Introduction
Gastric cancer is the fifth most common cancer in
the world (1,033,701 new cases; 5.7% of all cancer cases) with the
third highest cancer-related mortality (782,685 deaths, 8.2% of all
cases) as per GLOBOCAN 2018 data (1). In India, gastric cancer ranks fifth
with regards to the number of newly diagnosed cases (57,394 cases
[5.52%]), and cancer-related mortality (51,429 deaths [7.2%])
(1). Approximately, 95% cases of
gastric cancer are gastric adenocarcinomas (GACs) (2,3) and
most adenocarcinomas arise in the distal third of the stomach and
gastroesophageal junction (GEJ) (4). The incidence of adenocarcinomas, in
the proximal stomach and distal esophagus, has increased over the
years (5).
Taxanes (docetaxel or paclitaxel), which disrupt the
microtubule function and inhibit the process of cell division, have
shown encouraging activity for the treatment of GAC (6,7).
Docetaxel based chemotherapy has been shown to be effective and
well-tolerated in the neoadjuvant therapy of gastric cancer
(8-10).
Furthermore, docetaxel in combination with a platinum agent
(cisplatin/carboplatin/oxaliplatin) and 5-fluorouracil (FU) (DCF)
is a recommended treatment option for advanced gastric cancer
(11,12). Docetaxel as a monotherapy (7,13) or
in combination with other antineoplastic agents such as cisplatin
(14), 5-FU (15), irinotecan (16), carboplatin (17), and capecitabine (18) has demonstrated efficacy in advanced
gastric and GEJ adenocarcinoma.
The conventional docetaxel formulation is associated
with toxicities such as acute hypersensitivity reactions,
cumulative fluid retention, peripheral neuropathy, severe
nonimmunologic anaphylactoid reactions, infusion-site reactions,
and alcohol intoxication, related to the formulation vehicles,
polysorbate 80 and ethanol (19-23).
Furthermore, these adverse effects are still observed despite
corticosteroid and antihistamine premedications, which are
generally used to limit these toxicities (24). A novel lipid-based formulation of
docetaxel, nanosomal docetaxel lipid suspension (NDLS,
DoceAqualip), which is devoid of polysorbate 80 and ethanol was
developed to overcome these toxicity issues. NDLS is approved in
India for the treatment of patients with advanced gastric
adenocarcinoma, androgen independent (hormone refractory)
metastatic prostate cancer (HRPC), locally advanced or metastatic
breast cancer (MBC) after failure of prior chemotherapy, non-small
cell lung cancer (NSCLC) after failure of prior chemotherapy, and
for the induction treatment of locally advanced squamous cell
carcinoma of head and neck (LA SCCHN). NDLS was developed based on
the patented ‘NanoAqualip’ technology (patent numbers: Worldwide
(WO2008127358), Europe (2076244), Japan (5917789) and Canada
(CA2666322) (25) using lipids
generally regarded as safe (GRAS) by the US Food and Drug
Administration (USFDA). Docetaxel is added to high pressure
homogenized soy phosphatidylcholine and sodium cholesteryl sulfate
in sodium citrate buffer under continuous high pressure
homogenization for the development of NDLS (25). The resultant nanosomal (<100 nm)
particles (25) of NDLS may
increase the delivery of docetaxel to tumor tissues due to damaged
tumor vasculature, resulting in an enhanced permeability and
retention (EPR) effect. This may result in a greater systemic
availability of docetaxel (25,26)
and thus, improved therapeutic outcomes can be potentially expected
(27). In addition, polysorbate 80
and ethanol related toxicity issues can be circumvented as
well.
The efficacy and safety of NDLS has been
demonstrated in breast, ovarian, cervical, gastric, penile, hormone
refractory prostate cancer, non-small cell lung cancer and sarcoma
(28-32).
We report here a multicenter, retrospective experience in real-life
practice evaluating the efficacy and safety of NDLS based
chemotherapy in the treatment of gastric and GEJ adenocarcinomas in
the neoadjuvant and metastatic settings.
Materials and methods
Study design
In this multicenter, retrospective study, we
analyzed the medical charts of adult patients who were treated with
NDLS based chemotherapy as part of their routine clinical care for
histopathologically proven gastric and GEJ adenocarcinoma. The data
is captured from April 2014 to October 2018. The study endpoints
were overall response rate [ORR: Proportion of patients achieving
complete (CR)+partial response (PR)], disease control rate [DCR:
CR+PR+stable disease (SD)] and overall survival (OS was defined as
time from treatment to death due to any cause; for patients who
were still alive at the time of data analysis or who were lost to
follow-up, OS was censored at the last recorded date that the
patient was known to be alive). Treatment response was evaluated
using the Response Evaluation Criteria in Solid Tumors (RECIST)
1.1(33). Incidence of adverse
events (AEs) documented in the treatment charts were recorded and
graded according to the National Cancer Institute Common
Terminology Criteria for Adverse Events (CTCAE) Criteria version
5.0. Similarly, data on deaths and discontinuations were captured
from the patients' health records.
Ethics statement
The study protocol was reviewed and approved by the
OM Ethics Committee, Ahmedabad, India. The study was conducted in
accordance with the Ethical principles that have their origin in
the Declaration of Helsinki, and in accordance with the
International Conference on Harmonization's Good Clinical Practice
guidelines (ICH-GCP), applicable regulatory requirements, and in
compliance with the protocol.
Statistical analysis
Demographic and baseline characteristics were
summarized using descriptive statistics. Categorical variables were
summarized with frequency and percentage. Continuous variables were
summarized with count, mean, standard deviation, median, minimum
and maximum. Response rate was presented as frequency and
percentage of patients. Survival analysis was performed to measure
lifetime or the amount of time until the occurrence of an event
(death in case of overall survival). Survival data was analyzed
using a non-parametric procedure performed PROC LIFETEST of SAS
(Version 9.4) to measure the duration of time until a specified
event occurs. OS was calculated and analyzed using the Kaplan-Meier
method and the log-rank test to estimate the survival function from
lifetime data after treatment. The AEs were summarized as
frequencies and percentages by type of reactions.
Results
Patients disposition and
demographics
Data of 43 patients with gastric (n=39) and GEJ
(n=4) adenocarcinomas who were treated with NDLS based chemotherapy
regimens was retrospectively analyzed. The baseline characteristics
of these patients are summarized in Table I.
 | Table IPatient disposition and baseline
characteristics. |
Table I
Patient disposition and baseline
characteristics.
| Parameters | All patients
(n=43) | Neoadjuvant setting
(n=18) | Metastatic setting
(n=25) |
|---|
| Age (years), mean ±
SD, range | 55.14 ±10.7
(34-75) | 54.8±11.4
(34-73) | 55.3±10
(38-75) |
| BSA,
kg/m2, mean ± SD | 1.54±0.2 | 1.6±0.2 | 1.54±0.24 |
| Sex, n (%) |
|
Male | 31 (72.1) | 16 (88.9) | 15 (60) |
|
Female | 12 (27.9) | 2 (11.1) | 10 (40) |
| Cancer Stage, n
(%) | | | |
|
II | 6 (14.0) | 6 (33.3) | - |
|
III | 10 (23.3) | 10 (55.6) | - |
|
IV | 27 (62.8) | 2 (11.1) | 25 (100.0) |
| NDLS dose, n
(%) | | | |
|
75
mg/m2 | 37 (86.0) | 15 (83.3) | 22 (88.0) |
|
50
mg/m2 | 6 (14.0) | 3 (16.7) | 3 (12.0) |
| Metastasis site, n
(%)a | | | |
|
Lymph
node | 10 (23.3) | - | 10 (40.0) |
|
Bone | 2 (4.7) | - | 2 (8.0) |
|
Liver | 1 (2.3) | | 1 (4.0) |
| Line of therapy, n
(%) | | | |
|
First-line | 38 (88.4) | 18 (100.0) | 20 (80.0) |
|
Second-line | 4 (9.3) | - | 4 (16.0) |
|
Third-line | 1 (2.3) | - | 1 (4.0) |
| ECOG performance
score | | | |
|
0 | 3 (7.0) | - | 3 (12.0) |
|
1 | 37 (86.0) | 18 (100.0) | 19 (76.0) |
|
2 | 3 (7.0) | - | 3 (12.0) |
| Comorbid disease, n
(%) | | | |
|
Hypertension | 13 (30.2) | 2 (11.1) | 11 (44.0) |
|
Diabetes | 5 (11.6) | 1 (5.6) | 4 (16.0) |
|
Hypothyroidism | 5 (11.6) | 2 (11.1) | 3 (12.0) |
|
Others | 3 (7.0) | 3 (16.7) | - |
NDLS was administered as a 1 h infusion in 3 weekly
cycles at a dose of 75 mg/m2 (n=37, 86%) and 50
mg/m2 (n=6, 14%). NDLS was used as a first-line therapy
in majority (90.7%) of the patients. Granulocyte-colony stimulating
factor (GCSF) was used in majority of the patients (90.7%, 39/43)
as primary prophylaxis.
NDLS based treatment regimens.
The most common NDLS based treatment regimen in the
neoadjuvant setting was NDLS/oxaliplatin/capecitabine [DOX, 50%
(9/18 patients)] followed by NDLS/oxaliplatin/5-FU [DOF, 33.3%
(6/18 patients)]. In the metastatic setting, NDLS/cisplatin/5-FU
[DCF, 28% (7/25 patients)] followed by DOF (24%, 6/25 patients)
were the most commonly used regimens.
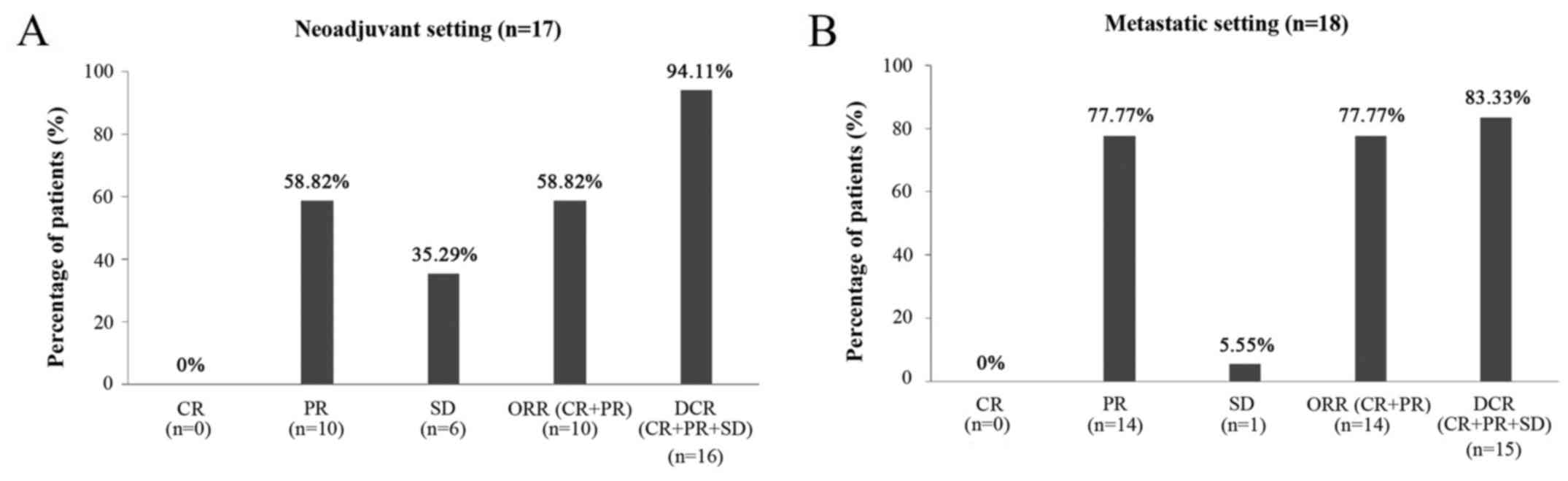
Efficacy
Of 43 patients who received NDLS based chemotherapy
for the treatment of gastric and GEJ adenocarcinoma in neoadjuvant
and metastatic settings, efficacy evaluation was available for 35
patients (17/18 patients in neoadjuvant and 18/25 patients in
metastatic setting). In the neoadjuvant setting, the ORR and DCR
were 58.82 and 94.11%, respectively (Fig. 1A) whereas in the metastatic setting,
the ORR and DCR were 77.77 and 83.33%, respectively (Fig. 1B).
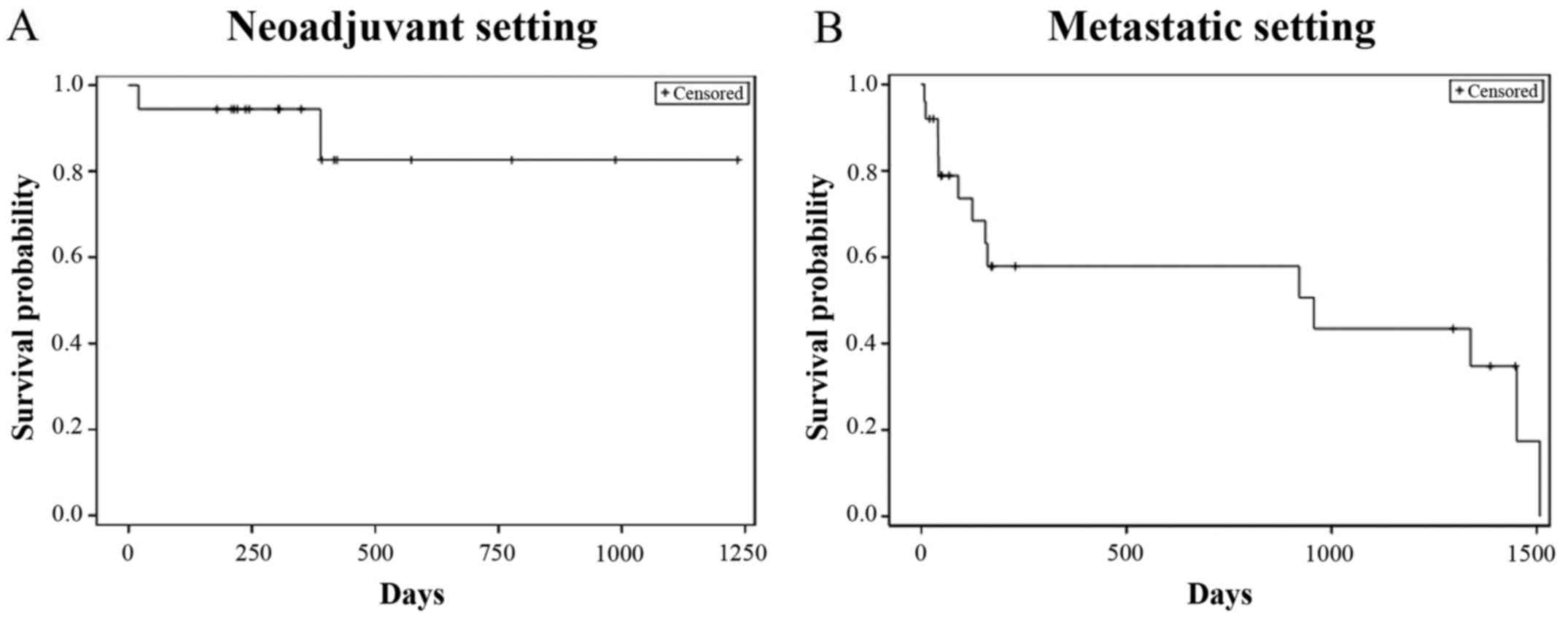
Overall survival
The patient survival data was collected from the
date of administration of the first dose of NDLS based therapy till
the last follow-up date (September 30, 2018) for alive patients and
date of death for patients who died. The proportion of patients who
were alive at the last follow-up was 88.9% (16/18) in the
neoadjuvant setting and the median OS was not reached (follow-up
duration: 0.7-41.2 months) (Fig.
2A). In the metastatic setting, the proportion of patients who
were alive at the last follow-up was 56% (14/25) and the median OS
was 31.9 months (follow-up duration: 0.2-50.3 months) (Fig. 2B).
Safety
The data on AEs was available for 33 (76.7%)
patients. Of these, at least 1 AE was reported in 72.7% (24/33)
patients. Grade 1 AEs were reported in 69.7% (23/33) patients,
grade 2 in 30.3% (10/33), grade 3 in 12.1% (4/33) and grade 4 in
9.1% (3/33) patients, respectively. Anemia, lymphopenia
thrombocytopenia, and neutropenia were the hematological AEs
reported while nausea, vomiting and weakness were the most-common
non-hematological AEs reported (Table
II).
| Table IISafety profile of NDLS in patients
with gastric and GEJ adenocarcinoma (n=33). |
Table II
Safety profile of NDLS in patients
with gastric and GEJ adenocarcinoma (n=33).
| A, Hematological
AEs |
|---|
| Adverse event
(>5% patients) | All grades, n
(%) | Grade III, n
(%) | Grade IV, n
(%) |
|---|
| Anemia | 18 (54.55) | 1 (1.92) | - |
| Lymphopenia | 7 (21.21) | 2 (3.85) | - |
|
Thrombocytopenia | 6 (18.18) | 1 (1.92) | 2 (3.85) |
| Neutropenia | 4 (12.12) | 1 (1.92) | 1 (1.92) |
| B,
Non-hematological AEs |
| Adverse event
(>5% patients) | All grades, n
(%) | Grade III, n
(%) | Grade IV, n
(%) |
| Nausea | 5 (15.15) | - | - |
| Vomiting | 5 (15.15) | - | - |
| Weakness | 5 (15.15) | - | - |
| Hyperglycemia | 4 (12.12) | - | - |
| Anorexia | 3 (9.09) | - | - |
| Diarrhea | 3 (9.09) | - | - |
| Alteration in
LFT | 3 (9.09) | 2 (3.85) | - |
| Mouth ulcer | 2 (6.06) | - | - |
| Mucositis | 2 (6.06) | - | - |
| Alopecia | 2 (6.06) | - | - |
Discussion
Addition of docetaxel to the therapeutic
armamentarium of gastric and GEJ adenocarcinoma has demonstrated
improved treatment outcomes (34).
Docetaxel based chemotherapy is recommended as neoadjuvant therapy
for gastric cancer. Furthermore, docetaxel as a monotherapy or as
combination therapy is recommended for unresectable locally
advanced, recurrent or metastatic gastric adenocarcinoma (35). The current study presents the
findings of NDLS based chemotherapy in patients with gastric and
GEJ cancer in neoadjuvant and metastatic settings.
Neoadjuvant treatment remains the gold standard for
the treatment of locally advanced gastric cancer, which aims at
‘downstaging’ the tumor and eliminating the spread of tumor cells
or lymph node metastases (36). The
available evidence suggests a role for neoadjuvant docetaxel-based
chemotherapy in downstaging the cancer, achieving complete surgical
resection and probably improving the outcome in patients with
locally advanced GAC (37).
An ORR of 44-70% has been reported with docetaxel
based regimens in neoadjuvant treatment of gastric cancer (8-10)
whereas in our study, NDLS based neoadjuvant chemotherapy
demonstrated an ORR of 58.8%. Yahyazadeh-Jabbari et al,
evaluated the efficacy and safety of
docetaxel/oxaliplatin/capecitabine (DOX) regimen in 49 patients
with resectable gastric and GEJ cancers, and reported an ORR of
48.9% (8). Another study by Spigel
et al showed an ORR of 61% with DOX regimen in 49 patients
with localized carcinoma of the esophagus or gastroesophageal
junction (9). In our study,
NDLS-based DOX regimen resulted in an ORR of 44.4% (4/9 patients)
and a DCR of 88.9% (8/9 patients). The combination of
docetaxel/oxaliplatin/5-FU (DOF regimen) as neoadjuvant
chemotherapy in the treatment of advanced gastric cancer (n=68)
showed an ORR of 70.6% (10). In
our study, NDLS based DOF regimen was administered in 6 patients in
the neoadjuvant setting and demonstrated an ORR of 66.7% and DCR of
100%. Pathological response and R0 resection are potent
surrogate factors for evaluating the efficacy of neoadjuvant
chemotherapy (38,39); however, these were not available in
the present study, and the results are provided based on RECIST
1.1. In our study, at a follow-up duration ranging from 0.7 to 41.2
months, the median OS was not reached with NDLS based neoadjuvant
chemotherapy; and 88.9% patients were alive at the last
follow-up.
Docetaxel based regimens have been associated with
an ORR of 37-73% in the treatment of metastatic gastric cancer
(11,40,41).
In our study, NDLS based chemotherapy showed an ORR of 77.77% and a
median OS of 31.9 months for patients receiving NDLS based
chemotherapy in the metastatic setting. The use of docetaxel for
the treatment of metastatic GAC as DCF regimen was approved by the
US FDA based on TAX 325 study (n=221), (11) which demonstrated an ORR of 37%, and
a median OS of 9.2 months (11).
Another study by the Swiss Group for Clinical Cancer Research
reported an ORR of 36.6% for DCF regimen in metastatic GAC (median
OS: 10.4 months) (40). In our
study, patients receiving NDLS based DCF regimen in the metastatic
setting reported an ORR of 80% (PR: 80%, 4/5 patients) and a DCR of
100% [PR: 80% (4/5 patients), SD: 20% (1/5 patients)]. In a study
by Rosenberg et al, the DOF regimen resulted in an ORR of
73.2% in the treatment of metastatic or unresectable gastric or GEJ
adenocarcinoma (median OS: 10.3 months) (41). In our study, NDLS based DOF regimen
showed partial response in all 5 patients evaluated in the
metastatic setting (ORR: 100%).
Polysorbate 80 and ethanol, which are used as
formulation vehicles in the conventional docetaxel formulation,
have been implicated in the AEs such as acute hypersensitivity
reactions, cumulative fluid retention, peripheral neuropathy
(19), severe nonimmunologic
anaphylactoid reactions (20),
injection-site reactions (21), and
alcohol intoxication (22,23). Corticosteroid premedication is
generally used with docetaxel based chemotherapy to circumvent the
aforementioned AEs, however, these AEs can still be observed
despite premedication (24). In our
study, AEs like neurotoxicity, fluid retention and acute
hypersensitivity reactions were not reported with NDLS based
chemotherapy. Anemia, lymphopenia, thrombocytopenia and neutropenia
were the hematological AEs whereas nausea, vomiting, weakness and
hyperglycemia were the most common (≥10%) non-hematological AEs
reported in our study. Anemia (10.2%), nausea (10.2%) and vomiting
(6.1%) were the most frequent grade 3/4 AEs with DOX regimen
(8). In the study by Spigel et
al, the most common (≥5%) grade 3/4 nonhematologic AEs
associated with DOX regimen were anorexia (20%), esophagitis (20%),
nausea (16%), vomiting (16%), dehydration (16%), pulmonary symptoms
(14%), fatigue (12%), dysphagia (10%), diarrhea (8%), hyperglycemia
(6%) and sepsis (6%) (9). In the
metastatic setting, the grade 3/4 AEs observed with the DCF regimen
were: Neutropenia (82%), stomatitis (21%), diarrhea (19%) and
lethargy (19%) (11). In a review
by Di Cosimo et al, neutropenia was the most common grade
3/4 AE occurring in 50-81% patients with advanced gastric cancer
receiving docetaxel based triplet chemotherapy (42). NDLS was mostly used at 75
mg/m2 in our study and was found to be well-tolerated.
Severe grade 4 neutropenia and thrombocytopenia were reported in
1.9% and 3.9% patients. The most commonly reported grade 3/4 AEs
were lymphopenia (3.9%), anemia, thrombocytopenia and neutropenia
(1.9% each).
Corticosteroids premedication is routinely
administered in patients receiving conventional docetaxel to
mitigate the toxicity issues such as hypersensitivity and fluid
retention (43). In a recent study,
Obradović et al used transcriptional profiling of tumors and
matched metastases in patient-derived xenograft models in mice and
suggested the possible role of glucocorticoid receptor (GR)
activation resulting in breast cancer progression and metastasis
(44). Corticosteroid premedication
is not warranted with the NDLS formulation, especially when used as
monotherapy, hence, it may potentially help in circumventing the
risk of disease progression.
As this is a retrospective data collection study,
lack of completeness of data for safety as well as survival data is
a major limitation. Also, the details pertaining to tumor size and
resectability was not captured in the patient records, hence, could
not be presented for patients receiving NDLS in the neoadjuvant
setting. The progression-free survival (PFS) could not be captured
in this study since, being a real-world study, the data on
progression and serial scans were not available for most of the
patients at most of the follow-up timepoints.
In conclusion, nanosomal docetaxel lipid suspension
(NDLS) based regimens were effective and well-tolerated in managing
gastric cancer in neoadjuvant and metastatic settings. This study
provides valuable insights into the safety and efficacy of NDLS
based chemotherapy in the management of gastric and
gastroesophageal junction adenocarcinoma. A clinical trial is
underway to evaluate the safety and efficacy of NDLS based
treatment in gastric cancer.
Acknowledgments
The authors would like to thank Mr. Shreekant Sharma
(ISMPP CMPPTM; Intas Pharmaceuticals Ltd., Ahmedabad,
Gujarat, India) for providing writing assistance and Dr Venugopal
Madhusudhana (ISMPP CMPPTM; Intas Pharmaceuticals Ltd.,
Ahmedabad, Gujarat, India) for additional editorial assistance when
developing the manuscript.
Funding
The present study was funded by an unrestricted
research grant by Intas Pharmaceuticals Ltd. (Ahmedabad, Gujarat,
India), towards statistical analysis and manuscript writing.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
SS, SKDM and GB conducted the research, acquired the
data and critically revised the manuscript for important
intellectual content. NJ, DB, MAK and IA designed the study, were
involved in data interpretation and critically revised the
manuscript for important intellectual content. All authors made
substantial contributions to this study and agree to be accountable
for all aspects of the work. All authors read and approved the
final manuscript.
Ethical approval and consent to
participate
The study protocol was reviewed and approved by the
OM Ethics Committee (Ahmedabad, India). The current study was
conducted in accordance with the ethical principles of the
Declaration of Helsinki, the International Conference on
Harmonization's Good Clinical Practice guidelines and applicable
regulatory requirements. Patient consent to review their medical
records was not required by the Ethics Committee as NDLS is already
approved in India and patient confidentiality was completely
maintained. In this retrospective study, no patient identifiers
were used and data were anonymized.
Patient consent for publication
Not applicable.
Competing interests
Drs. Mujtaba A. Khan, Deepak Bunger and Nisarg Joshi
are employees of Intas Pharmaceutical Ltd., India. Dr Imran Ahmad
is an employee of Jina Pharmaceutical Inc., USA.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Hunt N and McHale S: The psychological
impact of alopecia. BMJ. 331:951–953. 2005.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ajani JA, Lee J, Sano T, Janjigian YY, Fan
D and Song S: Gastric adenocarcinoma. Nat Rev Dis Primers.
3(17036)2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Lerut T: Carcinoma of the esophagus and
gastro-esophageal junction. In: Surgical Treatment: Evidence-Based
and Problem-Oriented. Holzheimer RG, Mannick JA (eds).
Zuckschwerdt, Munich, 2001. Available from: https://www.ncbi.nlm.nih.gov/books/NBK6982/.
Accessed March 20, 2020.
|
|
5
|
Gee DW and Rattner DW: Management of
gastroesophageal tumors. Oncologist. 12:175–185. 2007.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sakamoto J, Matsui T and Kodera Y:
Paclitaxel chemotherapy for the treatment of gastric cancer.
Gastric Cancer. 12:69–78. 2009.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Bang YJ, Kang WK, Kang YK, Kim HC, Jacques
C, Zuber E, Daglish B, Boudraa Y, Kim WS, Heo DS and Kim NK:
Docetaxel 75mg/m(2) is active and well tolerated in patients with
metastatic or recurrent gastric cancer: A phase II trial. Jpn J
Clin Oncol. 32:248–254. 2002.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Yahyazadeh-Jabbari SH, Malekpour N,
Salmanian B, Foodazi H, Salehi M and Noorizadeh F: The phase 2
study of ‘(TOX) preoperative chemotherapy’ response rate and side
effects in [Locally Advanced Operable Gastric Adenocarcinoma]
patients with docetaxel, oxaliplatin and capcitabine. Iran J Cancer
Prev. 6:133–140. 2013.PubMed/NCBI
|
|
9
|
Spigel DR, Greco FA, Meluch AA, Lane CM,
Farley C, Gray JR, Clark BL, Burris HA III and Hainsworth JD: Phase
I/II trial of preoperative oxaliplatin, docetaxel, and capecitabine
with concurrent radiation therapy in localized carcinoma of the
esophagus or gastroesophageal junction. J Clin Oncol. 28:2213–2219.
2010.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Zhen Y, Xu Z, Sun Y, Guo H, Gong W, Chai J
and Li Z: DOF as neoadjuvant chemotherapy in the treatment of
advanced gastric cancer. Chin J Clin Oncol. 38:564–567. 2011.
|
|
11
|
Van Cutsem E, Moiseyenko VM, Tjulandin S,
Majlis A, Constenla M, Boni C, Rodrigues A, Fodor M, Chao Y, Voznyi
E, et al: Phase III study of docetaxel and cisplatin plus
fluorouracil compared with cisplatin and fluorouracil as first-line
therapy for advanced gastric cancer: A report of the V325 study
group. J Clin Oncol. 24:4991–4997. 2006.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Nishiyama M and Wada S: Docetaxel: Its
role in current and future treatments for advanced gastric cancer.
Gastric Cancer. 12:132–141. 2009.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Einzig AI, Neuberg D, Remick SC, Karp DD,
O'Dwyer PJ, Stewart JA and Benson AB III: Phase II trial of
docetaxel (Taxotere) in patients with adenocarcinoma of the upper
gastrointestinal tract previously untreated with cytotoxic
chemotherapy: The eastern cooperative oncology group (ECOG) results
of protocol E1293. Med Oncol. 13:87–93. 1996.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Ridwelski K, Gebauer T, Fahlke J, Kroning
H, Kettner E, Meyer F, Eichelmann K and Lippert H: Combination
chemotherapy with docetaxel and cisplatin for locally advanced and
metastatic gastric cancer. Ann Oncol. 12:47–51. 2001.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Constenla M, Garcia-Arroyo R, Lorenzo I,
Carrete N, Campos B and Palacios P: Docetaxel, 5-fluorouracil, and
leucovorin as treatment for advanced gastric cancer: Results of a
phase II study. Gastric Cancer. 5:142–147. 2002.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Roy A, Cunningham D, Hawkins R, Sörbye H,
Adenis A, Barcelo JR, Lopez-Vivanco G, Adler G, Canon JL, Lofts F,
et al: Docetaxel combined with irinotecan or 5-fluorouracil in
patients with advanced oesophago-gastric cancer: A randomised phase
II study. Br J Cancer. 107:435–441. 2012.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Kurt E, Cubukcu E, Karabulut B, Olmez OF,
Kurt M, Avci N, Ozdemir F, Tunali D, Evrensel T and Manavoglu O: A
multi-institutional evaluation of carboplatin plus docetaxel
regimen in elderly patients with advanced gastric cancer. J BUON.
18:147–153. 2013.PubMed/NCBI
|
|
18
|
Thuss-Patience PC, Kretzschmar A, Dogan Y,
Rothmann F, Blau I, Schwaner I, Breithaupt K, Bichev D, Grothoff M,
Grieser C and Reichardt P: Docetaxel and capecitabine for advanced
gastric cancer: Investigating dose-dependent efficacy in two
patient cohorts. Br J Cancer. 105:505–512. 2011.PubMed/NCBI View Article : Google Scholar
|
|
19
|
ten Tije AJ, Verweij J, Loos WJ and
Sparreboom A: Pharmacological effects of formulation vehicles:
Implications for cancer chemotherapy. Clin Pharmacokinet.
42:665–685. 2003.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Coors EA, Seybold H, Merk HF and Mahler V:
Polysorbate 80 in medical products and nonimmunologic anaphylactoid
reactions. Ann Allergy Asthma Immunol. 95:593–599. 2005.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Schwartzberg LS and Navari RM: Safety of
polysorbate 80 in the oncology setting. Adv Ther. 35:754–767.
2018.PubMed/NCBI View Article : Google Scholar
|
|
22
|
FDA Drug Safety Communication (2014, June
20). FDA warns that cancer drug docetaxel may cause symptoms of
alcohol intoxication after treatment. Available from: https://www.fda.gov/Drugs/DrugSafety/ucm401752.htm.
Accessed March 20, 2020.
|
|
23
|
Mirza A and Mithal N: Alcohol intoxication
with the new formulation of docetaxel. Clin Oncol (R Coll Radiol).
23:560–561. 2011.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Ho MY and Mackey JR: Presentation and
management of docetaxel-related adverse effects in patients with
breast cancer. Cancer Manag Res. 6:253–259. 2014.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Ahmad A, Sheikh S, Ali SM, Ahmad MU,
Paithankar M, Saptarishi D, Maheshwari K, Kumar K, Singh J and
Patel G: Development of aqueous based formulation of docetaxel:
Safety and pharmacokinetics in patients with advanced solid tumors.
J Nanomed Nanotechnol. 6(1)2015.
|
|
26
|
Lewis LD, Miller AA, Rosner GL, Dowell JE,
Valdivieso M, Relling MV, Egorin MJ, Bies RR, Hollis DR, Levine EG,
et al: A comparison of the pharmacokinetics and pharmacodynamics of
docetaxel between African-American and Caucasian cancer patients:
CALGB 9871. Clin Cancer Res. 13:3302–3311. 2007.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Ahmad A, Sheikh S, Taran R, Srivastav SP,
Prasad K, Rajappa SJ, Kumar V, Gopichand M, Paithankar M, Sharma M,
et al: Therapeutic efficacy of a novel nanosomal docetaxel lipid
suspension compared with taxotere in locally advanced or metastatic
breast cancer patients. Clin Breast Cancer. 14:177–181.
2014.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Ashraf M, Sajjad R, Khan M, Shah M, Bhat Y
and Wani Z: 156P Efficacy and safety of a novel nanosomal docetaxel
lipid suspension (NDLS) as an anti cancer agent-a retrospective
study. Ann Oncol. 27:ix46–ix51. 2016.
|
|
29
|
Naik R and Khan MA: Doceaqualip in a
patient with prostate cancer who had an allergic reaction to
conventional docetaxel: A case report. Mol Clin Oncol. 6:341–343.
2017.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Prasanna R, Bunger D and Khan MA: Efficacy
and safety of DoceAqualip in a patient with locally advanced
cervical cancer: A case report. Mol Clin Oncol. 8:296–299.
2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Vyas V, Joshi N and Khan M: Novel
docetaxel formulation (NDLS) in low cardiac reserve ovarian cancer.
Open Access J Cancer Oncol. 2(000122)2018.
|
|
32
|
Gupta S, Pawar SS and Bunger D: Successful
downstaging of locally recurrent penile squamous cell carcinoma
with neoadjuvant nanosomal docetaxel lipid suspension (NDLS) based
regimen followed by curative surgery. BMJ Case Rep.
2017(bcr2017220686)2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Tetzlaff ED, Cheng JD and Ajani JA: Review
of docetaxel in the treatment of gastric cancer. Ther Clin Risk
Manag. 4:999–1007. 2008.PubMed/NCBI View Article : Google Scholar
|
|
35
|
NCCN Clinical Practice Guidelines in
Oncology (NCCN Guidelines®). Gastric Cancer. Version 1.2019-March
14, 2019. https://www.nccn.org/professionals/physician_gls/pdf/gastric.pdf.
July 1, 2020.
|
|
36
|
Menges M and Hoehler T: Neoadjuvant
therapy of gastric cancer: A decisive step forward. Gastrointest
Tumors. 1:99–104. 2014.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Inno A, Basso M, Cassano A and Barone C: A
review of docetaxel: Its use in the treatment of gastric cancer.
Clin Med Insights 2: https://journals.sagepub.com/doi/10.4137/CMT.S5191.
|
|
38
|
Pauligk C, Tannapfel A, Meiler J, Luley
KB, Kopp HG, Homann N, Hofheinz RD, Schmalenberg H, Probst S, Haag
GM, et al: Pathological response to neoadjuvant 5-FU, oxaliplatin,
and docetaxel (FLOT) versus epirubicin, cisplatin, and 5-FU (ECF)
in patients with locally advanced, resectable
gastric/esophagogastric junction (EGJ) cancer: Data from the phase
II part of the FLOT4 phase III study of the AIO. J Clin Oncol.
33:4016. 2015.
|
|
39
|
Hu SB, Liu CH, Wang X, Dong YW, Zhao L,
Liu HF, Cao Y, Zhong DR, Liu W, Li YL, et al: Pathological
evaluation of neoadjuvant chemotherapy in advanced gastric cancer.
World J Surg Oncol. 17(3)2019.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Roth AD, Fazio N, Stupp R, Falk S,
Bernhard J, Saletti P, Koberle D, Borner MM, Rufibach K, Maibach R,
et al: Docetaxel, cisplatin, and fluorouracil; docetaxel and
cisplatin; and epirubicin, cisplatin, and fluorouracil as systemic
treatment for advanced gastric carcinoma: A randomized phase II
trial of the Swiss group for clinical cancer research. J Clin
Oncol. 25:3217–3223. 2007.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Rosenberg AJ, Rademaker A, Hochster HS,
Ryan T, Hensing T, Shankaran V, Baddi L, Mahalingam D, Mulcahy MF
and Benson AB III: Docetaxel, oxaliplatin, and 5-fluorouracil (DOF)
in metastatic and unresectable gastric/gastroesophageal junction
adenocarcinoma: A phase II study with long-term follow-up.
Oncologist. 24:1039–e642. 2019.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Di Cosimo S, Ferretti G, Fazio N,
Silvestris N, Carlini P, Alimonti A, Gelibter A, Felici A, Papaldo
P and Cognetti F: Docetaxel in advanced gastric cancer-review of
the main clinical trials. Acta Oncol. 42:693–700. 2003.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Weiss RB, Donehower RC, Wiernik PH, Ohnuma
T, Gralla RJ, Trump DL, Baker JR Jr, Van Echo DA, Von Hoff DD and
Leyland-Jones B: Hypersensitivity reactions from taxol. J Clin
Oncol. 8:1263–1268. 1990.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Obradović MMS, Hamelin B, Manevski N,
Couto JP, Sethi A, Coissieux MM, Münst S, Okamoto R, Kohler H,
Schmidt A and Bentires-Alj M: Glucocorticoids promote breast cancer
metastasis. Nature. 567:540–544. 2019.PubMed/NCBI View Article : Google Scholar
|