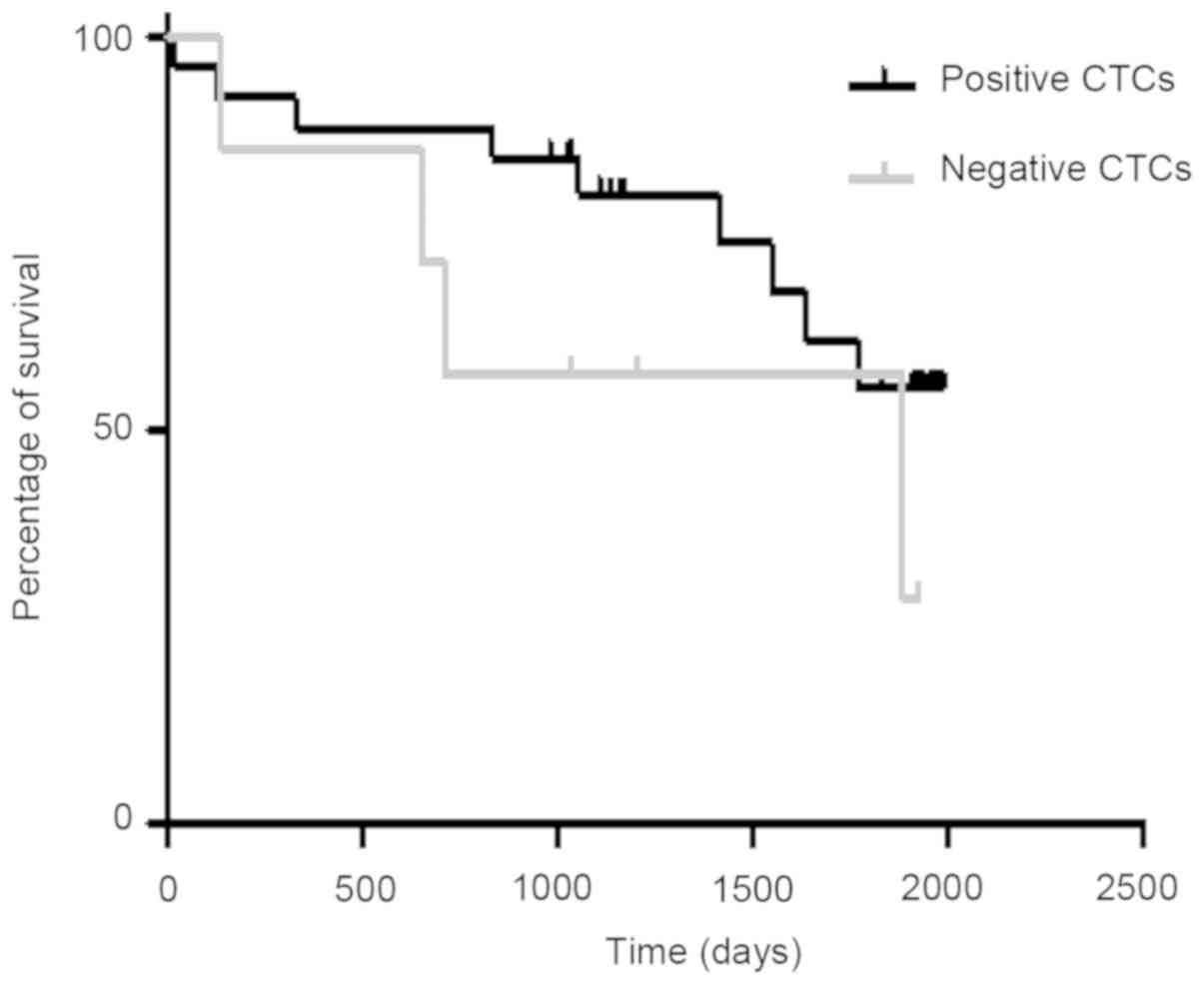
Overall survival was analysed using a Kaplan Meier
plot (Fig. 1) of patients positive
and negative for CTCs. It showed no relationship between positive
CTCs being associated with poorer survival, Chi-squared 1.47,
P=0.23, HR=0.42 (95% CI: 0.1-1.7). Median survival in patients with
CTCs was 46.5 months whereas it was only 34.1 months in patients
without CTCs.
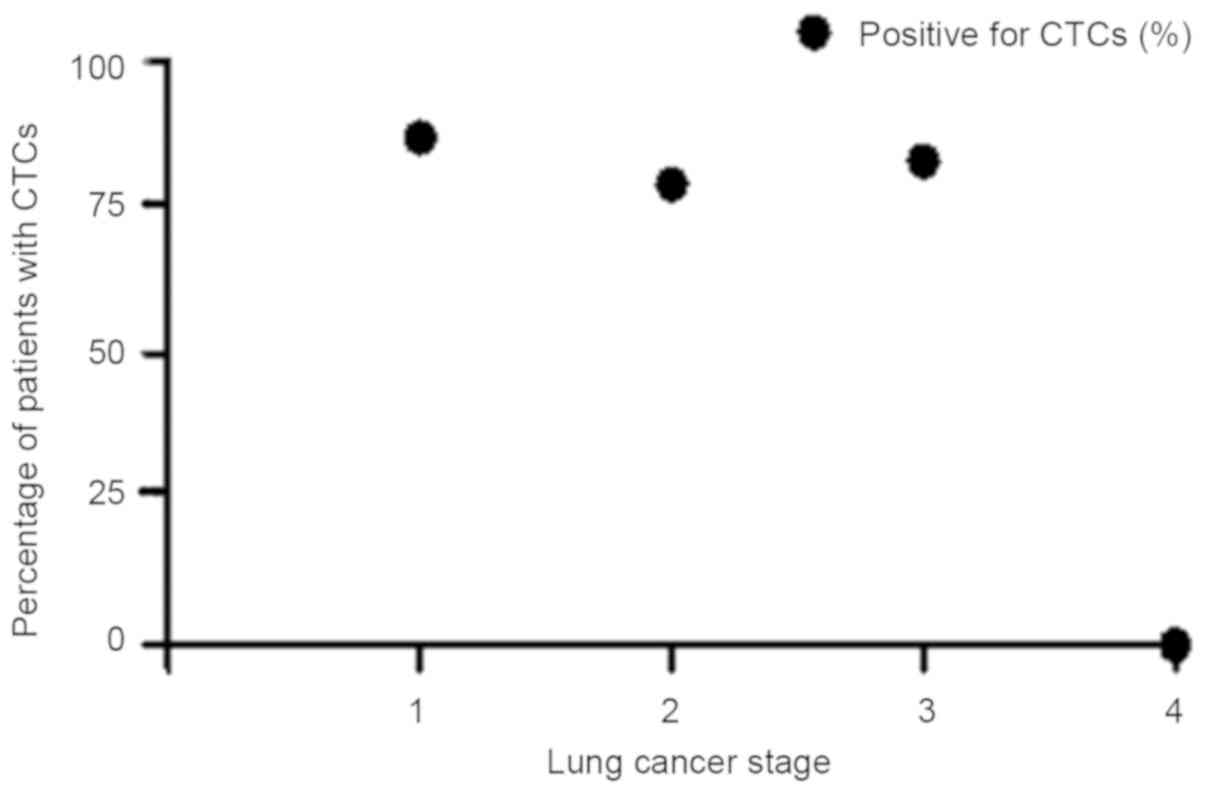
There was no direct correlation between the stage
and detection of CTCs (Table II). A
Pearson's analysis (Fig. 2) between
proportion of patients with positive CTCs status and lung cancer
stage showed negative correlation, Pearson's r=-0.80, P=0.20.
| Table IISurvival depending on lung cancer
stage and CTC status. |
Table II
Survival depending on lung cancer
stage and CTC status.
| | | Total | CTC status |
|---|
| Stage | Total (%) | Alive | Deceased | Detected | Not detected |
|---|
| 1 | 15 (45.4%) | 9 (60%) | 6 (40%) | 13 (87%) | 2 (13%) |
| 2 | 11 (33.3%) | 8 (73%) | 3 (27%) | 8 (73%) | 3 (27%) |
| 3 | 6 (18.1%) | 3 (50%) | 3 (50%) | 5 (83%) | 1 (17%) |
| 4 | 1 (3.3%) | 0 (0%) | 1 (100%) | 0 (0%) | 1 (100%) |
| Total | 33 | 20 (61%) | 13 (39%) | 26 (79%) | 7 (21%) |
Of the 21 patients with adenocarcinoma 17 (81%)
patients had positive CTCs whereas of the 12 patients with squamous
cell carcinoma 9 (75%) patients had positive CTCs (P=0.70)
(Table I).
A total of 6 of the 7 (86%) patients that had their
operation performed thoracoscopically were positive for CTCs
whereas 20 of the 26 (77%) patients that had an open operation were
positive for CTCs (P=0.63; Table
III). Survival in the patients undergoing a thoracoscopic
approach was 51 vs. 38 months in the open group (P=0.43).
| Table IIIMedian survival based on operative
approach and CTC status. |
Table III
Median survival based on operative
approach and CTC status.
| | | CTC detected | CTC not detected |
|---|
| Surgery | Total | Total (%) | Survival
(months) | Total (%) | Survival
(months) |
|---|
| VATS | 7 | 6(86)a | 54b | 1(14) | 23b |
| Open | 26 | 20(77)a | 38b | 6(23) | 37b |
Survival was better, although not significantly, in
women positive for CTCs compared with men (58 vs. 38 months,
respectively), P=0.43. In women negative for CTCs survival was 37
months compared to 21 months in men negative for CTCs (P=0.61;
Table IV).
| Table IVMedian survival based on gender and
CTC status. |
Table IV
Median survival based on gender and
CTC status.
| | | CTC detected | CTC not detected |
|---|
| Sex | Total | Total (%) | Survival
(months) | Total (%) | Survival
(months) |
|---|
| Female | 18 | 14(43) | 58a | 4(12) | 37a |
| Male | 15 | 12(36) | 38b | 3(9) | 21b |
In the subgroup of patients who underwent a wedge
resection 3 of the 4 patients (75%) were positive for CTCs, whereas
in the group undergoing lobectomy or pneumonectomy 23 out of 29
patients (79%) were positive for CTCs (P=0.85).
Discussion
Previously we demonstrated the ability of ScreenCell
in detecting CTCs in patients with lung cancer (8). In this study we sought to evaluate the
impact of positive CTCs on long term follow-up. There was no effect
of the presence of CTCs on median survival, in fact their presence
was actually surprisingly associated with longer median survival
compared to those patients negative for CTCs, although not
significantly. This was also the case when we analysed the results
with shorter follow up and fewer patients (8).
It is known that different types of lung cancer
metastasize via difference means and this can reflect their
potential to spread. Small cell lung cancer and undifferentiated
NSCLC spread via single cell or small cell cluster movement whereas
in adenocarcinoma and squamous cell carcinoma spread results from
movement of large clusters of organised cells (13). ScreenCell looks for individual CTCs.
Given that all patients in our cohort had either adenocarcinoma or
squamous cell carcinoma it may be that the presence of isolated
CTCs is not clinically relevant to the metastatic potential as
these tumour will not metastasize until organised clusters of cells
are formed. In our cohort there was no difference in the proportion
of CTCs between adenocarcinomas and squamous cell carcinomas
however this likely reflects that they both metastasize in a
similar way (13). The improved
prognosis (although not significant) in patients with CTCs may
reflect the fact that detection of single CTCs primes the immune
system to respond to organised clusters of cells.
Our data did not show a significant association
between the proportion of patients with CTCs and lung cancer stage
(Fig. 2). However it is interesting
to note that even in patients with stage I lung cancer 87% of
patients had CTCs found in a sample of peripheral blood. Thus even
at this early stage lung cancers are producing CTCs which can be
detected in a peripheral blood sample. This highlights the
potential importance that the detection of CTCs could have as a
screening test for early stage lung cancer.
There is evidence to support that patients
undergoing a VATS lobectomy for early stage lung cancer have
improved survival compared to those patients undergoing an open
operation. One potential reason for this is that there is reduced
manipulation of the lung and the tumour with a VATS approach
compared to open surgery, which reduces the number of CTCs shed
during surgery (14,15). However we were unable to detect any
difference in the number of CTCs between VATS and open surgery to
support this theory although the numbers in our VATS group were
small.
Limitations of our study included the small sample
size of 33 patients and the heterogeneity of the cohort with
patients with different lung cancer stage. The study was designed
as a pilot study to assess whether a link exists between ScreenCell
detected CTCs and prognosis. Although there was heterogeneity in
the cohort it was designed to reflect clinical practice of patients
operated on for lung cancer.
Our result show that the presence of CTCs detected
with ScreenCell does not have an effect on prognosis in patients
with operated NSCLC. We believe that this may reflect the fact the
ScreenCell detects single cells which may not be relevant to the
metastatic potential of lung adenocarcinoma and squamous cell
carcinoma.
There was no relationship between lung cancer stage
and the proportion of patients with CTCs. It is interesting that
even in stage I lung cancers more than 80% of patients were found
to have detectable CTCs which is encouraging in supporting this
technology to aid early lung cancer diagnosis.
Acknowledgements
Not applicable.
Funding
The present study was supported by funding was from
The Harefield Charitable Cryotherapy Trust Funds.
Availability of data and materials
All data generated or analysed during this study are
included in this published article.
Authors' contributions
JB wrote the manuscript, analysed the data and
performed the statistical tests. DC collected and analysed the data
and helped with writing the manuscript. AR analysed the samples for
the presence of circulating tumour cells, EK was involved in the
designing the study and writing the manuscript. VA designed the
study and wrote the manuscript.
Ethics approval and consent to
participate
Ethical approval was sought prior (ethical approval
no. 10/H0504/9), with consent obtained pre-operatively. Patients
who participated in this research had complete clinical data. The
signed informed consents were obtained from the patients or the
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lung cancer statistics. Cancer research
UK, Oxford, 2018. https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/lung-cancer.
Accessed April 4, 2018.
|
|
2
|
Bannister N and Broggio J: Survival for
people diagnosed by cancer type, split by stage at diagnosis. Data
based on people diagnosed in England in. 2012, 2013 and 2014.
Produced in collaboration with Public Health England (PHE). In:
Cancer survival by stage at diagnosis for England (experimental
statistics): Adults diagnosed 2012, 2013 and 2014 and followed up
to 2015. Office for National Statistics, Newport, pp1-30, 2016.
|
|
3
|
National Lung Screening Trial Research
Team. Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, Fagerstrom
RM, Gareen IF, Gatsonis C, Marcus PM and Sicks JD: Reduced lung
cancer mortality with low dose computed tomographic screening. N
Engl J Med. 365:395–409. 2011.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Pantel K, Brakenhoff RH and Brandt B:
Detection, clinical relevance and specific biological properties of
disseminating tumour cells. Nat Rev Cancer. 8:329–340.
2008.PubMed/NCBI View
Article : Google Scholar
|
|
5
|
Zhang Z, Ramnath N and Nagrath S: Current
Status of CTCs as Liquid Biopsy in Lung Cancer and Future
Directions. Front Oncol. 5(209)2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Hou HW, Warkiani ME, Khoo BL, Li ZR, Soo
RA, Tan DS Lim WT, Han J, Bhagat AA and Lim CT: Isolation and
retrieval of circulating tumor cells using centrifugal forces. Sci
Rep. 3(1259)2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Dent BM, Ogle LF, O'Donnell RL, Hayes N,
Malik U, Curtin NJ, Boddy AV, Plummer ER, Edmondson RJ, Reeves HL,
et al: High-resolution imaging for the detection and
characterisation of circulating tumour cells from patients with
oesophageal, hepatocellular, thyroid and ovarian cancers. Int J
Cancer. 138:206–216. 2016.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Chudasama D, Barr J, Beeson J, Beddow E,
McGonigle N, Rice A, Nicholson A and Anikin V: Detection of
Circulating Tumour Cells and Survival of Patients with Non-small
Cell Lung Cancer. Anticancer Res. 37:169–173. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Chudasama D, Rice A, Anikin V, Soppa G and
Dalal P: Circulating Tumour Cells in Patients with Malignant Lung
Tumors Undergoing Radio-frequency Ablation. Anticancer Res.
35:2823–2826. 2015.PubMed/NCBI
|
|
10
|
Chudasama D, Burnside N, Beeson J,
Karteris E, Rice A and Anikin V: Perioperative detection of
circulating tumour cells in patients with lung cancer. Oncol Lett.
14:1281–1286. 2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Chudasama D, Rice A, Soppa G and Anikin V:
Circulating tumour cells in patients with lung cancer undergoing
endobronchial cryotherapy. Cryobiology. 71:161–163. 2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Freidin MB, Tay A, Freydina DV, Chudasama
D, Nicholson AG, Rice A, Anikin V and Lim E: An assessment of
diagnostic performance of a filter-based antibody-independent
peripheral blood circulating tumour cell capture paired with
cytomorphologic criteria for the diagnosis of cancer. Lung Cancer.
85:182–185. 2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Popper HH: Progression and metastasis of
lung cancer. Cancer Metastasis Rev. 35:75–91. 2016.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Chen FF, Zhang D, Wang YL and Xiong B:
Video-assisted thoracoscopic surgery lobectomy versus open
lobectomy in patients with clinical stage Ⅰ non-small cell lung
cancer: A meta-analysis. Eur J Surg Oncol. 39:957–963.
2013.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Cai YX, Fu XN, Xu QZ, Sun W and Zhang N:
Thoracoscopic lobectomy versus open lobectomy in stage I non-small
cell lung cancer: A meta-analysis. PLoS One.
8(e82366)2013.PubMed/NCBI View Article : Google Scholar
|