Introduction
One of the most dreadful cancers globally is the
colorectal cancer (CRC), it is rated at the third position among
the prevalent causes of death in both men and women in the world.
The common sites of metastases are abdominal lymph nodes (48.3%),
liver (57.6%), and lungs (37.6%) (1). Nonetheless, bone metastases are also
diagnosed in about 3.7-11% in metastatic CRC (mCRC) patients
(2) and 8.6-27% are describe in
autopsies series cases (3). We
report a case of patient with mCRC with unhabitual bone metastases
presentation.
Case report
A 56 year-old woman with a 6 month history of
persistent and worsening neck pains on the right side without
triggering factor, associated with paresthesia and distal right
upper limb weakness. It was also noted that she had been smoking
for 40 years. An examination was performed, which identified distal
right upper limb deficit estimated at 4/5 on her interosseous
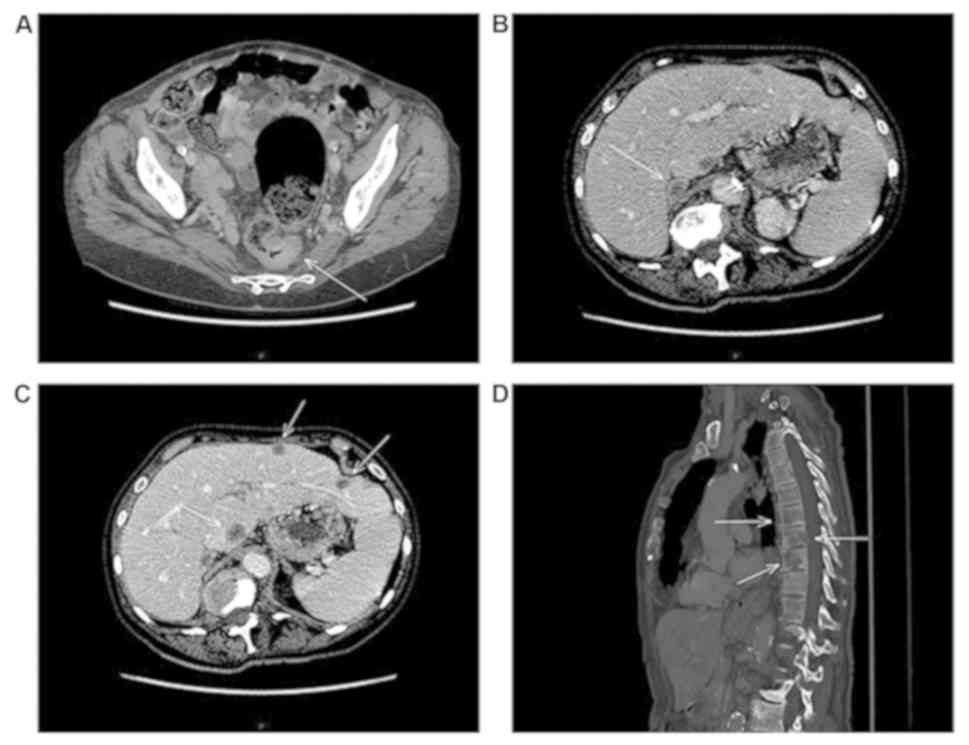
muscles of the right hand. Additionally, a computerized tomography
(CT) of the whole body showed revealed a multiple osteolytic bone
lesions of the cranial vault and the axial and peripheral skeleton,
a multi-nodular liver and both adrenal glands. Furthermore, a mass
of the sigmoid colon was recognized, which was perceived to be the
main tumor (Fig. 1). The subsequent
testing of the blood exhibited high carcioembryonic agent (CEA)
levels at 4,441 µg/l as well as CA 19.9 serum levels of 85 kU/l.
Afterwards, a colonoscopy identified a stenosis, and an ulcerative
circumferential abrasion of 15 cm after the anal margin. The
histological analyses of the biopsies demonstrated that the colic
adenocarcinoma was poorly differentiated (Ki-67:98%, CK7 and CK20
negative; CDX2 affirmative) with NRAS, KRAS, BRAF and PIK3CA
wild-type. Additionally, biopsies of the bone and the liver were
conducted to confirm the analysis of the colonic metastasis.
The patient received only one cycle of the 5-FU,
leucovorin in addition to oxaliplatin (FOLFOX) regime. This was
followed by rapid deterioration of her clinical condition; she
later succumbed to the disease 4 weeks after the diagnoses due to
disease progression.
Discussion
A number of previous studies identified that bone
metastatic colorectal cancer (mCRC) was infrequent (1,2). The
analysis in the United States National Cancer Registry between 2008
and 2013 reported advanced occurrence of the bone metastases CRC at
an earlier age and in male patients. In addition, it was identified
that bone metastases CRC was associated with liver metastasis and
poor survival globally (4,5). That given level of susceptibility may
be due to the patterns of the blood movement commencing at the
colorectal region proceeding to the portal system, as well as the
molecular signaling leading to biological interactions between the
body organs (6).
It is noteworthy that bone metastasis of CRC is a
critical condition that affects the overall condition of the
patient. Bone metastasis of CRC will advance during the period of
diagnosis. Changes in the bowel habit are a common sign of the
disease that may be associated with illness as the patient may
experience poor nutrition. Katagiri et al (7) performed examinations of skeletal
metastases of unidentified origin, and identified that primitive
CRC (2/134 patients) was uncommon and was correlated with worse
universal survival. Hanamura et al (8) described CRC as having a higher
tendency of metastasis in the lungs, the liver and the lymph nodes
at the abdominal regions, and rarely occurring in the bone marrow.
There was a previous case report describing a 60 year-old man who
had sigmoid CRC with bone marrow and lymph node metastasis, with a
similar deterioration in health to the present patient. Table I presents 7 manuscripts that
utilized chemotherapy with different overall survival (OS).
 | Table ILiterature review of 7 manuscripts
detailing bone metastasis in colorectal cancer. |
Table I
Literature review of 7 manuscripts
detailing bone metastasis in colorectal cancer.
| Author, year | Title manuscript | Name Journal | Case description | Mode of
treatment | OS | (Refs) |
|---|
| Hanamura et
al, 2016 | Favorable control of
advance colon adenocarcinoma with sever bone marrow metastasis: A
case report | Mol Clin Oncol | 60-year-old man,
smoker | FOLFOX6 | 10 months | (8) |
| Shah et al,
2014 | An aggressive
presentation of colorectal cancer with an atypical
lymphoproliferative pattern of metastatic disease: A case report
and review of the literature | Clin Colorectal
Cancer | 58-year-old man | FOLFOX with
bevacizumab | 1 months | (9) |
| Sun et al,
2012 | Metastatic
adenocarcinoma involving the bone marrow | Blood | 70-year-old
patient | Surgery and
FOLFOX | 3 months | (5) |
| Wang et al,
2009 | Bone marrow necrosis
caused by metastatic colon cancer | J Clin Oncol
2009 | 37-year-old man | FOLFOX with
cetuximab | 3 months | (10) |
| Pleyer et al,
2007 | Massive infiltration
of bone marrow in colon carcinoma after treatment with activated
protein C | Wien Klin
Wochenschr | Localized CRC
complicated by sepsis which was treated with activated protein
C | FOLFOX4 | 12 months | (11) |
| Lee et al,
2004 | A case of bone marrow
necrosis with thrombocytopenic purpura as a manifestation of occult
colon cancer | Jpn J Clin Oncol | 67-year-old Korean
man | FOLFOX4 | 4 months and 15
days | (12) |
| Suresh Babu et
al, 2000 | Cytokeratin-positive
cells in the bone marrow and survival of patients with stage i, ii
or iii breast cancer | N Engl J Med | 552 patients in stage
I to III | Use of
chemotherapy | 7 months | (1) |
The exact chemotherapeutic treatments to counter
metastases of the bone marrow have not yet been developed and there
have been reports of poor prognosis among the majority of the
patients with CRC. Methodological chemotherapy against metastasis
CRC with bone marrow metastases has also proved ineffective
(8).
However, the benefice to start the denosumab and
bisphosphonates was not evident in our case, because of the rapid
evolution of disease. Moreover, up to date, the benefit and
effectiveness of using denosumab with bisphosphonates in
cancer-related bone injuries has been demonstrated in literature.
The metastasis of the bone in CRC is rare; however, has a poor
prognosis and worsens the quality of life of the patients.
The molecular chromosomal variations can be more
precise markers than clinicopathological characteristics to assess
the prognosis of a patient with early and intermediate stage CRC.
In the examination of 300 patients with stages I-III CRC, for
instance, PIK3CA transformations predicted a poorer prognosis.
However, this was only in the KRAS wild-type patients with CRC.
Furthermore, PIK3CA transformation was correspondingly recognized
as an autonomous biomarker for local recurrence amid stages I-III
CRC; however, there was no convincing analytical significance for
the KRAS transformations for early and intermediate stages of the
CRC. Although a previous study demonstrated that NRAS
transformations could predict a poor prognosis for patients with
CRC with metastases (5), regardless
of the discrepancies in the previous studies, it was suggested that
the biological markers may predict the prognosis of a patient with
CRC at different stages and may aid the individualized selection of
adjuvant treatment for a patient after operation.
Sun et al (5)
identified that in CRC, >20 genes and two RNAs have different
expression patterns at the metastasis stage. In that previous
study, the Gene Ontology pathway analysis demonstrated that
microRNA-429 was involved in CRC. In addition to treatment
decisions, future management should also be considered. Future
studies should aim to perform an in-depth examination of the
molecular structures coupled with genetic studies, to provide
clarification of the pathogenesis of bone metastases. Furthermore,
NRAS proteins, as well as the KRAS proteins, have been found to be
homologous enzymes of the RAS protein group; the genetic
assessments have elucidated variances. Additionally, the NRAS and
the KRAS transformations have been found to have mutually exclusive
mechanisms to prompt carcinogenesis; mutant KRAS prompts too much
propagation and diversification of the human colonic epithelial
cell streaks, whereas, NRAS mutants suppress apoptosis.
In conclusion, CRC is one of the most prevalent
malignancies, causing a large number of deaths worldwide. The
spread of the life-threatening neoplasms into the bone is not due
to accidental progression; however, it involves a number of
molecular interactions coordinated through composite exchanges
between the neoplastic cells and their surroundings. Further
molecular and genetic studies are needed to clarify the
pathogenesis of bone metastases, which will be beneficial in
guiding future management and treatment decisions.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YA and SA collected imaging data, collected
measurements, analyzed the data and wrote the manuscript. WA
performed imaging analyses. ML designed the current study and wrote
the manuscript. SG, PH and SC collected the literature. The final
version of the manuscript has been read and approved by all
authors.
Ethics approval and consent to
participate
The study protocol was approved by the local Ethics
Committee and the Institutional Review Board of Assistance
Publique-Hôpitaux de Paris, Beaujon Hospital.
Patient consent for publication
The patient consented to the publication of data and
associated images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Suresh Babu MC, Garg S, Lakshmaiah KC,
Babu KG, Kumar RV, Loknatha D, Abraham LJ, Rajeev LK, Lokesh KN,
Rudresha AH and Rao SA: Colorectal cancer presenting as bone
metastasis. J Cancer Res Ther. 13:80–83. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kanthan R, Loewy J and Kanthan SC:
Skeletal metastases in colorectal carcinomas: A saskatchewan
profile. Dis Colon Rectum. 42:1592–1597. 1999.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Katoh M, Unakami M, Hara M and Fukuchi S:
Bone metastasis from colorectal cancer in autopsy cases. J
Gastroenterol. 30:615–618. 1995.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Gelson WT, Rimmer MJ, Landells W and Douds
AC: Sacral metastasis as a presentation of colonic adenocarcinoma.
J R Soc Med. 100:191–192. 2007.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Sun Y, Shen S, Tang H, Xiang J, Peng Y,
Tang A, Li N, Zhou W, Wang Z, Zhang D, et al: MiR-429 identified by
dynamic transcriptome analysis is a new candidate biomarker for
colorectal cancer prognosis. OMICS. 18:54–64. 2014.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Schlüter K, Gassmann P, Enns A, Korb T,
Hemping-Bovenkerk A, Hölzen J and Haier J: Organ-Specific
metastatic tumor cell adhesion and extravasation of colon carcinoma
cells with different metastatic potential. Am J Pathol.
169:1064–1073, 169. 2006.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Katagiri H, Takahashi M, Inagaki J,
Sugiura H, Ito S and Iwata H: Determining the site of the primary
cancer in patients with skeletal metastasis of unknown origin: A
retrospective study. Cancer. 86:533–537. 1999.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Hanamura F, Shibata Y, Shirakawa T,
Kuwayama M, Oda H, Ariyama H, Taguchi K, Esaki T and Baba E:
Favorable control of advanced colon adenocarcinoma with severe bone
marrow metastasis: A case report. Mol Clin Oncol. 5:579–582.
2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Shah SM, Rosenthal MH, Griffin GK,
Jacobsen ED and McCleary NJ: Aggressive presentation of colorectal
cancer with an atypical lymphoproliferative pattern of metastatic
disease: A case report and review of the literature. Clin
Colorectal Cancer. 13:5–11. 2014.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Wang YC, Chang PY and Yao NS: Bon arrow
necrosis caused by metastatic colon cancer. J Clin Oncol.
10(e48)2009.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Pleyer L, Went P, Russ G, Prinz E, Faber
V, Röwert HJ, Karlbauer R and Greil R: Massive infiltration of bone
marrow in colon carcinoma after treatment with activated protein C.
Wien Klin Wochenschr. 119:254–258. 2007.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Lee JL, Lee JH, Kim MK, Cho HS, Bae YK,
Cho KH, Bae SH, Ryoo HM, Lee KH and Hyun MS: A case of bone marrow
necrosis with thrombotic thrombocytopenic purpura as a
manifestation of occult colon cancer. Jpn J Clin Oncol. 34:476–480.
2004.PubMed/NCBI View Article : Google Scholar
|