Introduction
In recent years, the frequency of esophagogastric
junction cancer (EGJ) has been rapidly increasing in Europe and the
United States. According to Comprehensive registry of esophageal
cancer in japan 2010, the incidence of EGJ cancer is also
increasing (1). The EGJ cancers are
classified by Rudiger Siewert et al (2) and different types require different
treatment strategies, therefore there is no established consensus
on the optimal treatment.
In Europe neoadjuvant-chemoradiotherapy (neo-CRT) is
the standard treatment for EGJ cancer based on the CROSS trial
(3), but it is concerned that the
effect of CRT is lower in adenocarcinoma than in squamous cell
carcinoma.
Radical esophagectomy is considered as the standard
treatment for patients with esophagogastric junction (EGJ) cancer
with extensive invasion of the esophagus and/or suspected
metastasis to the mediastinal area. With recent advances in
surgical technique and perioperative management, the rate of
perioperative mortality for radical esophagectomy has been reported
to be <5% (4). The latest study
which based on the Japanese national clinical database reported
that the overall 30-day mortality rate for open esophagectomy was
0.9%, and total surgery related mortality rate was 2.4% (5). Furthermore, it is suggested that
minimally invasive esophagectomy (MIE) may be performed and may
contribute to reduction of complications. However, complications
during anastomosis which causes mediastinitis and empyema thoracis
can led to septic shock may be severe and, thus, caution is
required. Specifically, necrosis of the esophageal anastmosis
reconstruction conduit after esophagectomy is a complication that
carries a risk of mortality of up to 90% (6). The reconstructed conduit necrosis is
rare and is only reported in <2% of primary resections with
reconstruction (6). Herein, we
describe the case of a patient with necrosis in the residual
esophagus, rather than in the reconstructed conduit. We include our
treatment and the clinical outcome.
Case report
A 66-year-old man presented to Asai Hospital (Chiba,
Japan) with epigastric discomfort and symptoms of gastrointestinal
obstruction. Gastrointestinal endoscopy revealed a tumor at the
EGJ, which was confirmed as an adenocarcinoma on biopsy.
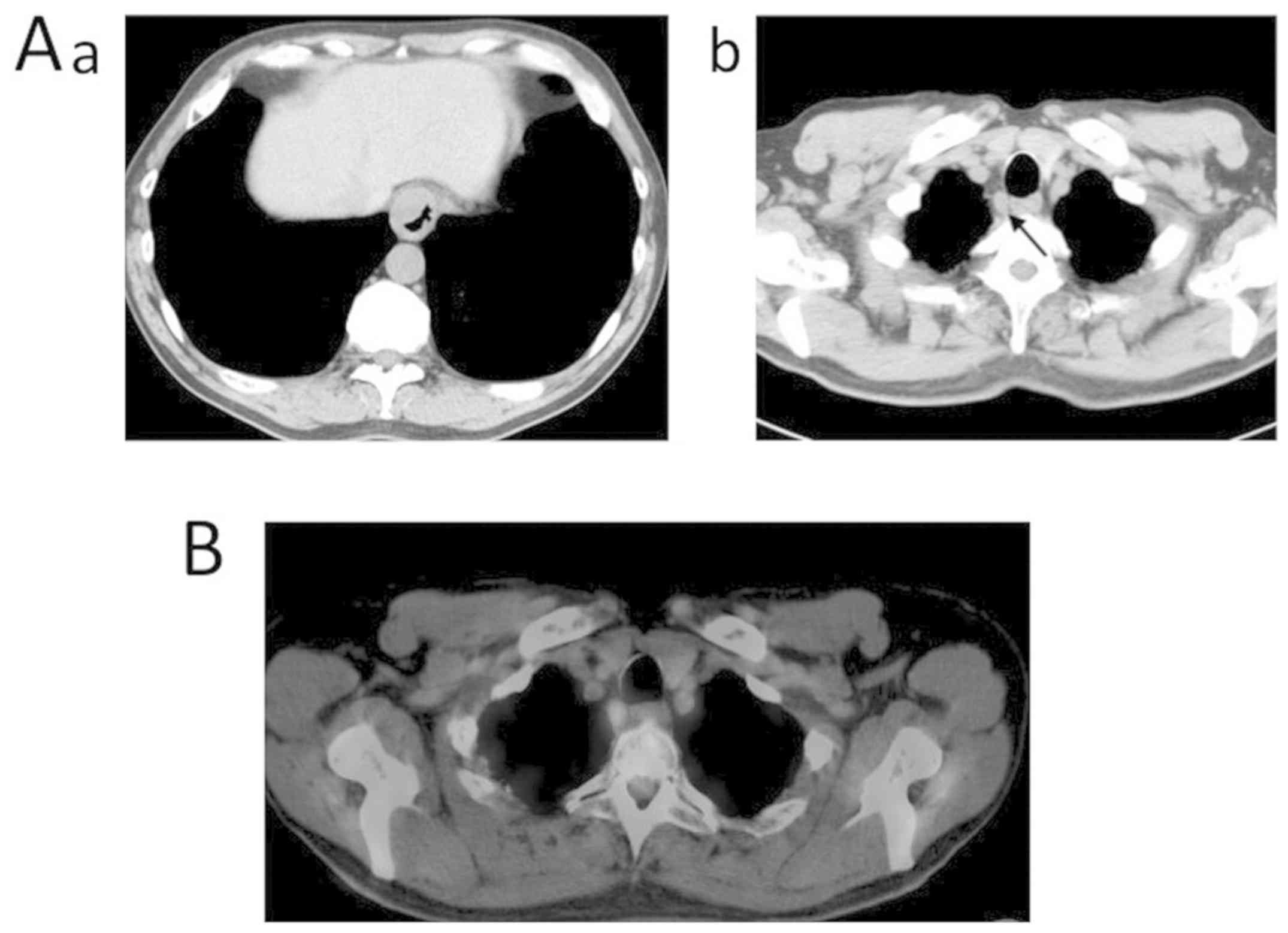
Contrast-enhanced computed tomography (CT) was performed at our
institution, which revealed a tumor extending from the lower
thoracic esophagus to the EGJ, with associated swelling of the
upper mediastinal lymph nodes. Based on the criteria of the
International Union against Cancer Committee (UICC, 8th Edition),
the clinical staging was as follows: 101R, 107, and 106 pre. There
was little suspicion of lymph node metastasis owing to the small
amount of accumulation observed on positron-emission tomography
(PET) CT (PET-CT) imaging (Fig. 1A
and B). Laboratory tests revealed
abnormal values of creatinine level (1.14 mg/dl; reference range
0.65-1.07), with all other levels being within normal range. Tumor
marker levels were as follows: Carcinoembryonic antigen, 4.7 ng/dl
(upper reference limit, 5.0 ng/dl); carbohydrate antigen 19-9, 6.9
IU/ml (upper reference limit, 37.0 IU/ml); and cancer antigen 125,
14.5 IU/ml (upper reference limit, 35.0 IU/ml). Based on these
findings, we made a clinical diagnosis of EGJ cancer, with a UICC
8th classification of cT3N1M0 c-stage-Ⅲ.
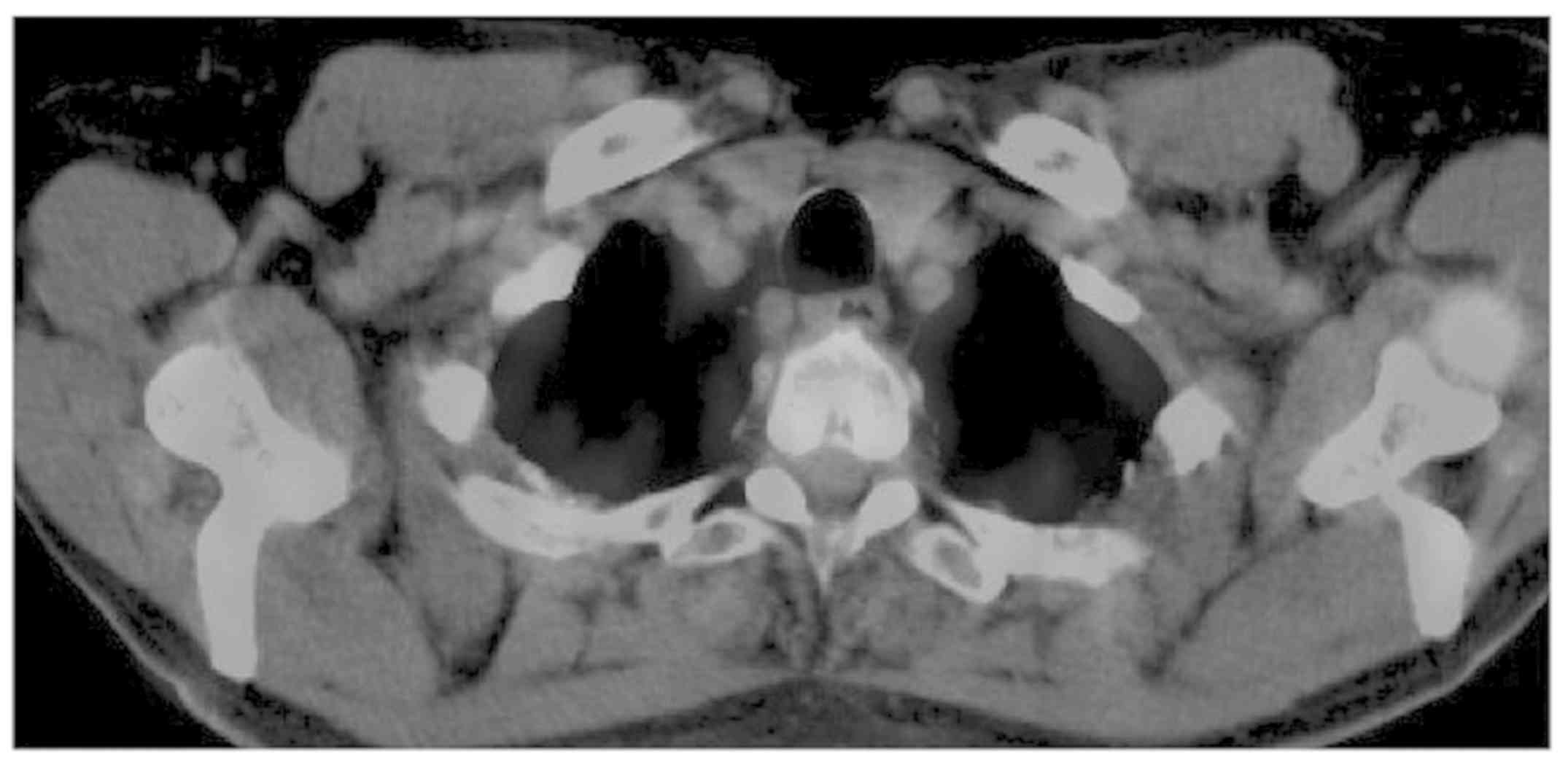
In accordance with this diagnosis, preoperative S-1
neoadjuvant chemotherapy (NAC) was implemented (oral
fluoropyrimidine, containing tegafur, gimeracil, and oteracil
potassium) in combination with oxaliplatin. After 3 courses of NAC,
the size of the tumor was reduced, but without a clinical change in
lymphadenopathy, with still little accumulation of PET-CT scans
(Fig. 2). Based on these findings,
we proceeded with esophagectomy, with three-field lymph node
dissection and gastric tube reconstruction, via an intrathoracic
route. Surgery was performed 4 weeks after the chemotherapy.
We first proceeded with cervical surgery. The right
reflex nerve was identified during right cervical lymph node
dissection (101R), with observation of an enlarged lymph node.
Accordingly, we proceeded with bilateral dissection of the lymph
nodes dissection, but with no observable evidence of
lymphadenopathy on the left side. The abdominal component of the
surgery was performed as per usual methods, with the stomach
used to reconstruct the esophageal conduit. Following upper, middle
and lower mediastinal lymphadenectomy, we proceeded with
reconstruction of the gastric tube, with dissection of the right
bronchial artery and azygos vein. The surgical time was 318 min,
with a volume of blood loss of 210 ml.
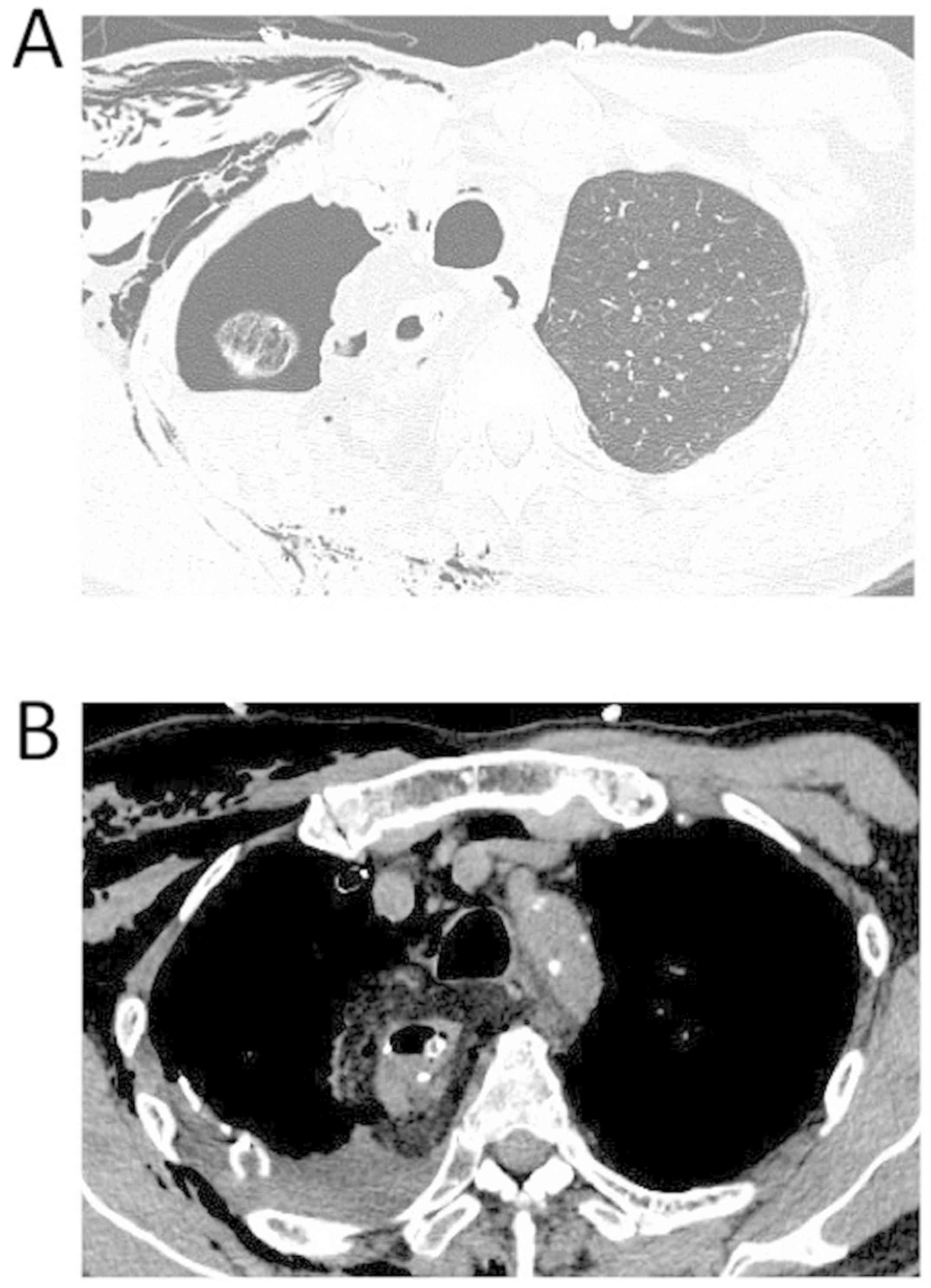
An idiopathic pneumothorax developed on
postoperative day (POD) 2, with a brown-green drainage from the
chest tube. The pneumothorax was confirmed on CT imaging, but with
no evidence of abnormality around the anastomosis. As the
pneumothorax did not improve with conservative treatment, with
persistent green drainage in the thoracic tube, we proceeded with
surgical management of the pneumothorax and observation of the
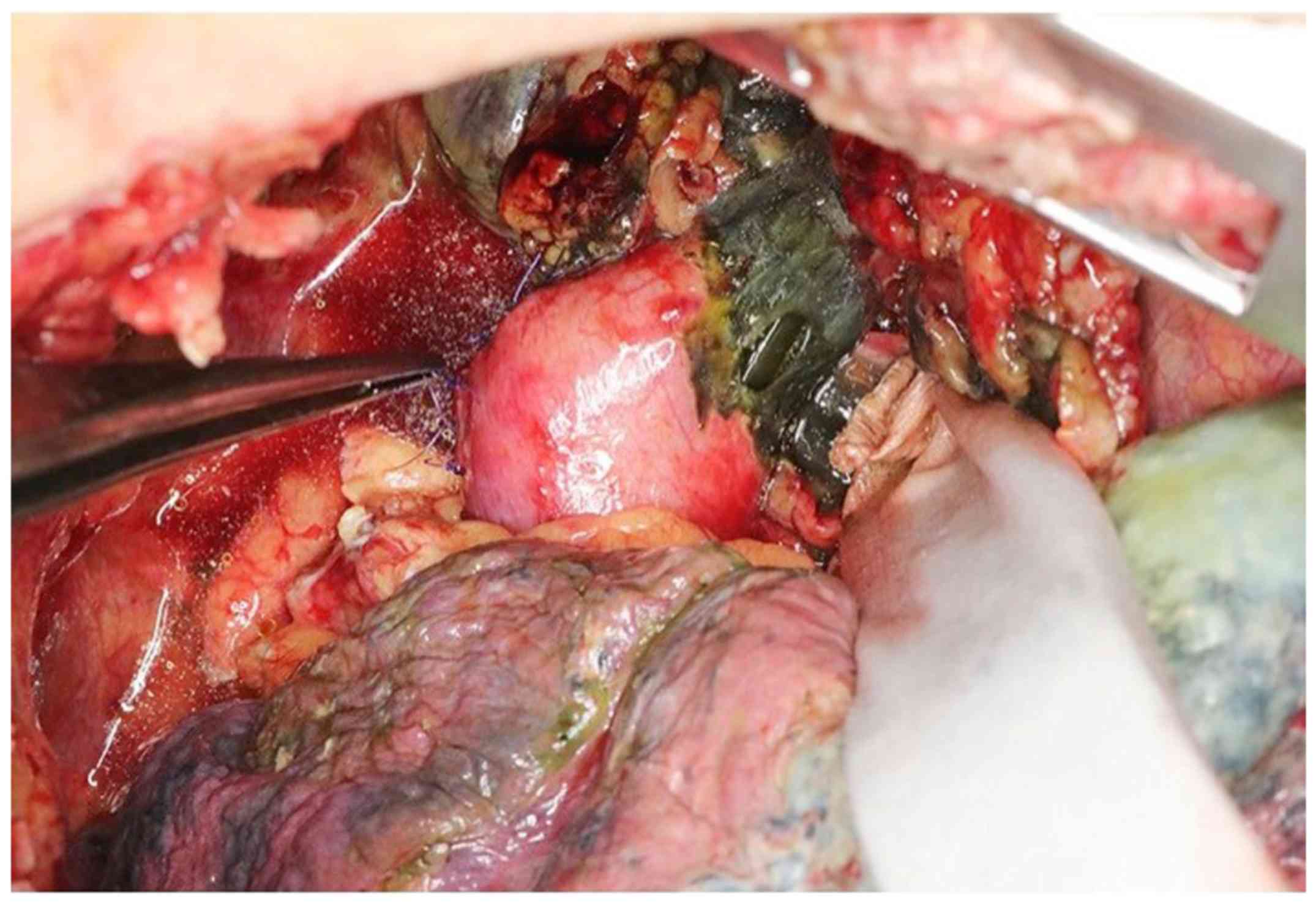
anastomosis (Fig. 3). On repeat
thoracotomy, the continued presence of brown-green pleural fluid
was confirmed, and necrosis of the esophagus was observed, after
release of the belaq attached to the anastomosis. The area of
necrosis was localized 4 cm on the oral side of the anastomosis,
with necrotic damage being more prominent on the right than left
side, but with no signs of necrosis in the gastric tube (Fig. 4).
We proceeded with excision of the residual necrotic
esophagus, followed with reconstruction of an external fistula on
left side of neck. The residual gastric tube was positioned under
the skin, through an antethoracic route. The pneumothorax was
detected in the S1 area and closed using staples.
Post-surgery, the patient did not develop further
complications and was discharged on POD 17 after the second
surgery. On POD 38 (after the second surgery), we proceeded with
reconstruction to connect the residual esophagus and gastric tube,
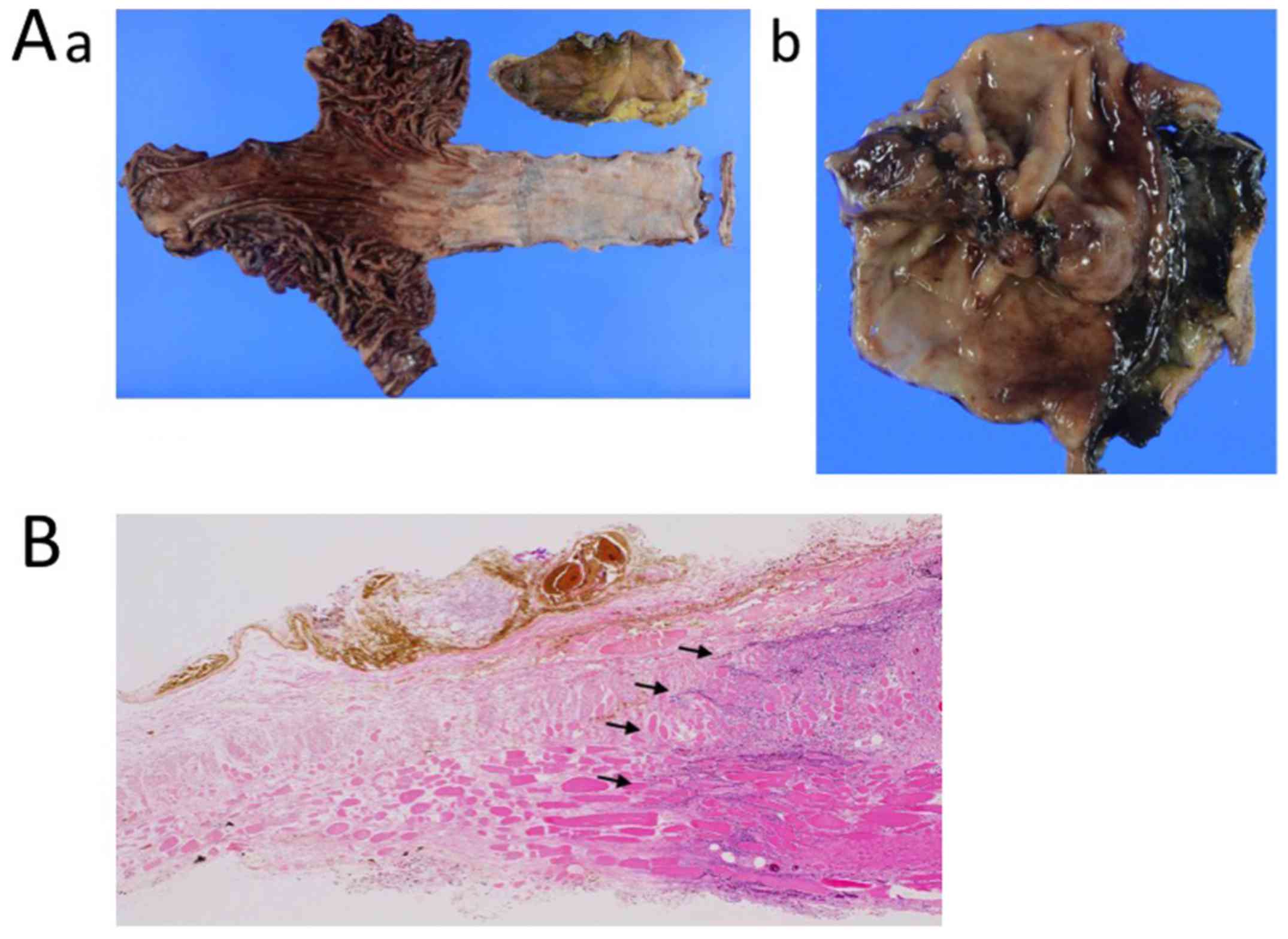
through the jejunum. Pathological findings of the resected specimen
confirmed residual adenocarcinoma at the esophagogastric junction,
with the following tumor components identified: Tub1 >tub2 and
>por2. The resected margin was negative. The final pathological
diagnosis was ypT1aN0(0/66)M0, ypStageIA (UICC 8th). Owing to the
impairment in the local circulation, necrotizing tissue was
observed in the entire layer of the residual esophagus, but not in
the layer of the conduit (Fig. 5A
and B). At 7 months post-discharge,
the patient was alive, with no evidence of cancer recurrence.
Discussion
It is very rare for residual esophageal necrosis to
occur after esophagectomy. Although conduit necrosis after
esophagectomy has previously been reported, we identified only one
report regarding necrosis of the esophagus (7). Blood flow to the conduit after
esophagectomy is primarily dependent on the mucosal capillary
network (8). The nature of this
capillary network, however, has not been clearly determined.
Takemura et al (7) argued
that the capillary network developed in the submucosal layer would
sustain the residual esophagus, despite inclusion of the main
artery along with lymph node dissection.
The following factors can contribute to necrosis of
the esophageal conduit (6,9): Diabetes, hypertension, and peripheral
vascular disease. However, smoking, preoperative chemotherapy, and
bodyweight were not identified as contributing factors to conduit
necrosis (9). The mortality rate
associated with necrosis of the esophageal conduit can be as high
as 90% (6). We note that the patient
in the case study reported by Takemura et al (7), had a history of myocardial infarction
and vascular disease-factors that were not present in our case. The
factors that cause necrosis remain unknown in this patient.
Acute ischemic necrosis of the esophagus is
possible, as occurs in bowel disease, although the etiology of this
acute necrosis is different in the esophagus and bowel. Necrosis of
the esophagus (also known as black esophagus) is very rare,
with a prevalence of 0.2% in autopsy data (10). The etiology of black esophagus is
associated with risk factors for atherosclerosis (such as
hypertension, diabetes, and ageing) or diabetic ketoacidosis, as
well as multiple organ dysfunction and sepsis (11). However, none of these factors were
identified in our case. As such, it is likely that performance of
the surgical anastomosis itself was the cause of esophageal
necrosis in our case.
The enlarged right lymph node (101R) was strongly
adherent to the wall of the esophagus. Therefore, the possibility
of direct invasion of the cancer into the esophageal wall could not
be ruled out. During dissection, the muscle layer of the esophagus
was excised. Once the 101 lymph nodes were dissected, the cervical
esophagus was excised from the surrounding area and released, which
differed from traditional cervical dissection and esophagectomy. We
do note that this caused a disruption of the local blood flow to
the right side of the esophageal wall. Takemura et al
(7) reported that the length of the
residual esophagus might be one of the causes of necrosis, but the
length of residual esophagus in our case was normal. Although it
remains unclear what caused necrosis of the residual esophagus in
our case, it is possible that the wide anastomosis, which extended
into the cervical area, might be an important factor to
consider.
Residual esophageal necrosis after esophagectomy is
very rare and the possible causative factors remain to be fully
clarified. Based on our experience, extensive dissection of the
cervical esophagus area might be a contributing factor, due to a
deterioration of the local blood flow.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
ST and IH designed the study and wrote the initial
draft of the manuscript. IH, NT, AI, HS, TT, HG, YN and MO
contributed to design and assisted in the preparation of the
manuscript. All other authors have contributed to data collection
and interpretation, and critically reviewed the manuscript. All
authors approved the final version of the manuscript, and agree to
be accountable for all aspects of the work in ensuring that
questions related to the accuracy or integrity of any part of the
work are appropriately investigated and resolved.
Ethics approval and consent to
participate
This study was approved by the Institutional Ethics
Review Board of the Chiba Cancer Center (H29-262) (Chiba,
Japan).
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and any accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Tachimori Y, Ozawa S, Numasaki H, Ishihara
R, Matubara H, Muro K, Oyama T, Toh Y, Udagawa H, Uno T, et al:
Comprehensive registry of esophageal cancer in Japan 2010.
Esophagus. 14:189–214. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Rudiger Siewert J, Feith M, Werner M and
Stein HJ: Adenocarinoma of the esophagogastric junction: Results of
surgical therapy based on anatomical/topographic classification in
1,002 consecutive patients. Ann Surg. 232:353–3361. 2000.PubMed/NCBI View Article : Google Scholar
|
|
3
|
van Hagen P, Hulshof MC, van Lanschot JJ,
Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, Richel DJ,
Nieuwenhuijzen GA, Hospers GA, Bonenkamp JJ, et al: Preoperative
chemoradiotherapy for esophageal or junctional cancer. N Engl J
Med. 366:2074–2084. 2012.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Lerut T, Coosemans W, Decker G, De Leyn P,
Nafteux P and Van Raemdonck D: Anastomotic complications after
esophagectomy. Dig Surg. 19:92–98. 2002.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Yoshida N, Yamamoto H, Baba H, Miyata H,
Watanabe M, Toh Y, Matubara H, Kakeji Y and Seto Y: Can minimally
invasive esophagectomy replace open esophagectomy for esophageal
cancer? Latest analysis of 24,233 esophagectomies from the Japanese
national clinical database. Ann Surg, 2019 [Epub ahead of
print].
|
|
6
|
Dickinson KJ and Blackmon SH: Management
of conduit necrosis following esophagectomy. Thorac Surg.
25:461–470. 2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Takemura M, Fujiwara Y, Moriura K and Hori
T: A case of residual esophageal necrosis after lower esophagectomy
for early esophageal cancer. J Jap College Surgeons (Nihon Gekakei
Rengo Gakkaishi). 36:612–616. 2011. View Article : Google Scholar
|
|
8
|
Liebermann-Meffert DM, Meier R and Siewert
JR: Vascular anatomy of the gastric tube used for esophageal
reconstruction. Ann Thorac Surg. 54:1110–1115. 1992.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Urschel JD: Esophagogastrostomy
anastomotic leaks complicating esophagectomy: A review. Am J Surg.
169:634–640. 1995.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Gurvits GE: Black esophagus: Acute
esophageal necrosis syndrome. World J Gastroenterol. 16:3219–3225.
2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Gurvitis GE, Shapsis A, Lau N, Gualtieri N
and Robilotti JG: Acute esophageal necrosis: A rare syndrome. J
Gastroenterol. 42:29–38. 2007.PubMed/NCBI View Article : Google Scholar
|