Introduction
Miliary lung metastases are a rare form of
metastasis, accounting for 1-2% of cases of non-small-cell lung
carcinoma (NSCLC). Miliary metastases have been reported to be more
commonly found in patients with NSCLCs with an epidermal growth
factor receptor (EGFR) mutation (1,2).
However, there is only one case report on miliary lung metastases
from NSCLC with ROS1 rearrangement (3). We report such a case in a patient with
ROS1-rearranged lung adenocarcinoma.
Case report
A 50-year-old woman who had never smoked underwent
right middle lobectomy for stage IIIA lung micropapillary
adenocarcinoma in June 2017. She refused adjuvant chemotherapeutic
treatment. In February 2018, the follow-up computed tomography (CT)
did not reveal any evidence of recurrence. The patient discontinued
hospital visit on her own judgment. She presented to Kanagawa
Cardiovascular and Respiratory Center (Yokohama, Japan) in November
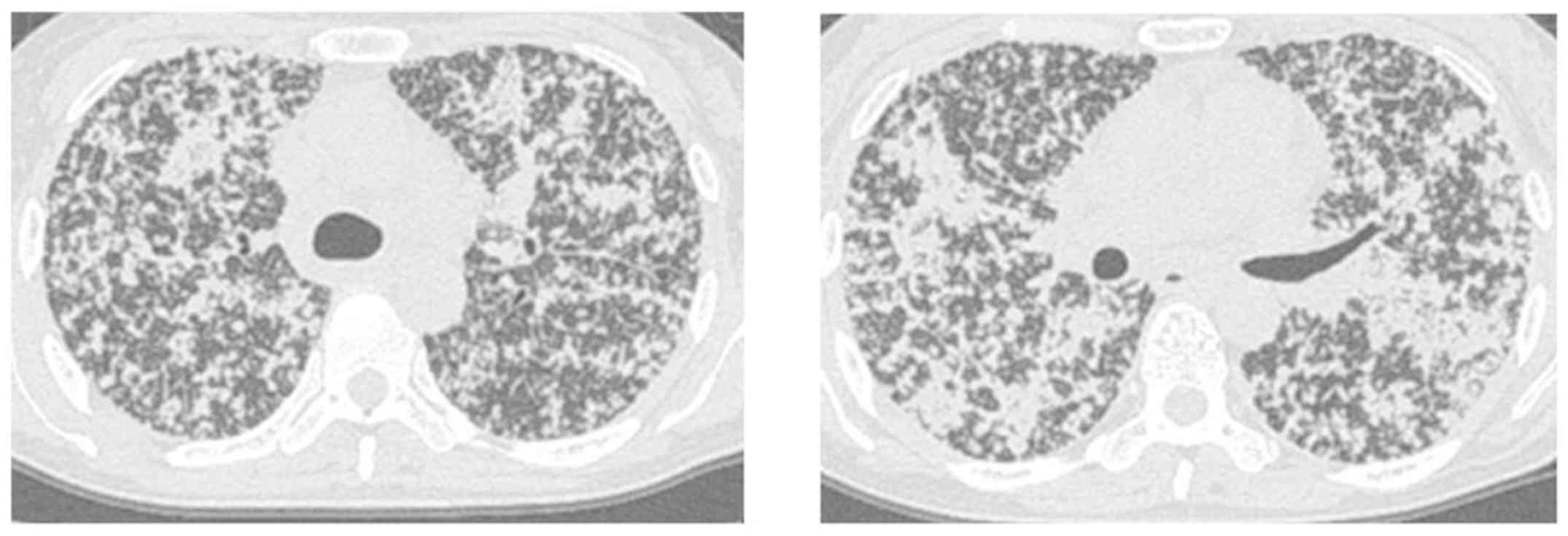
2018 complaining of a 1-month history of cough and dyspnea. She had
severe hypoxia with a pulse oximetry reading of 85% on room air;
thus, oxygen therapy at 5 l/min was started. Chest CT showed
numerous tiny, randomly distributed nodules throughout both lungs,
bilateral patchy consolidation, mediastinal lymphadenopathy, and
intralobular septal thickening (Fig.
1). No metastases were observed in other organs. Laboratory
examinations revealed carcinoembryonic antigen levels to be 84.6
ng/ml (normal, <5.0 ng/ml), KL-6 level to be 3,731 U/ml (normal,
<500 U/ml), and lactase dehydrogenase (LDH) level to be 1,859
U/l (normal, <222 U/l). Based on these results, a diagnosis of
recurrent lung cancer with miliary lung metastases and
lymphangiosis carcinomatosa was made.
Molecular analysis of the surgical specimens
revealed no EGFR mutation or anaplastic lymphoma kinase (ALK)
rearrangement, but there was ROS1 rearrangement as determined using
reverse transcription polymerase chain reaction using primer
sequences according to the manufacturer's instructions of the ROS1
fusion gene detection kit (Amoy Diagnostics Co., Ltd.). Treatment
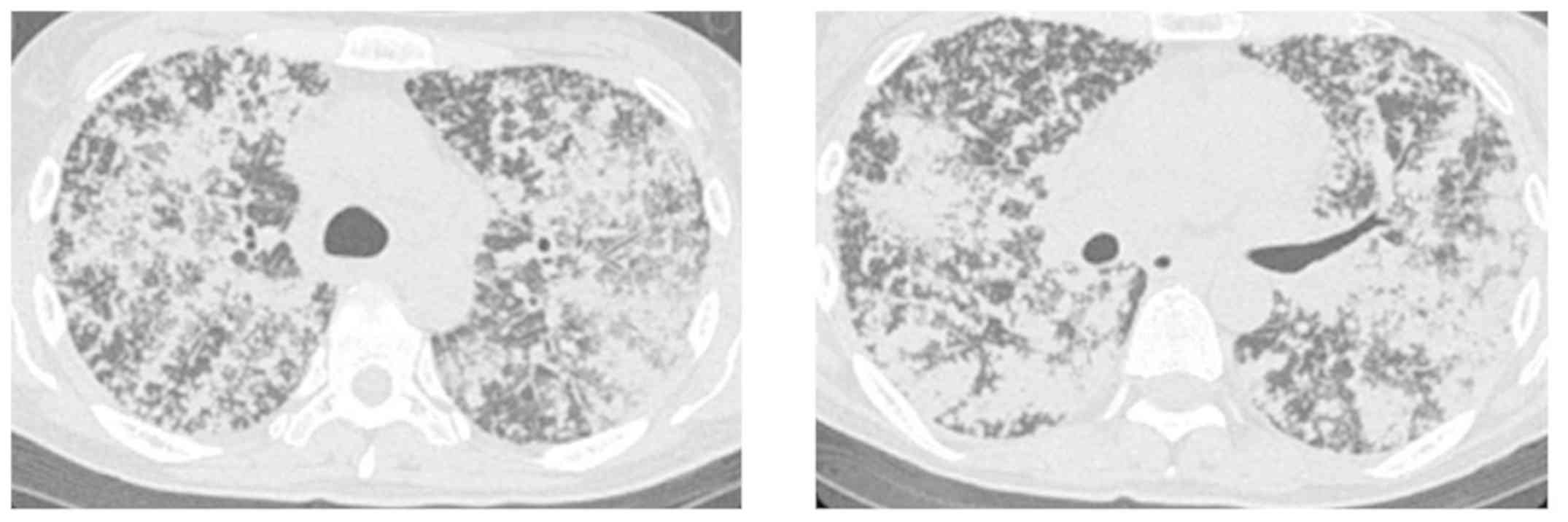
with crizotinib (200 mg/day orally) was administered. However,
after 5 days of treatment, the patient's respiratory condition
rapidly worsened, requiring nasal high-flow oxygen with a fraction
of inspired oxygen of 90%. Chest CT revealed an increase in the
number of miliary nodules and worsening of consolidation (Fig. 2). The LDH level increased to 4503
U/l. However, we could not determine whether the aggravation of her
respiratory condition was due to drug-induced pneumonitis or
disease progression because her respiratory condition rapidly
worsened and could not be assessed by biopsy due to high risk of
further deterioration. Crizotinib treatment was discontinued and
pulse steroids were administered. However, the patient's condition
failed to improve, and her performance status score fell to 2.
Therefore, she was started on a therapy with cisplatin, pemetrexed,
and bevacizumab and closely observed.
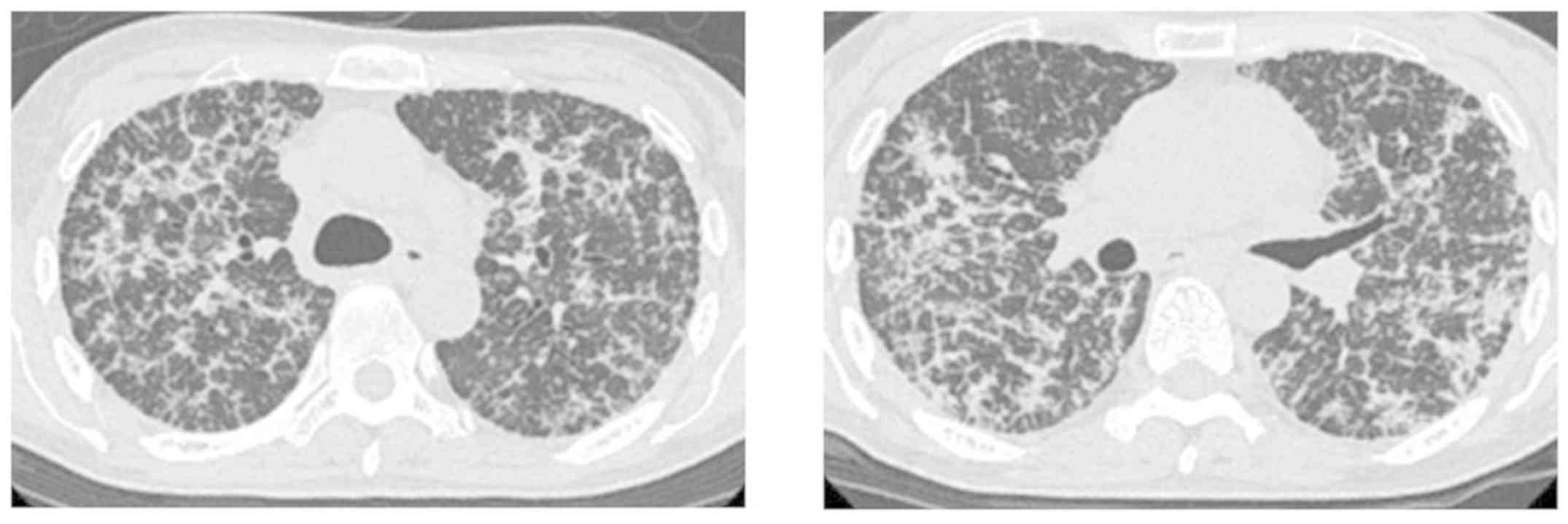
After the first cycle of chemotherapy, CT showed
regression of the nodules and consolidation. Her respiratory
condition dramatically improved, and she was treated with only 1
l/min of nasal oxygen (Fig. 3). At
the same time, her CEA and LDH levels decreased to 42.7 ng/ml and
2,755 U/l, respectively. In May 2019, she received maintenance
therapy with pemetrexed and bevacizumab following four cycles of
platinum-based chemotherapy and continued five cycles of
maintenance therapy until the deterioration of lung metastases.
Discussion
In the present study, we report a case of miliary
lung metastases from ROS1-rearranged lung adenocarcinoma. Miliary
lung metastases have been described as a rare form of metastases
observed in 1-2% of cases of NSCLC (1,2). These
cases are reported to occur more commonly in association with an
EGFR mutation. Laack et al reported five cases of miliary
lung metastases in NSCLCs with exon 19 deletion (4). Hsu et al reported that patients
with NSCLC with an EGFR mutation were three times more likely to
present with miliary metastases than those without the mutation,
indicating the importance of evaluating the status of EGFR mutation
in cases of NSCLC with miliary lung metastases (5). On the other hand, miliary lung
metastases from NSCLC have also been reported with a different
oncogenic driver mutation. Falk et al reported miliary lung
metastases from NSCLC with an ALK rearrangement (6). With regard to ROS1-mutated NSCLC, we
found only one case report of miliary lung metastases: This patient
was successfully treated by crizotinib (3). By contrast, our patient was markedly
improved by combination cytotoxic chemotherapy consisting of
cisplatin, pemetrexed, and bevacizumab after discontinuing
crizotinib treatment. Our case as well as those cited above
indicate that oncogenic driver mutations may be correlated with
miliary lung metastases.
ROS1 rearrangement is considered a rare oncogenic
mutation, reported in only 1-2% of cases of NSCLC (7). Chest physicians should be aware that
miliary lung metastases can develop in patients with lung
adenocarcinoma with oncogenic driver mutations other than an EGFR
mutation, including ROS1 rearrangement. However, crizotinib did not
have a desired effect in our case, whereas one reported case of
miliary lung metastases from ROS1-rearranged lung adenocarcinoma
was successfully treated by crizotinib (3). Although the reason for crizotinib being
ineffective in our case remains unclear, the objective response
rate of crizotinib for ROS1-rearranged NSCLC patients is reportedly
69.3-72%; about 30% of them did not respond to crizotinib
adequately, as seen in our case (8,9).
In conclusion, we present a case of miliary lung
metastases from a ROS1-rearranged lung adenocarcinoma. Chest
physicians should be aware that miliary lung metastases can occur
in patients with NSCLCs with oncogenic driver mutations other than
an EGFR mutation, including ROS1 rearrangement. We await reports of
additional cases similar to ours.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
RO and AS analyzed and interpreted the data and
wrote the manuscript. RO, AS, TK, MA, SI, TB, SK, EH and TO
evaluated the patient and participated in the therapy. KO evaluated
the pathological specimens. All authors have read and approved the
final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient provided written informed consent for
the publication of the case details and any associated images.
Competing interests
Although Dr Sekine and Dr Ikeda have received
lecture fees from Chugai Pharmaceuticals, there was no drug supply
and funding for this study. All authors have stated that they have
no conflicts of interest related to this article to disclose.
References
|
1
|
Umeki S: Association of miliary lung
metastases and bone metastases in bronchogenic carcinoma. Chest.
104:948–950. 1993.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Wu SG, Hu FC, Chang YL, Lee YC, Yu CJ,
Chang YC, Wu JY, Shih JY and Yang PC: Frequent EGFR mutations in
nonsmall cell lung cancer presenting with miliary intrapulmonary
carcinomatosis. Eur Respir J. 41:417–424. 2013. View Article : Google Scholar
|
|
3
|
Brindel A, Huet D, Vaillant P, Vignaud JM
and Tiotiu A: ROS-1 rearranged bronchopulmonary adenocarcinoma
revealed by a pulmonary miliary. Bull Cancer. 105:549–551.
2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Laack E, Simon R, Regier M, Andritzky B,
Tennstedt P, Habermann C, Verth CZ, Thöm I, Grob T, Sauter G and
Bokemeyer C: Miliary never-smoking adenocarcinoma of the lung:
Strong association with epidermal growth factor receptor exon 19
deletion. J Thorac Oncol. 6:199–202. 2011.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Hsu F, Nichol A, Toriumi T and De-Caluwe
A: Miliary metastases are associated with epidermal growth factor
receptor mutations in non-small cell lung cancer: A
population-based study. Acta Oncol. 56:1175–1180. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Falk AT, Poudenx M, Otto J, Ghalloussi H
and Barrière J: Adenocarcinoma of the lung with miliary brain and
pulmonary metastases with echinoderm microtubule-associated protein
like 4-anaplastic lymphoma kinase translocation treated with
crizotinib: A case report. Lung Cancer. 8:282–284. 2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Rothschild SI and Gautschi O: Crizotinib
in the treatment of non-small-cell lung cancer. Clin Lung Cancer.
4:473–480. 2013.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Shaw AT, Ou SH, Bang YJ, Camidge DR,
Solomon BJ, Salgia R, Riely GJ, Varella-Garcia M, Shapiro GI, Costa
DB, et al: Crizotinib in ROS1-rearranged non-small-cell lung
cancer. N Engl J Med. 371:1963–1971. 2014. View Article : Google Scholar
|
|
9
|
Wu YL, Yang JC, Kim DW, Lu S, Zhou J, Seto
T, Yang JJ, Yamamoto N, Ahn MJ, Takahashi T, et al: Phase II study
of crizotinib in east asian patients with ROS1-positive advanced
non-small-cell lung cancer. J Clin Oncol. 36:1405–1411.
2018.PubMed/NCBI View Article : Google Scholar
|