Introduction
Robot-assisted radical prostatectomy (RARP) is
currently the gold standard surgical procedure for localized
prostate cancer (PC). Although RARP is reportedly associated with
safer surgery and better oncological outcomes than conventional
open radical prostatectomy (ORP) (1), RARP has risks of specific
complications due to the use of carbon dioxide pneumoperitoneum and
a steep Trendelenburg position (2,3). Acute
kidney injury (AKI) is a serious postoperative complication
especially after laparoscopic surgery; however, the link between
RARP and AKI is controversial (2-6).
A previous study reported that the postoperative serum creatinine
(sCre) concentration increased in patients who underwent RARP but
decreased in those who underwent ORP (2). To the contrary, another study reported
that the incidence of AKI after RARP was significantly lower than
that after ORP (5). Yet other
studies reported that postoperative renal function was unaltered in
patients who underwent RARP (3,6).
Therefore, there is currently no consensus regarding the risk of
AKI after RARP. Furthermore, long-term follow-up data on changes in
renal function after RARP are also lacking. The present study aimed
to compare the incidences of postoperative AKI between RARP and
ORP, as well as long-term changes in postoperative renal function
between them.
Patients and methods
Patients and surgical techniques
We retrospectively reviewed 257 patients with PC who
underwent either RARP (n=187) or ORP (n=70) at our institution from
2011 to 2014. Since RARP started to be covered by Japanese public
health insurance in 2012, most patents underwent ORP between 2011
and the first half of 2012, while majority of patients received
RARP after the second half of 2012. We performed RARP using the
peritoneal approach as previously described (1) and ORP using the conventional
retroperitoneal approach, respectively. Patients who underwent RARP
were placed in the Trendelenburg position at an angle of 25̊ from
the horizontal plane. Lymph node dissection was performed in RARP
patients who were predicted to have ≥5% lymph node metastasis
according to the Japan PC nomogram (7) and in all ORP patients. Cavernous nerve
preservation was carried out on the cancer-negative lobe in RARP
patients; bilateral preservation was limited only when the
patient's cancer was located at the transitional zone. In ORP
patients, cavernous nerve preservation was performed in a limited
number of patients. All patients underwent pretreatment
evaluations, including blood tests, chest x-rays, computed
tomography, and bone scintigraphy. Posttreatment monitoring was
generally performed with routine blood tests including
prostate-specific antigen (PSA) every 1-6 months.
The present study was approved by the Internal
Institutional Review Board of Graduate School of Medicine and
Faculty of Medicine, University of Tokyo (approval no. 3124).
Written informed consent was obtained from each patient prior to
surgery. Patients were given the opportunity to decline
participation in the study through the opt-out form on our
website.
Evaluation protocol of postoperative
renal function and definition of AKI
The sCre concentration was measured at the following
six time points: Prior to surgery, immediately after surgery
(postoperative day 0 [POD0]), on POD1, 3 months after surgery, 1
year after surgery, and 2 years after surgery. Postoperative AKI on
POD0 and POD1 was diagnosed according to the Kidney Disease:
Improving Global Outcomes (KDIGO) criteria (8,9): An
increase in sCre by ≥0.3 mg/dl within 48 h, an increase in sCre to
≥1.5 times baseline within the previous 7 days, or a urine output
rate of ≤0.5 ml/kg/h for 6 h (note that the last criterion was not
applicable in this study because of inaccurate urine output
measurement due to possible urine leakage after prostatectomy).
Statistical analysis
Differences in clinical variables between the RARP
and ORP groups were evaluated using the Mann-Whitney U test for
continuous variables and the χ2 test for categorical
variables. Correlations between clinicopathological variables and
AKI on POD0 were assessed by the χ2 test for univariate
analysis. Continuous variables were dichotomized by their median
values. All significant variables in the univariate analysis were
included in the multivariate analysis using logistic regression.
Statistical analyses were performed using JMP Pro version 14.2.0
(SAS Institute, Cary, NC, USA). P<0.05 was considered
statistically significant.
Results
Patient characteristics and
postoperative AKI
The patients' baseline characteristics are
summarized in Table I. As shown in
Fig. 1, 25 of 187 (13.4%) patients
who underwent RARP met the KDIGO's AKI criteria on POD0, while none
of the patients who underwent ORP met the criteria (Pearson's
χ2 test, P=0.001). On POD1, 3 of 187 (1.6%) patients who
underwent RARP and 2 of 70 (2.9%) patients who underwent ORP met
the criteria (P=0.517).
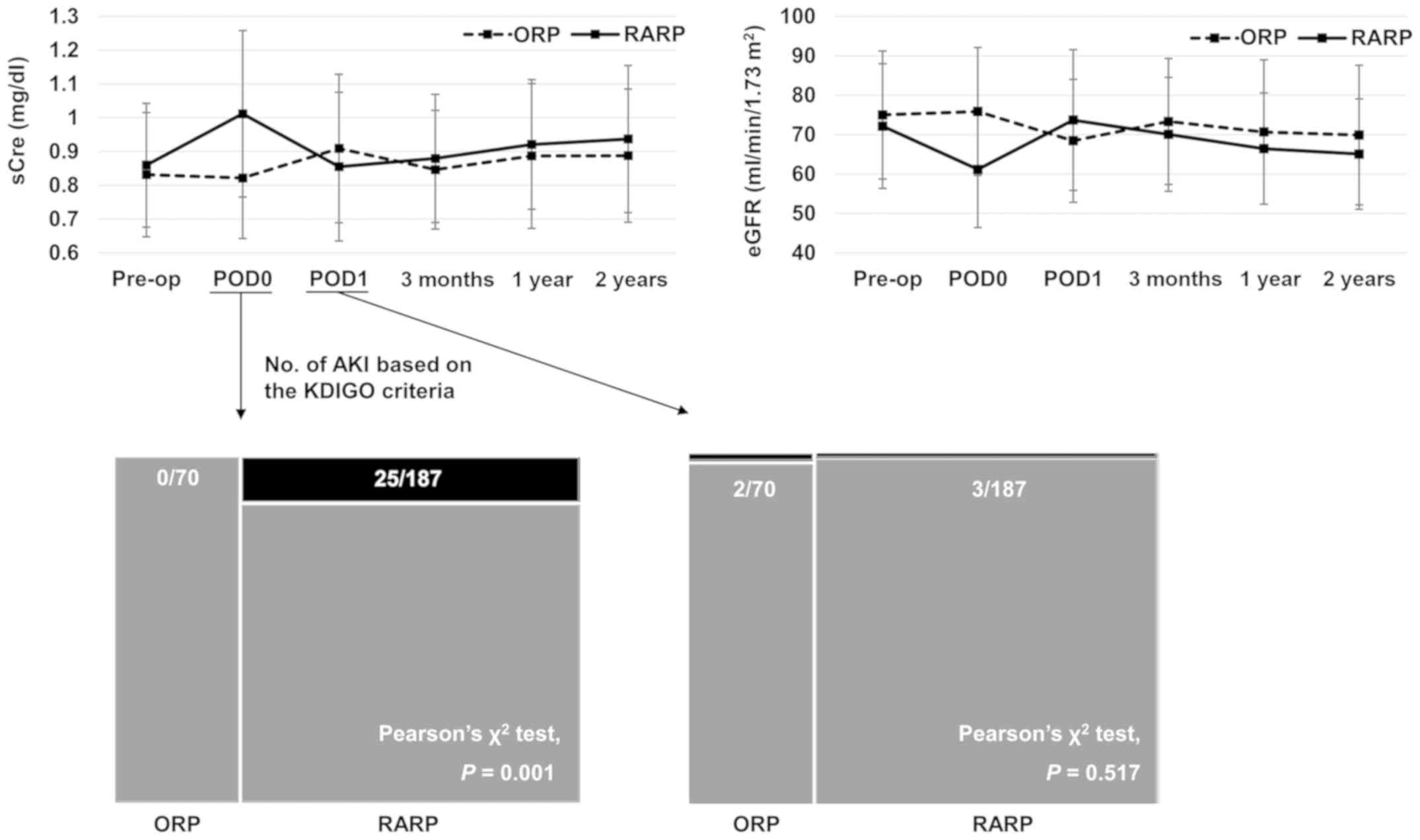 | Figure 1sCre levels in patients undergoing
RARP or ORP at the six allocated time points: Prior to surgery,
immediately after surgery (POD0), POD1, 3 months after surgery, 1
year after surgery and 2 years after surgery. The number of
patients with postoperative AKI on POD0 and POD1, based on the
KDIGO criteria, are presented. None of 70 (0%) patients with ORP
and 25 of the 187 (13.4%) patients with RARP met the KDIGO's AKI
criteria on POD0 (Pearson's χ2 test; P=0.001).
Additionally, 2 of the 70 (2.9%) patients with ORP and 3 of the 187
(1.6%) patients with RARP met the same criteria (P=0.517) on POD1.
For reference, changes in eGFR are also presented in the upper
right corner. data are presented as the mean ± standard deviation.
sCre, serum creatinine; RARP, robot-assisted radical prostatectomy;
ORP, open radical prostatectomy; POD, postoperative day; AKI, acute
kidney injury; KDIGO, Kidney Disease: Improving Global Outcomes;
eGFR, estimated glomerular filtration rate. |
 | Table IPatient baseline characteristics. |
Table I
Patient baseline characteristics.
| Variables | Total (257) | ORP (70) | RARP (187) | P-value |
|---|
| Age, years, median
(IQR) | 67 (63-71) | 67 (61-71) | 66 (63-70) | 0.898a |
| BMI,
kg/m2, median (IQR) | 24.0 (22.1-25.5) | 23.8 (21.6-25.8) | 24.1 (22.0-25.2) | 0.791a |
| Initial PSA, ng/ml,
median (IQR) | 7.6 (5.8-10.9) | 8.1 (6.0-11.8) | 7.4 (5.5-10.6) | 0.131a |
| Preoperative sCre,
mg/dl, median (IQR) | 0.82 (0.73-0.95) | 0.81 (0.70-0.90) | 0.83 (0.73-0.96) | 0.154a |
| Prostate volume, ml,
median (IQR) | 29.9 (22.4-40.3) | 32.0 (21.4-41.9) | 29.4 (22.5-40.0) | 0.581a |
| Pathological T stage,
n (%) | | | | 0.306b |
|
≤pT2 | 198 (77.0) | 57 (81.4) | 141 (75.4) | |
|
≥pT3 | 59 (23.0) | 13 (18.6) | 46 (24.6) | |
| Pathological N stage,
n (%) | | | | 0.001b,c |
|
pN0/x | 253 (98.4) | 66 (94.3) | 187(100) | |
|
pN1 | 4 (1.6) | 4 (5.7) | 0 (0) | |
| Pathological Gleason
score, n (%) | | | | 0.081b |
|
≤7 | 199 (77.4) | 49 (70.0) | 150 (80.2) | |
|
≥8 | 58 (22.6) | 21 (30.0) | 37 (19.8) | |
| Surgical time, min,
median (IQR) | 231 (199-265) | 209 (190-243) | 237 (204-271) | 0.001a,c |
| Blood loss, ml,
median (IQR) | 450 (150-865) | 1075 (728-1753) | 300 (100-500) |
<0.001a,c |
| Fluid infusion, ml,
median (IQR) | 2100 (1800-2750) | 2975 (2600-3713) | 2000 (1700-2350) |
<0.001a,c |
Long-term follow-up data of
postoperative renal function
Three months after surgery, none of the 28 patients
who met the KDIGO criteria on either POD0 or POD1 had a prolonged
significant increase in sCre, whereas 2 of 257 (0.8%) patients
(both in the RARP group) had a new increase in sCre from baseline.
One year after surgery, 5 of 257 (1.9%) patients (4 in the RARP
group and 1 in the ORP group) had a significant increase in sCre
from baseline, whereas 5 (1.9%) patients (all in the RARP group)
had a significant increase 2 years after surgery.
Correlations between
clinicopathological variables and AKI on POD0
In the univariate analysis, the procedure type (ORP
vs. RARP), initial PSA concentration (<7.55 vs. ≥7.55 ng/ml),
preoperative sCre (<0.82 vs. ≥0.82 mg/dl), pathological T stage
(≤pT2 vs. ≥pT3), and surgical time (<231 vs. ≥231 min) were
significantly associated with AKI on POD0 (Table II). The multivariate analysis
incorporating these five variables showed that performance of RARP
and a surgical time of ≥231 min were independent predictors of AKI
on POD0. However, the odds ratio for the procedure type was not
convergent because there was no event in the ORP group. Therefore,
these results might be used for reference purposes only.
| Table IIUnivariate and multivariate analyses
assessing associations between clinicopathological variables and
acute kidney injury on postoperative day 0. |
Table II
Univariate and multivariate analyses
assessing associations between clinicopathological variables and
acute kidney injury on postoperative day 0.
| | Univariate | Multivariate |
|---|
| Variables | P-value | Likelihood ratio
P-value | Odds ratio (95%
confidence interval) | Odds ratio
P-value |
| Procedure type (ORP
vs. RARP) | 0.001b |
<0.001b | Not convergent | 0.988 |
| Age (<67 vs. ≥67
yearsa) | 0.067 | | | |
| BMI (<24 vs. ≥24
kg/m2a) | 0.061 | | | |
| Initial PSA (<7.55
vs. ≥7.55 ng/mla) | 0.022b | 0.091 | 0.44 (0.16 to
1.17) | 0.099 |
| Preoperative sCre
(<0.82 vs. ≥0.82 mg/dla) | 0.044b | 0.138 | 0.48 (0.18 to
1.29) | 0.147 |
| Prostate volume
(<29.9 vs. ≥29.9 mla) | 0.541 | | | |
| Pathological T stage
(≤pT2 vs. ≥pT3) | 0.033b | 0.193 | 0.52 (0.19 to
1.38) | 0.187 |
| Pathological N stage
(0/x vs. 1) | 0.508 | | | |
| Pathological Gleason
score (≤7 vs. ≥8) | 0.494 | | | |
| Surgical time
(<231 vs. ≥231 mina) |
<0.001b | 0.002b | 0.20 (0.07 to
0.64) | 0.006b |
| Blood loss (<450
vs. ≥450 mla) | 0.115 | | | |
| Fluid infusion
(<2100 vs. ≥2100 mla) | 0.745 | | | |
Discussion
In the present study, a large number of patients who
underwent RARP met the KDIGO's AKI criteria immediately after
surgery (POD0), whereas patients who underwent ORP (control group)
did not. Nevertheless, on POD1, only a few patients in both
treatment groups met the criteria, suggesting that AKI after RARP
was just a transient phenomenon. Furthermore, the long-term
follow-up data demonstrated that only a few patients developed a
decline in renal function after surgery regardless of the procedure
type. Therefore, the transient AKI phenomenon immediately after
RARP might have little clinical significance.
The association between RARP and AKI is
controversial (2-6).
One study showed results similar to ours in that the postoperative
sCre concentration increased in patients who underwent RARP but
decreased in those who underwent ORP (2). However, another study showed a
completely opposite result; i.e., the incidence of AKI after RARP
was significantly lower than that after ORP (5). In yet other studies, postoperative
renal function was unaltered in patients who underwent RARP
(3,6). These inconsistencies might be
attributable to the diagnostic time of AKI or the timing of blood
sampling, given that fewer patients who underwent RARP than ORP in
our study met the AKI criteria on POD1 (<24 h after
surgery).
Impairment of renal function after laparoscopic
surgery has been widely reported, and the common underlying
mechanisms include increased intra-abdominal pressure and carbon
dioxide pneumoperitoneum (4,5,10).
Under conditions of pneumoperitoneum, direct compression of the
intra-abdominal vessels and renal parenchyma can decrease cardiac
output, renal blood flow, and urine output (10). These physiologic changes stimulate
the renin-angiotensin system and further decrease renal blood flow,
eventually resulting in impairment of renal function (4,5).
Additionally, the steep Trendelenburg position required for RARP
could be an additional cause of renal impairment, although the
mechanism has not been well documented (2,3). Other
possible mechanisms include pseudo-renal failure due to
intraperitoneal urine leakage during prostatectomy; however, this
may depend on the amount of leaked urine (11). We consider that in general, the
amount of leaked urine during prostatectomy is not large enough to
cause pseudo-renal failure and that the risk of pseudo-renal
failure is likely similar between RARP and ORP (Note: No patient
receiving ORP developed AKI immediately after surgery, although
there should exist a certain amount of urine leakage). Finally,
prerenal AKI can be suspected because of decreased fluid
replacement during surgery; notably, however, fluid infusion was
not associated with AKI on POD0 in the present study, even in the
univariate analysis.
In conclusion, this retrospective single-center
study revealed transient AKI immediately after RARP, but not after
ORP. However, this finding might be of little clinical significance
given the long-term follow-up data of postoperative renal function.
Nevertheless, this transient AKI phenomenon immediately after RARP
should be recognized to provide better perioperative management of
patients undergoing radical prostatectomy.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed are available from
the corresponding author on reasonable request.
Authors' contributions
AN and ST conceived and designed the present study,
analyzed and interpreted the data, and drafted the manuscript. MS
conceived, designed and supervised the study. TK, KU and TF
acquired data including patients' baseline characteristics,
perioperative factors and laboratory data. TK, KU and TF also
revised the manuscript for important intellectual content. HF and
HK supervised the study, acquired patient pre-operative data,
drafted the manuscript and were involved in revising it critically
for important intellectual content. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Internal
Institutional Review Board of Graduate School of Medicine and
Faculty of Medicine, University of Tokyo (approval no. 3124).
Written informed consent was obtained from each patient prior to
surgery. Patients were given the opportunity to decline
participation in the study through the opt-out form on our
website.
Patient consent for publication
Not applicable
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Fujimura T, Fukuhara H, Taguchi S, Yamada
Y, Sugihara T, Nakagawa T, Niimi A, Kume H, Igawa Y and Homma Y:
Robot-assisted radical prostatectomy significantly reduced
biochemical recurrence compared to retro pubic radical
prostatectomy. BMC Cancer. 17(454)2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
D'Alonzo RC, Gan TJ, Moul JW, Albala DM,
Polascik TJ, Robertson CN, Sun L, Dahm P and Habib AS: A
retrospective comparison of anesthetic management of robot-assisted
laparoscopic radical prostatectomy versus radical retropubic
prostatectomy. J Clin Anesth. 21:322–328. 2009.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Saito J, Noguchi S, Matsumoto A, Jinushi
K, Kasai T, Kudo T, Sawada M, Kimura F, Kushikata T and Hirota K:
Impact of robot-assisted laparoscopic prostatectomy on the
management of general anesthesia: Efficacy of blood withdrawal
during a steep Trendelenburg position. J Anesth. 29:487–491.
2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Li JR, Cheng CL, Weng WC, Hung SW and Yang
CR: Acute renal failure after prolonged pneumoperitoneum in
robot-assisted prostatectomy: A rare complication report. J Robot
Surg. 1:313–314. 2008.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Joo EY, Moon YJ, Yoon SH, Chin JH, Hwang
JH and Kim YK: Comparison of acute kidney injury after
robot-assisted laparoscopic radical prostatectomy versus retropubic
radical prostatectomy: A propensity score matching analysis.
Medicine (Baltimore). 95(e2650)2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Ahn JH, Lim CH, Chung HI, Choi SU, Youn SZ
and Lim HJ: Postoperative renal function in patients is unaltered
after robotic-assisted radical prostatectomy. Korean J Anesthesiol.
60:192–197. 2011.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Naito S, Kuroiwav K, Kinukawav N, Goto K,
Kogav H, Ogawa O, Murai M and Shiraishi T: Clinicopathological
Research Group For Localized Prostate Cancer Investigators.
Validation of Partin tables and development of a preoperative
nomogram for Japanese patients with clinically localized prostate
cancer using 2005 International Society of Urological Pathology
consensus on Gleason grading: Data from the clinicopathological
research group for localized prostate cancer. J Urol. 180:904–909.
2008.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Kellum JA, Lameire N, Aspelin P, Barsoum
RS, Burdmann EA, Goldstein SL, Herzog CA, Joannidis M, Kribben A,
Levey AS, et al: Kidney disease: Improving global outcomes (KDIGO)
acute kidney injury work group. KDIGO clinical practice guideline
for acute kidney injury. Kidney Int. (Suppl 2):1–138. 2012.
|
|
9
|
Doi K, Nishida O, Shigematsuv T, Sadahirov
T, Itami N, Iseki K, Yuzawa Y, Okada H, Koya D, Kiyomoto H, et al:
Japanese clinical practice guideline for acute kidney injury 2016
committee: The Japanese clinical practice guideline for acute
kidney injury 2016. Clin Exp Nephrol. 22:985–1045. 2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Wever KE, Bruintjes MH, Warlé MC and
Hooijmans CR: Renal perfusion and function during pneumoperitoneum:
A systematic review and meta-analysis of animal studies. PLoS One.
11(e0163419)2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Kruger PS and Whiteside RS: Pseudo-renal
failure following the delayed diagnosis of bladder perforation
after diagnostic laparoscopy. Anaesth Intensive Care. 31:211–213.
2003.PubMed/NCBI View Article : Google Scholar
|














